Rehabilitative Palliative Care: Scoping Review to Inform an All-Ireland Approach to Development
by Elizabeth Morrow*, Mary Lynch
Faculty of Nursing and Midwifery, Royal College of Surgeons in Ireland, University of Medicine and Health Sciences, Dublin, Ireland
*Corresponding author: Elizabeth Morrow, Senior Research Fellow, Faculty of Nursing and Midwifery, Royal College of Surgeons in Ireland, University of Medicine and Health Sciences, Dublin, Ireland. 123 St. Stephen’s Green D02 YN77 Ireland
Received Date: 06 December 2025
Accepted Date: 27 January 2026
Published Date: 30 January 2026
Citation: Morrow E, Lynch M (2026) Rehabilitative Palliative Care: Scoping Review to Inform an All-Ireland Approach to Development. Arch Palliat Care Med 7: 120. DOI: https://doi.org/10.29011/2689-9825.000120
Abstract
Rehabilitative Palliative Care (RPC) is an emerging approach in healthcare provision that seeks to maintain function, independence, and quality of life for adults with life-limiting illness. Although international interest in RPC is increasing, the evidence base to guide policy and practice remains limited. In recognition of the lack of concrete evidence, this scoping review was conducted to inform an inclusive all-Ireland approach for integrating RPC into practice. A scoping review examined the global evidence on RPC. Following the Arksey and O’Malley framework and JBI and PRISMA-ScR guidance, five databases (PubMed, CINAHL, Scopus, Web of Science, PsycINFO) were searched for literature published between 2015 and 2025 using key search terms derived from the literature. Eligible articles focused on adults receiving palliative or end-of-life care and were empirical or conceptual. Data extraction captured article type, key findings and outcomes, and implications for RPC. Articles were analysed using descriptive mapping and thematic synthesis. A total of 157 articles met the inclusion criteria. Eight themes were generated: 1) Integration of rehabilitation in palliative care and end-of-life care, 2) Outcome measures, functionality, and quality of life, 3) Interdisciplinary and team-based models 4) Person-centred care and lived experiences, 5) Professional education, training, and workforce readiness, 6) Access, equity and underrepresented groups, 7) Economic and policy considerations, 8) The impact of the COVID-19 pandemic on service delivery. Potential benefits of RPC include supporting function, autonomy, and quality of life. Gaps include inconsistent terminology, underdeveloped models of care, and limited evaluative, economic and educational research. Findings provide a foundation for future research priorities, policy development, and service planning across the island of Ireland and beyond..
Keywords: Rehabilitative palliative care; Rehabilitation; End-oflife care; Life limiting illness; Integrated care; Interprofessional care
Abbreviations: AHP: Allied Health Professional; CPD: Continuous Professional Development; DOH: Department of Health; HCP: Healthcare Professional; HEI: Higher Education Institution; HSE: Health Service Executive; IPCC: Intraprofessional Cultural Competence; MDT: Multidisciplinary Team; NI: Northern Ireland; PHW: Public Health Workforce; ROI: Republic of Ireland; RPC: Rehabilitative Palliative Care; RHP: Regulated Health Care Professional; SPC: Specialist Palliative Care; UN: United Nations; UK: United Kingdom; USA: United States of America; WHO: World Health Organization
Introduction
Rehabilitative Palliative Care (RPC) is an emerging approach in healthcare provision that seeks to maintain function, independence, and quality of life for adults with life-limiting illness [1-4]. Unlike traditional palliative care, which often prioritises symptom control and end-of-life support, RPC emphasises interventions that enable patients to live fully throughout the illness trajectory [4-6]. Central to this approach is person-centred care, recognising the diverse needs, preferences, and rights of individuals receiving palliative care, and the supportive relationship of caregivers and families [7,8].
Internationally, the World Health Organization (WHO) recognises rehabilitation and palliative care as essential components of quality health services that should be integrated within health systems using the knowledge and skills of a multi-professional workforce [9,10]. Integration of rehabilitation within palliative care can improve patient outcomes and health system efficiency, but access remains limited by resource constraints, siloed services, and professional or healthcare funder’s attitudes. While integrated rehabilitation has been implemented in high-income settings for chronic conditions or trauma, it remains under-resourced and variable within palliative care.
WHO’s 2023 policy brief highlights the potential of integrating rehabilitation in palliative care to enhance quality, accessibility, effectiveness, and cost-efficiency, offering practical guidance for health system planning [9]. The European Association for Palliative Care (EAPC) has advanced RPC across Europe through its dedicated taskforce, promoting an interdisciplinary approach that promotes patient independence and quality of life. The taskforce emphasises clear definitions, standardised delivery models, and adequate resourcing, highlighting collaboration among physiotherapists, occupational therapists, speech and language therapists, dietitians, nurses, social workers, doctors and other health professionals, to deliver holistic, person-centred care [11].
In both Northern Ireland (NI) and the Republic of Ireland (ROI) palliative care policy has increasingly recognised the importance of supporting patients with their comfort, function, independence, and quality of life. The National Clinical Programme for Palliative Care in the Republic of Ireland and the Regional Palliative Care in Partnership Board in Northern Ireland both endorse multidisciplinary person-centred palliative care as a priority. Ireland’s National Adult Palliative Care Policy focuses on developing, evaluating, and scaling models of RPC to ensure patients receive the right care tailored to their needs. However, RPC remains relatively underdeveloped in practice.
A range of influential organisations, including the National Institute for Health and Care Excellence (NICE), specialist research institutions such as the Cecilie Saunders Institute and King’s College London, and palliative care organisations such as Marie Curie, alongside professional rehabilitation bodies, have fostered multidisciplinary approaches to support function and quality of life in advanced illness. Several clinical and policy leaders have long advocated for greater all-Ireland (NI and ROI) collaboration in palliative care. Dame Judith Hill, a former Chief Nursing Officer for Northern Ireland and a founding figure in the establishment of the All-Ireland Institute of Hospice & Palliative Care (AIIHPC), has been particularly influential in promoting cross-border coordination and shared professional development.
The AIIHPC was created to support an all-Ireland approach, with leaders such as Dr Feargal Twomey, Professor Sonja McIlfatrick, and Professor Andrew Davis advancing common standards, integrated research and workforce planning, and joint policy engagement. Cross-border research structures, including the Palliative Care Research Network jointly funded by the Health Research Board (ROI) and the Public Health Agency (NI), further demonstrate sustained clinical leadership commitment to islandwide collaboration. The AIIHPC has led initiatives to advance RPC, including the seminar “Living Well with Advancing Illness – An Interdisciplinary Rehabilitative Palliative Care Approach to Patient Care” held in Dublin on 11 June 2025 and activities to develop an All-Ireland Position Paper on Rehabilitative Palliative Care, including this scoping review [12,13]. Together, these initiatives show clear professional endorsement for integrated, allIreland RPC development.
An all-Ireland approach to RPC is essential because the island’s shared geography, population identities, free movement, and comparable health challenges, demand coherent and equitable service provision across jurisdictions. Patients and families, whether they are living in NI, ROI or other countries, frequently navigate healthcare systems that often operate in isolation, creating gaps, duplication, and variability in access and quality. A coordinated, all-Ireland framework would allow for shared standards, integrated pathways, and collaborative workforce development, strengthening the capacity of both systems to deliver person-centred, rehabilitation-focused palliative care. Such alignment also enhances opportunities for joint research, knowledge exchange, and innovation, ensuring that care is informed by the best evidence and responsive to emerging needs. Ultimately, an all-Ireland approach supports more seamless, consistent, and holistic care for people with life-limiting illness, regardless of where they live.
The need for consistent and coordinated approaches to RPC are becoming more pressing due to population changes. Both the ROI and NI are experiencing significant demographic shifts characterised by an ageing population and increased longevity [14]. This trend is accompanied by a rising prevalence of multimorbidity, with two-thirds of people aged 65 and over living with multiple chronic conditions.Over 80% of those aged 85 and older affected by complex health needs [14]. These trends place increasing demand on health and social care systems, particularly in the provision of palliative care services. In ROI, projections suggest that by 2028, the number of people dying annually will increase by approximately 50%, intensifying the need for comprehensive, specialist palliative care. Similarly, NI faces a growing number of individuals living with advanced chronic or life-limiting illnesses, many requiring coordinated RPC to manage symptoms and maintain quality of life.
Aims
The aim of this scoping review was to gain a comprehensive view of the international literature on RPC, identify knowledge gaps, and highlight implications for future research, policy and service development. The justification for the review is that, although there is growing momentum from practice settings and strong drivers for RPC internationally, the evidence to inform policy and service development remains unclear. Identifying and synthesising this evidence is essential to guide research priorities, inform policy development, and strengthen clinical practice.
The intention of this paper is distinct in that it synthesises and analyses the international evidence base on RPC, whereas the full research report presents the methodological detail and findings of the project including sector consultation activities across the island of Ireland [13]. The position paper (green paper) translates these insights into concise policy and practice recommendations targeted towards these jurisdictions [12].
Methods
A systematic scoping review was conducted following the methodological frameworks originally developed by Arksey and O’Malley [15], which provides a systematic approach to mapping the existing literature in areas where concepts are complex or inconsistently defined. Their five-stage process- identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarising and reporting results- formed the foundation of this review. Scoping review methodology was considered appropriate given the evolving and interdisciplinary nature of RPC and the different terminology and models described across the literature. This methodological framework was further refined to emphasise a more iterative and reflective approach, clearer articulation of the research questions, and the importance of stakeholder consultation (described in the full report [13]) to enhance the review’s rigour and relevance [16].
The scoping review also drew on available guidance, the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) [17] and JBI (Joanna Briggs Institute) guidelines [18], ensuring a structured and transparent approach to literature identification, selection, and synthesis. Using these guidelines enhances transparency and methodological robustness in scoping reviews [18-20]. Transparency included a comprehensive search strategy with clear inclusion and exclusion criteria, and support for the inclusion of diverse evidence types (quantitative, qualitative, and grey literature) to comprehensively map key concepts, evidence sources, and gaps in knowledge.
Scope of the Review
The SPIDER tool (Sample, Phenomenon of Interest, Design, Evaluation, Research type) was used to guide the search strategy, as it is specifically designed for qualitative and mixed-methods evidence synthesis, allowing for a nuanced and flexible approach when exploring complex concepts such as RPC [21]. Searches were limited to studies involving adult populations aged 18 years and over, to ensure the review focused on RPC relevant to adult populations. This age restriction was applied because care approaches, disease trajectories, and healthcare needs often differ significantly between paediatric and adult populations, making the findings more applicable and clinically meaningful for adult services. To implement this inclusion criteria, age-related filters or keywords specifying “adult,” “aged 18 and over,” or equivalent terms were included in the search strategy across databases where possible. Additionally, studies exclusively involving children or adolescents were excluded during the screening process to maintain the review’s focus on adult care (Table 1).
|
Element |
Details |
|
Sample (S) |
Adults (aged 18 and over) receiving palliative or end-of-life care; health and social care professionals involved in palliative rehabilitation; paid and unpaid caregivers and family carers. |
|
Phenomenon of Interest (PI) |
Rehabilitative palliative care; palliative rehabilitation; functional maintenance; quality of life and independence in the context of palliative or terminal illness. |
|
Design (D) |
Qualitative studies (e.g. interviews, focus groups, ethnography); mixed-method studies; relevant quantitative designs where applicable (e.g., randomised controlled trials, quasi-experimental approaches); evaluation studies; case studies and descriptive studies where applicable. |
|
Evaluation (E) |
Outcomes, experiences and perspectives of patients and professionals; impact on quality of life, function, independence, healthcare economics, service innovation and care processes. |
|
Research Type (R) |
Qualitative, quantitative, and mixed-methods studies published in peer-reviewed literature and grey literature sources. |
Table 1: SPIDER Tool.
Research Questions
The scoping review was structured around four key research questions, developed by the research team to reflect the aims of the study:
- How is rehabilitative palliative care (RPC) defined and conceptualised in the literature?
- Why is RPC increasingly relevant in contemporary palliative care, including the context of ageing populations, chronic illness, and international policy recognition?
- What does the global evidence reveal about the implementation, outcomes, and impact of RPC for adults?
- What gaps exist in the evidence base, including issues of terminology, evaluative research, and Irish-specific data?
These questions guided all stages of the scoping review, including search strategy, study selection, and data extraction, ensuring that both breadth and depth of the literature were captured in the results.
Search Strategy
A comprehensive search of the following electronic databases was undertaken; PubMed, CINAHL, Scopus, Web of Science, and PsycINFO. Search terms included: “rehabilitative palliative care”, “palliative rehabilitation”, “functional maintenance in palliative care”, and “interdisciplinary palliative care”. Boolean operators and database-specific filters were applied to refine results and ensure relevant coverage. Full search terms and an example search is provided in Appendix 1. Search terms.
Inclusion criteria
Studies were included if they met the following criteria:
- Adult populations (18 years or older) receiving palliative care or end-of-life care
- Published between 2015 and 2025
- Published in English language (or translated to English language at publication)
- Empirical (quantitative or qualitative) or conceptual studies
Exclusion criteria
Studies were excluded if they related to:
- Paediatric, children or younger populations (under 18 years)
- Not relating to patients receiving palliative care or end-of-life care
- Published before 2015
- Not published in English language
Data extraction
Data were systematically extracted from included studies using a bespoke predefined template (Microsoft Word tables). Charting captured study characteristics including article type, design, population, intervention focus, outcomes, and key themes (see Supplementary data).
Methodological challenges
Identifying literature on RPC presented several methodological challenges. The most significant is the volume of literature that might be included in such a search. The initial searches using multiple search terms identified over 57,000 articles on PubMed alone. Due to inconsistent terminology and the lack of standardised definitions within the existing evidence base many terms exist. While terms such as “rehabilitative palliative care” and “palliative rehabilitation” are central to the topic, different terms are in use, including for example “rehabilitation in palliative care,” “interdisciplinary palliative care,” “integrated palliative and rehabilitation care,” as well as broader concepts such as “functional maintenance in palliative care” and “living well with chronic illness.” Additional terms including “terminal illness,” “life-limiting illness,” “life-limiting condition,” “hospice,” and “terminal care”. A core search string was developed to enhance specificity of the searches (Table 2).
|
Concept |
Key search term |
|
Rehabilitative palliative care |
“rehabilitative palliative care” |
|
Population group |
Adult (18+ years of age) |
|
Publication date |
Articles published between January 2015 and May 2025 |
|
Language |
Articles published in English |
Table 2: Core search string.
Screening
Systematic searches of PubMed, CINAHL, Scopus, Web of Science, and PsycINFO (2015-2025) identified 1,142 records, with an additional 63 records found through citation tracking and grey literature searching (total 1,205). After removing 463 duplicate/otherwise ineligible records, 742 records remained for title and abstract screening. Of these, 508 records were excluded as not relevant to RPC or related models. A total of 234 full-text articles were assessed for eligibility, and 77 were excluded for not meeting inclusion criteria. The final sample comprised 157 articles which were included in the analysis. Figure 1 presents the PRISMA-ScR flow diagram for the scoping review.
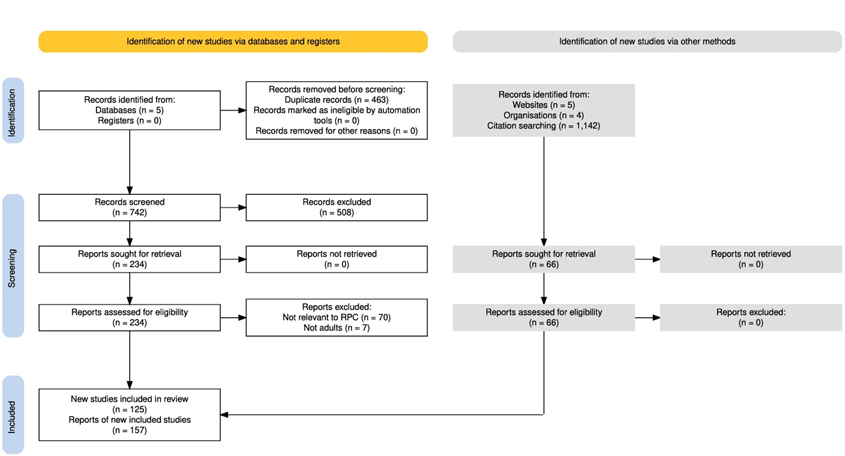
Figure 1: PRISMA-ScR Flow chart.
Analysis
The extracted data were analysed using a dual analysis approach. First, descriptive mapping provided an overview of article types, study characteristics, geographical distribution, and methodological approaches. Second, a thematic synthesis following the method described by Braun and Clarke [22], identified recurring concepts, intervention strategies, and patterns related to RPC (identifying eight key themes presented in the results). This approach allowed the review to directly address the research questions, synthesising both global trends and gaps in the evidence, to inform future research, policy, and practice [15].
Results
The results of the review are structured to provide a summary of the included literature, an overview of the key features of the global RPC literature, presentation of key themes derived from the literature, and identified gaps in the evidence.
Summary of the included literature
Article types: The search identified 157 highly relevant publications published between 2015 and 2025, encompassing peer-reviewed journal articles, policy documents, and grey literature that met all of the inclusion criteria. After screening for eligibility, the final corpus included empirical studies (qualitative, quantitative, and mixed-methods), conceptual papers, reviews, and service evaluations addressing rehabilitative palliative care (RPC) or closely related approaches (e.g. palliative rehabilitation, rehabilitation in palliative care, integrated rehabilitation–palliative models).
Place of publication (lead author affiliation): The majority of studies originated from high-income countries. The main source countries were USA=64, Denmark=20, Canada=16, UK=12, Australia=7, China=7, Germany=6, India=4, Singapore=3, Spain / Italy=2 each. One article each: Israel, Czech Republic, Ukraine, Ireland, Colombia, Scandinavia, Belgium, Switzerland, Austria. Five articles listed broader or mixed regions or “Worldwide”. Only a small number of studies were identified from the Republic of Ireland or Northern Ireland, highlighting a critical evidence gap in the all-Ireland context.
Article Types: Of the included articles 125 reported on a study. Type of study and count were: Review=42, Qualitative Study=28, Program Evaluation=17, Survey=13, Retrospective Study=11, RCT=4, Pilot Study=4, Longitudinal Study=3, Descriptive Study=2, Cross-sectional Study=1. Most included studies were qualitative or descriptive in nature, focusing on patient’s or healthcare professional’s experiences, conceptual frameworks, and service innovations. Only a limited number of evaluative or experimental studies, such as randomised controlled trials or costeffectiveness analyses, were found. Quantitative outcome data were sparse and heterogeneous, with quality-of-life and functional outcomes inconsistently measured. Settings represented across the literature included hospice, hospital, community, and homebased services, with increasing emphasis on community and home models supporting patient self-management, functional health, and independence.
Data Extracted: Tables summarising data extracted from all 157 articles are available in the full report (13). Data extracted were citation for the article, country (first author affiliation), author’s abstract, summary of key findings, and implications for RPC.
Key features across the global RPC literature
Among existing RPC frameworks, the model articulated by Tiberini and Richardson [4] is one of the most frequently referenced. Their formulation positions RPC as an approach that embeds rehabilitation, enablement, self-management, and self-care within a comprehensive palliative care philosophy. In this model, RPC is enacted through coordinated, interdisciplinary practice, with nurses, physicians, psychosocial specialists, and allied health professionals working in partnership with patients, families, and informal caregivers to support individual priorities and personally meaningful goals.
A diverse set of RPC delivery models has been documented internationally. These range from hospice-based programmes incorporating day therapy services, to inpatient and outpatient rehabilitation teams, as well as community-focused or homebased interventions [23-31]. Although the majority of studies have centred on people with cancer, research attention is expanding to include those living with non-malignant conditions- such as advanced respiratory disease, cardiac failure, and progressive neurological disorders, illustrating a broader recognition of the populations for whom RPC may be beneficial [32-35].
Evidence regarding the effectiveness of RPC is emerging but remains limited by small scale studies and methodological constraints (e.g., ethical challenges of randomisation and controlled methods). Nonetheless, recent scholarship highlights several directions for future research and development. For example, there is growing interest in applying RPC principles to older adults living with frailty and multimorbidity, as well as in the use of remote or digital rehabilitation modalities to expand accessibility [11,36-38].
Parallel to these trends is the increasing emphasis on patientreported outcome measures that reflect individualised or personal goal-oriented benefits or outcomes of RPC [24,39,40,25,4145]. Equity of access, particularly for socially marginalised or underserved groups, has also emerged as a central concern in both research and service planning for RPC [25].
Key Themes within the RPC Literature
Delving deeper into the literature, the scoping review identified several recurring themes within the included literature. These themes reflect the breadth of RPC research and highlight clinical, organisational, and experiential dimensions relevant to an allIreland approach. The themes from the literature are presented in the results section in the order of their strength in the literature, as summarised by Table 3.
Theme | Components of the theme (sub-themes) | No. of articles mentioning theme |
Integration of rehabilitation in palliative care and end-of-life care | Integration of practice or conceptual frameworks, integrated models, holistic care, service-level approaches. | 70 |
Outcomes, functionality, and quality of life | Functional outcomes, QoL, symptom burden, PROMs. | 69 |
Interdisciplinary and team-based models of care | Interdisciplinary collaboration, interdisciplinary working, team functioning, specialist-generalist interfaces. | 59 |
Person-centred care and lived experience | Patient, caregiver, and family experiences; qualitative accounts of adaptation and meaning. | 49 |
Professional education, training, and workforce readiness | Curricula, competencies, workforce capability and gaps. | 26 |
Access, equity, and underrepresented groups | Inequalities, marginalised populations, rurality, minority and underserved groups. | 23 |
Economic and policy considerations | Costs of healthcare, cost-effectiveness, resource use, return on investment. | 11 |
Impact of COVID-19 on service delivery | Disruptions, tele-rehabilitation, virtual palliative care adaptations. | 6 |
Table 3: Overview of themes derived from the literature.
Theme 1: Integration of Rehabilitation Principles in Palliative Care and End-Of-Life Care
A large and robust body of literature argues for the importance of integrating rehabilitation with palliative care to optimise quality of life for patients with life-limiting illnesses [38,46-49]. Rather than viewing rehabilitation and palliative care as distinct or sequential, many recent studies promote a model of integrated care that addresses functional, psychosocial, and symptomrelated needs simultaneously [1-3,8,24,50-56]. For example, from the United Kingdom (UK), researchers proposed an integrated rehabilitation–palliative model aiming to support individuals with advanced illness in maintaining independence and participation, even in the face of decline [53]. Similarly, Blum and colleagues [32] and Silver et al. [57] have highlighted how interdisciplinary collaboration between rehabilitation and palliative teams can foster a more person-centred approach, tailoring care plans to individual goals and trajectories.
The integration of rehabilitation principles in palliative care is not only clinically valuable but also aligns with ethical imperatives of preserving autonomy and dignity throughout the care continuum [47,58,59]. The concept of integrative care is especially relevant in managing complex chronic conditions, where standard diseasefocused approaches often fall short [41,42,60-62]. For example, in Candada, Brose et al. emphasised the role of shared decisionmaking and collaborative goal setting in rehabilitation–palliative programmes, particularly for frail older adults with multiple comorbidities [63].
From the USA, Adorno and Wallace argued that a lack of coordination between disciplines can lead to fragmented care, unmet needs, and avoidable suffering- issues that integrative models seek to resolve [59]. Also, from the USA, the work of Armstrong and Okun suggests that integrating supportive care into chronic disease management pathways (e.g., for Parkinson’s disease) can proactively address functional decline, rather than reactively responding to crisis [64]. Movement and exercise are emerging themes in this literature, supporting the call for greater integration of care across different areas of professional practice [65-68]. Together, these studies reflect a shift towards more holistic, team-based care models that are proactive, adaptive, and responsive to the needs, preferences and lived experiences of patients [34,63,69,70].
Preserving function and promoting adaptation are key aims within the RPC ethos, shifting the focus from curative treatment to enabling patients to maintain autonomy and meaningful engagement in daily life [39,54,71]. Rather than assuming inevitable decline, many contemporary models support patients in optimising their remaining abilities and adapting to new situations [58,59,63,69,70,72-78]. Accordingly, Brose et al. (2023) advocate for a goal-oriented approach where rehabilitation interventions are not only clinically appropriate but also aligned with what matters most to each individual- be it walking unaided, continuing social activities, or maintaining everyday personal routines [63]. Other evidence highlights the importance of empowering patients to develop coping strategies that address both physical and psychological challenges, thereby enhancing resilience as illness progresses [79]. However, we acknowledge that resilience is a contested concept in relation to palliative care and its use requires careful consideration in policy and practice contexts, as well as with individual patients.
Adaptation is often supported through flexible, person-centred interventions and outcomes that respond to fluctuating functional capacities [7,37,80]. For instance, from Italy Bartolo et al. (2023) discuss how neurorehabilitation strategies can be tailored for patients with advanced neurological conditions to support mobility, communication, and independence for as long as possible [26]. Rehabilitation in this context is not limited to physical goals; it includes cognitive, emotional, and environmental adaptations in a person’s surroundings as well [79,79,81].
Rehabilitative palliative care offers a new conceptual framing for healthcare. As Blum et al. (2023) and Adorno and Wallace (2017) argue,enabling participation in personally meaningful activities, even in modified form, can significantly improve patients’ sense of identity and quality of life [32,59]. This framing of function as adaptable, rather than lost, represents a vital philosophical shift in palliative care: one that fosters dignity, agency, and continuity of self, amidst progressive illness [82].
A subtheme of the included literature describes the integration of spiritual, psychosocial, and non-physical domains as part of an integrated model of care. These articles focus on the role of RPC in supporting patients through spirituality, meaning, narrative, coping with emotional distress, and nonphysical forms of suffering [83-90].
Some specific examples of integration of rehabilitative principles in palliative care or end-of-life care from the literature are as follows:
- Rehabilitative palliative care implementation: Integration of rehabilitative principles into palliative care to improve function and enablement, supported by practical tools, case examples, and training for nurses [91].
- Garden-based palliative rehabilitation for people with dementia: Nature-based palliative rehabilitation programme in nursing homes using garden spaces, developed through interdisciplinary co-design to enhance health outcomes and garden use [92].
- Evaluation tools for interdisciplinary palliative care education: Development and assessment of evaluation tools to measure interdisciplinary learning, knowledge, skills, and attitudes in palliative care teams [93].
- Community-based palliative and rehabilitation care for socioeconomically disadvantaged groups: Scoping review highlighting the need for community-focused rehabilitation and palliative care models tailored to socioeconomically disadvantaged populations, such as those experiencing homelessness [51].
- Interdisciplinary assessment and evaluation tools development: Development of comprehensive assessment tools to evaluate interdisciplinary team competency in palliative care education [1].
Theme 2: Outcome Measures, Functionality, and Quality of Life
Existing studies claim or report a variety of favourable RPC outcomes, including gains in physical functioning, such as slowing rate of decline or deconditioning, improvements in psychological wellbeing, increases in self-efficacy, and overall enhancements in Health-Related Quality of Life (HRQoL) [7,46,53,94-96]. Outcome measures include evaluating functional change, symptoms, quality of life, or rehabilitation impact [79,96-103]. Some investigations also suggest potential reductions in acute care utilisation and caregiver strain [40,75,96,104-108]. Nevertheless, much of the current literature consists of small, exploratory, or observational studies, often characterised by heterogeneous samples and challenges associated with assessing outcomes in palliative contexts [79,96-99,102].
The literature also points to gaps where outcomes are unknown. While Patient-Reported Outcome Measures (PROMs) are widely used in broader palliative care and rehabilitation research, there are few tools specifically designed or validated for capturing the functional, autonomy-focused, and person-centred outcomes central to RPC. Existing PROMs often emphasise symptom burden or overall HRQoL rather than the personalised flexible outcomes RPC seeks to achieve.
Economic evaluations are sparse, leaving commissioners with limited data on healthcare utilisation, financial outcomes or costeffectiveness [109,110]. Internationally, multiple factors have been noted to impede realisation of the benefits of RPC in routine healthcare practice. These include entrenched cultural assumptions that rehabilitation is incompatible with advanced illness, limited opportunities for interprofessional training and interprofessional cultural competence (IPC), organisational barriers to integrated care, and persistent workforce shortages, particularly among Allied Health Professionals (AHP) trained in palliative rehabilitation [44,47,77,111-115]. Resource constraints as well as unclear funding mechanisms and different commissioning structures,further contribute to the uneven availability of RPC across regions, while policy documents frequently underemphasise or omit rehabilitative approaches or their evaluation within palliative care strategies [45,116].
Theme 3: Interdisciplinary and Team-Based Models of Care
The role of interdisciplinary teamwork is increasingly recognised as a cornerstone of effective RPC [38,52,60,89,94,95,106,117-124]. High-functioning teams that bring together diverse professionals, such as psychologists, physiotherapists, occupational therapists, palliative care physicians, nurses, and social workers, connected to community care teams can provide more holistic, coordinated care that is responsive to the changing needs of patients and families [24,94,115,121,125,126]. For example, in cancer care in the USA, Bakitas and colleagues describe how interdisciplinary collaboration fosters better communication, goal alignment, and mutual respect across disciplines, such as oncology and spiritual care and social work, enhancing the overall patient experience [106]. Similarly, Blum et al. (2023) illustrate how co-located interdisciplinary teams working within integrative care models improve continuity, reduce duplication of services, and support shared decision-making [32]. This team-based approach not only enhances clinical efficiency but also ensures that the psychosocial, functional, and spiritual dimensions of care are addressed with equal importance [32,127].
Effective interdisciplinary teamwork also plays a vital role in managing complexity and uncertainty, which are inherent in life-limiting illnesses [53,128,129]. Adorno and Wallace (2017) highlight the value of collaborative dialogue in navigating ethically challenging situations, particularly when balancing patient autonomy with clinical judgement [59]. Brereton and colleagues further emphasise the need for role clarity and strong leadership within teams to enable adaptive care planning [115]. In practice, fostering successful collaboration requires dedicated time for joint case discussions, shared assessment tools, and a culture of mutual learning [37,122]. When these elements are in place, interdisciplinary teams can serve not only as a mechanism for delivering care but also as a source of emotional and professional support for the professionals themselves- an important consideration in the often emotionally demanding context of palliative rehabilitation [53,118].
Emerging models of RPC vary based on healthcare context, patient populations, and resource availability, but share the core tenets of integration, interdisciplinary teamworking, person-centredness, individualisation and flexibility of care.
- Integrated interdisciplinary models: Most RPC approaches operate within an integrated interdisciplinary framework, combining expertise from palliative medicine, rehabilitation professionals (such as physiotherapists, occupational therapists, and speech therapists), nurses, and psychosocial support staff. As highlighted by Thiel et al. (2020), integration models emphasise tailored interventions based on individual patient needs and preferences, function levels, and care settings, ranging from outpatient to inpatient environments [93]. Such models are valued for promoting coordination across disciplines, to foster more holistic patient-centred care [130].
- Community and home-based models: Communitybased models focus on extending rehabilitation and palliative principles into patient’s home environments, promoting autonomy and function outside hospital settings. Schmidt et al. (2022) demonstrated a participatory, nature-based rehabilitation programme for people with severe dementia in nursing homes, emphasising the importance of interdisciplinary collaboration and tailored interventions to enhance engagement and wellbeing [131]. These models are crucial in serving populations experiencing greater vulnerability, including those with dementia or multimorbidity, and aim to facilitate return to, or maintain, community participation [108,126].
- Oncology-specific rehabilitation frameworks: In oncology, models are often structured around clinical guidelines that endorse referral to rehabilitation services at various treatment stages [57,66]. Guidelines endorse referral pathways for cancer survivors, emphasising assessment, intervention, and ongoing management of functional impairments. These models seek to integrate rehabilitation early and proactively into cancer care pathways, improving outcomes and reducing long-term morbidity.
- Sector-spanning and systemic models: Recent developments advocate for models that transcend individual care settings, fostering systemic integration of RPC in healthcare systems [48,53,132]. An approach in Denmark exemplifies a system-oriented model where rehabilitation and palliative care are recognised as complementary components within universal health coverage [52]. These models emphasise policy support, standardised quality assurance, and collaborative networks capable of adapting to highly segmented healthcare systems. They position RPC teams as agents of change, bridging gaps between specialised services and advocating for comprehensive, equitable access [48,53].
- Innovative and emerging approaches: Emerging models incorporate novel modalities such as nature-based interventions, virtual care, and tele-rehabilitation, responding to technological advancements and diverse patient needs [133]. For instance, Schimdt et al. (2022) describe a tailored garden-based rehabilitation programme for dementia patients, reflecting innovative use of environmental and participatory strategies to promote wellbeing and functional engagement [131]. Rehabilitative interventions have been responsive to change in contexts of delivery, such as social distancing measures during COVID-19 [134].
These examples highlight the diversity of evolving RPC models and their shared core values around personalised contextually responsive approaches designed to meet the potentially complex or changing needs, preferences and rights of people with lifelimiting illness [135].
Theme 4: Person-Centred Care and Lived Experiences
Another prominent theme across the included studies is the emphasis on person-centred care and the lived experience of patients, families, and caregivers [5,58,59,69,70,72-76,78,107]. This body of work highlights the psychosocial and existential dimensions of serious illness, including meaning-making, coping, and adaptation over time. Studies in this area explore how individuals navigate changing functional abilities, negotiate identity and autonomy, and articulate their needs, preferences, and fears as illness progresses [69,123]. They also illuminate the central role of relationships, social support, and communication in shaping the experience of care, often in pressurised situations [78]. Collectively, this literature asserts the importance of recognising patients and families as active participants in RPC, whose goals, values, and lived realities should guide contextual assessment and interventions.
Caregivers and family members are recognised as playing a central role in the success of RPC, often acting as both facilitators and recipients of information, support and care [118]. As patients with life-limiting illness strive to maintain function and autonomy, the involvement of caregivers becomes crucial in supporting daily routines, aligning care with personal preferences and needs, and supporting emotional well-being. Olesen and colleagues emphasise that when caregivers are actively included in rehabilitation planning and delivery, outcomes improve not only for patients but also for the caregivers themselves- through enhanced confidence, role clarity, and reduced emotional burden [136]. Studies such as Julião et al. (2021) in Portugal, and Brose et al. (2023) further illustrate that involving families in decisions and activity adaptation helps align care with the patient’s values and capabilities, fostering a more person-centred approach.
Importantly, the literature recognises that caregiver involvement is not without challenges. Many informal carers, especially those supporting patients at home, report feeling underprepared, isolated, and physically or emotionally overwhelmed [73,108,137]. To address these issues, several studies advocate for structured caregiver support interventions- including peer support groups, online training resources, and regular check-ins from rehabilitation professionals. For instance, in Denmark, Olesen and colleagues (2022) described a hybrid rehabilitation model that incorporated virtual coaching and educational sessions for family carers, improving their capacity to assist with therapy tasks and manage stress. The emerging evidence reinforces the view that RPC models must adopt a dyadic lens- one that sees caregivers not only as helpers, but also as individuals in need of support, skillbuilding, and care in their own right.
Theme 5: Professional Education, Training and Workforce Readiness
Professional education, training and workforce readiness emerged as a key theme across the included literature, highlighting the central role of specialist competencies and interdisciplinary training in delivering high-quality RPC [93,94,120,121,138]. Studies emphasised the need for structured curricula that integrate rehabilitation principles, symptom management, communication skills, and psychosocial support, highlighting persistent gaps in pre-registration and in-service training. Research also pointed to limited workforce confidence and variable preparedness in managing functional decline, complex symptom profiles, and goal-oriented rehabilitation within palliative contexts [93,94,120,121,138]. Educational interventions, such as targeted workshops, competency frameworks, and interprofessional training models, were shown to enhance clinical capability and team-based coordination. Collectively, this body of evidence illustrates that workforce development is essential to advancing RPC at scale and ensuring consistent, person-centred practice across settings.
Theme 6: Access, Equity and Underrepresented Groups
Much of the existing literature in RPC has focused on the needs of people with cancer and other high-profile diagnoses, yet there is a growing recognition of the need to address the experiences and rights of underrepresented populations and conditions [25,60,91,139]. This includes people with physical disabilities, neurological disorders, mental health issues, people experiencing homelessness, substance use disorders, and other racialised and marginalised groups who often face barriers to accessing coordinated and dignified care [48,53,71,140,141]. For example, in the Czech Republic, Buzgová and colleagues explored the palliative needs of patients with Parkinson’s disease and dementia, emphasising the importance of early integration of rehabilitation to maintain communication and mobility as cognition declines [141]. Similarly, research has shown how individuals with progressive neurodegenerative diseases benefit from tailored, interdisciplinary interventions that respect both functional limitations and psychosocial complexities [142].
Several studies have also highlighted gaps in care for socially marginalised populations [51,60,141,143,144]. For example, Hinrichs and colleagues in the USA, examined the intersection of palliative care and homelessness, calling for adapted service models that recognise the impact of compounded vulnerabilities, such as serious mental illness [144]. Also, in the USA, Aljassem and co-authors have argued that individuals with co-occurring mental illness and substance use disorders are frequently excluded from palliative rehabilitation services, despite having significant unmet needs [60]. Meanwhile, Mittal and colleagues advocated for inclusive care pathways that acknowledge trauma histories and cultural stigma [143]. These studies collectively call attention to the structural inequities that shape health outcomes. The evidence shows the necessity for flexible, non-judgemental, inclusive models of RPC, striving for equitable models that extend rights to fairness, respect and dignity, to those often left at the margins of healthcare systems [144].
Rehabilitative palliative care has been discussed in relation to diverse populations with complex or specific illness trajectories. For example, the literature includes examples of equity relating to disease-specific rehabilitation/palliative models, for patients who have:
- Parkinson’s disease [64,145]
- Neurological disease [141,142]
- Cardiac disease [32,61]
- Lung cancer [44,108]
- Dementia [35,131]
- Hematologic/cancer rehab [16,99] • Critical illness [41,42,147]
Theme 7: Economic and Policy Considerations
As healthcare systems face increasing pressure from ageing populations and chronic illness burdens, the economic and policy dimensions of RPC have gained growing attention [38,51,53,71,109,144]. Policymakers and service commissioners are increasingly seeking evidence not only of clinical effectiveness but also of cost-efficiency and system-level value. For example, in the UK, Hughes and colleagues explored the social return on investment (SROI) in community-based palliative rehabilitation programmes, showing that relatively modest investments can yield significant improvements in patient outcomes and potential reductions in downstream costs, such as unplanned hospital admissions or prolonged institutional care [148]. In the USA, Carpenter similarly highlighted the importance of demonstrating both qualitative and quantitative outcomes to justify sustainable funding for interdisciplinary, holistic care models [149].
Despite this, many existing service models remain fragmented or under-resourced due to a lack of formal policy recognition and formal evaluation. Brereton and colleagues noted that the integration of rehabilitation within palliative pathways is often constrained by siloed funding streams and divergent commissioning priorities [115]. Moreover, the lack of standardised outcome measures and inconsistent data collection practices, presents challenges for economic evaluation at scale. Emerging evidence, advocates for policy frameworks that support interdisciplinary training, crosssector collaboration, and flexible delivery models, particularly for home- and community-based care [63].
As RPC is an evolving model, there is limited published literature focusing exclusively on its economic evaluation. However, a broader body of evidence on palliative care services- which often include rehabilitative elements- demonstrates consistent cost savings and potential cost-effectiveness [53,75,109]. Studies have shown that early hospital-based palliative care consultations can reduce healthcare costs by 9-32%, largely through shortened lengths of stay and reduced intensity of care [109]. Similarly, community-based and home palliative services have been associated with decreased hospital readmissions and emergency department use, particularly in the last months of life [150].
Despite these findings, few studies employ formal economic evaluations using metrics such as cost per Quality-Adjusted Life Year (QALY), and even fewer take a societal perspective that includes informal care costs or caregiver burden [109]. The methodological heterogeneity in existing studies also makes direct comparisons challenging. Nonetheless, the available evidence suggests that RPC- by helping patients maintain function and reduce symptom burden- has the potential to be both clinically effective and economically beneficial. Further research specifically focused on the economic impact of RPC is needed to inform policy and commissioning decisions.
Theme 8: The Impact of the COVID-19 Pandemic on Service Delivery
The COVID-19 pandemic profoundly disrupted the delivery of RPC, exposing both systemic health system vulnerabilities and opportunities for innovation [112,151-154]. One of the most significant challenges was the widespread suspension or scaling back of in-person services, particularly for patients receiving palliative or end of life care in the community or care homes [151155]. Bayly and colleagues investigated how the pandemic affected access to rehabilitation within UK palliative services, finding that physical distancing and infection control measures often led to abrupt changes in care plans, increased isolation, and reduced opportunities for functional maintenance [53]. The shift to remote or hybrid models of care, though necessary, raised concerns about digital exclusion, especially among older patients and those with cognitive or physical impairments.
At the same time, the COVID-19 pandemic served as a catalyst for accelerated service adaptation, with many teams adopting virtual multidisciplinary meetings, tele-rehabilitation sessions, and remote monitoring tools [112,152,154]. Shih and colleagues noted that while some innovations improved efficiency and extended reach, they also risked fragmenting care and weakening the therapeutic alliance between patients and professionals [154]. Moreover, the crisis highlighted pre-existing gaps in policy and infrastructure related to integrated palliative rehabilitation [134]. Many services lacked contingency plans for continuity of function-focused care during public health emergencies. The literature emerging from this period shows the need for future-proof, resilient models of care that balance flexibility with equity, ensuring that a rehabilitative ethos remain central, even during crises [151].
Gaps in the Evidence
Despite increasing recognition of the importance of RPC, several significant gaps in the current evidence base remain. First, there is a paucity of robust, high-quality research evaluating the effectiveness of different RPC models across diverse healthcare settings and patient populations. Many studies are limited by small sample sizes, observational designs, or a lack of standardised outcome measures or inclusion of negative outcomes [156]. These limitations hinder the ability to draw definitive conclusions about the impact of RPC on patient, caregiver of family outcomes. Secondly, there is a notable deficiency in validated RPC tools that can comprehensively evaluate integration, interdisciplinary learning, team collaboration, continuity of RPC, and patientcentred outcomes within specialist or general healthcare services [52,106,157]. As highlighted by findings from the research literature, existing evaluation instruments often lack standardisation, reliability, and breadth, particularly in assessing attitudes, skills, and knowledge across different healthcare professions [35,78,116]. Thirdly, research exploring patient and carer perspectives on RPC remains limited, especially regarding long-term benefits, acceptability, and cultural appropriateness of interventions. This gap restricts the development of personcentred, flexible models of care that can meet diverse individual needs [158]. In addition, there is insufficient evidence regarding the training and education of healthcare professionals involved in RPC. While some guidance exists, comprehensive curricula and competency frameworks tailored to interdisciplinary teams are lacking, which may impact the quality and consistency of care delivery [88,117,120,121,138]. Finally, economic evaluations of RPC models are scarce, making it difficult for policymakers and healthcare organisations to appraise cost-effectiveness and progress on sustainability goals [109].
Discussion
This scoping review contributes a robust and comprehensive review of the international research literature on rehabilitative palliative care.
In relation to the first research question, how is Rehabilitative Palliative Care (RPC) defined and conceptualised in the literature? this scoping review found consistent support for RPC as an integrated, interdisciplinary, and person-centred approach that promotes functionality, adaptation, and quality of life for people with life-limiting illness. Across the literature, RPC is positioned as a means of enhancing autonomy, participation, and individualised flexible support, reflecting an important evolution in contemporary palliative care practice.
Despite the promising trajectory of this emerging healthcare field, the current evidence base remains uneven and predominantly descriptive, with limited high-quality quantitative studies and notable variability in study designs, populations, and outcomes. This variability reflects a broader conceptual ambiguity: definitions of RPC, and the extent to which rehabilitation and palliative care principles are operationally integrated, remain inconsistent across the literature. As such, the development of unified terminology, identification of core principles, standardised outcome measures, and shared practice frameworks is essential to enable comparison, replication, and scalability.
In relation to the second research question, Why is RPC increasingly relevant in contemporary palliative care, including the context of ageing populations, chronic illness, and international policy recognition? the findings of this review align with emerging international guidance, including WHO (2023) recommendations emphasising early, integrated, and function-supporting models of palliative care, and the EAPC’s (2025) call for interdisciplinary, rehabilitative, and person-centred approaches. These frameworks similarly advocate for preserving function, supporting selfmanagement, and enhancing quality of life through coordinated, holistic care, thereby reinforcing RPC’s relevance within international policy discourse [9]. Across the island of Ireland, RPC can contribute to major health-system reform agendas, including Sláintecare’s emphasis on integrated, community-based care and the growing policy momentum behind compassionate communities and public health approaches to palliative care [159,160].
In relation to the third research question, what does the global evidence reveal about the implementation, outcomes, and impact of RPC for adults? advancing the field will require greater conceptual clarity, rigorous evaluation of service models, investment in workforce capacity, and a more robust empirical foundation to support equitable, large-scale implementation. Implications for development of an all-Ireland approach to RPC are discussed below.
Implications for Development of an all-Ireland Approach to RPC
Across the themes and findings of this review, six key implications emerge. Figure 2 illustrates how these implications can inform the future development of RPC.
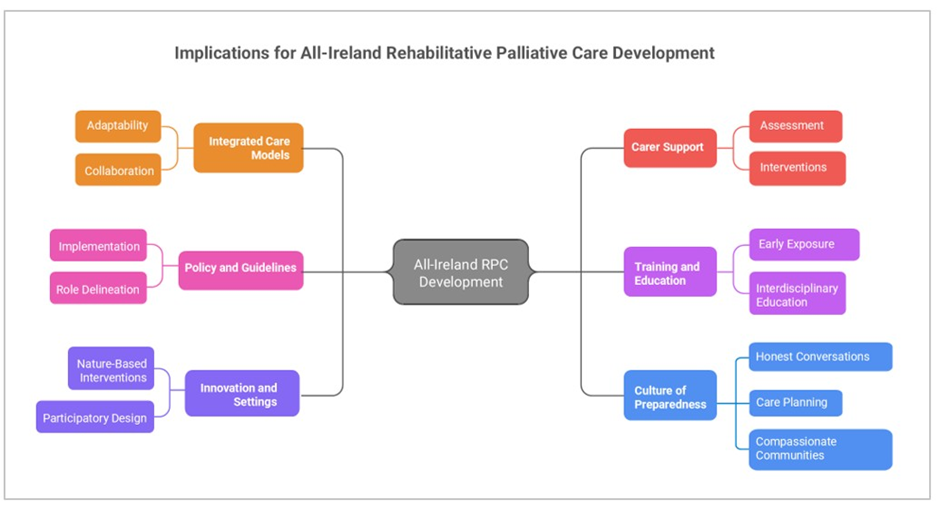
The main implications are as follows:
- Integrated care models: Effective RPC must function within highly specialised and segmented health systems across territories, requiring adaptability, collaboration, and clear delineation of roles among professionals and providers. Systematic reviews of studies on rehabilitation and palliative care emphasise the importance of models that combine specialties with models to comprehensively address complex patient needs and promote systemic change [53,60,61]. These models can act as catalysts for change, bridging gaps between services and fostering integrated care pathways.
- Policy and guideline development: Recognition of rehabilitation as an integral component of oncology and palliative care, despite underutilisation, suggests that improved implementation strategies are needed to translate guideline recommendations into practice [1,161]. Establishing shared quality standards and clearer role delineation can promote consistent, guideline-concordant care, ultimately enhancing functional/ adaption outcomes and health-related quality of life [98,161,162].
- Innovative settings and approaches: Nature-based interventions, such as garden-based programmes, exemplify personalised, resource-efficient methods to promote well-being and neuropsychiatric stability in vulnerable populations such as dementia patients. Participatory, human-centred interdisciplinary design ensures relevance, sustainability, and acceptability among patients and their families [66,131,163]. These approaches assert the importance of addressing holistic needs through creative, therapeutic environments.
- Supporting carers as part of the care team: Routine assessment and documentation of carer burden, alongside tailored educational interventions, can bolster resilience and improve social and psychological outcomes for families. Implementing structured, interdisciplinary carer support programmes, including psycho-social and educational components, is essential for a truly holistic approach to patient care [91,154,164]. Evidence indicates that carer well-being directly impacts patient outcomes, emphasising the need for comprehensive support that extends beyond the patient [165].
- Training and education: Healthcare curricula should incorporate early exposure to end-of-life communication, interaction, and rehabilitative principles, since adequate training correlates with increased confidence and competence in providing RPC [91,93,166]. Implementing competency-based, interdisciplinary education programmes helps prepare providers to navigate complex, multimorbid cases such as those involving endstage renal disease and stroke, which require coordinated, patientcentred interventions.
- Promoting a culture of preparedness: Creating a care culture that openly discusses death, dying, and end-of-life preferences facilitates honest conversations and enhances care planning, thereby establishing a solid foundation for effective RPC [93,129]. Fostering such a culture can improve patient autonomy, dignity, and the quality of the end-of-life experience.
Future Research
In relation to the fourth research question, What gaps exist in the evidence base, including issues of terminology, evaluative research, and Irish-specific data? three major evidence gaps are 1) Evaluative and economic research: Few studies measured outcomes using validated scales or included cost-effectiveness analyses. 2) Geographic representation: Minimal evidence from Ireland and from low- or middle-income countries limits generalisability. 3) Implementation science: Limited examination of how RPC can be scaled sustainably, integrated into national frameworks, or aligned with system reforms such as Sláintecare in ROI and community-based care strategies. Addressing these gaps through rigorous research, standardisation of measurement tools, and inclusion of diverse patient and professional perspectives is essential to advance the field and ensure the delivery of highquality, equitable RPC.
Limitations
This review has several limitations that should be acknowledged. The search was restricted to English-language publications, which may have excluded relevant evidence from non-English-speaking regions and contributed to a degree of country and cultural bias. Much of the included literature was small-scale, exploratory, or qualitative in nature, limiting the strength of empirical conclusions and reducing the generalisability of findings.
The lack of consistent definitions and the overlapping use of terminology across disciplines may have led to the omission of relevant studies. Additionally, interdisciplinary and interprofessional roles are often under-described or inconsistently labelled in the literature, which may have limited the identification of evidence specifically addressing team-based rehabilitative care within palliative contexts. It was not feasible to screen tens of thousands of articles by their titles or abstracts. Thus, a much more focused search strategy was necessary, using specific search terms to identify the most relevant and recent articles on rehabilitative palliative care.
Quantitative evidence fromrobust trials, economic evaluations, and longitudinal outcome studies, remains limited within RPC. Additionally, considerable conceptual variability was observed across studies, with inconsistent definitions and operationalisation of RPC, making comparison and synthesis challenging. These limitations highlight the need for clearer conceptual frameworks and more rigorous, internationally diverse research to advance understanding and implementation of RPC.
Conclusion
This scoping review has found that rehabilitative palliative care is supported by a conceptually robust foundation, with strong consensus across the literature on the importance of integration, interdisciplinary and team-based care, and person-centred approaches that are responsive to the lived experiences of patients, families, and caregivers. Evidence indicates that RPC can enhance functional ability, support adaptation, and improve quality of life, reinforcing its value within contemporary palliative care practice. However, local evidence on population needs, assessment practices, professional education and training, carer support and effective implementation strategies remains limited, particularly across regions or nations such as the island of Ireland. To advance the field, future research should prioritise rigorous evaluation of RPC’s effectiveness, cost implications, and patient-reported outcomes, ensuring that service development is both evidenceinformed and responsive to the diverse needs of communities.
Acknowledgements
The research was initiated and commissioned by the All-Ireland Institute of Hospice and Palliative Care (AIIHPC). AIIHPC is a leading organisation with national and international influence promoting excellence in palliative care. AIIHPC is a collaborative of hospices, health and social care organisations, charities and universities on the island of Ireland. As the palliative care sector’s institute, AIIHPC is involving service users, carers and communities in palliative care delivery and development, working to integrate palliative care across the health system so people are supported as early as possible, supporting the development of specialist palliative care services for everyone who needs them. This study of RPC was initiated and commissioned by Karen Charnley, Chief Executive Officer, AIIHPC and Melanie Nugent, Programme Manager for Education and Practice, AIIHPC. Members of the Steering Group contributed knowledge and expertise to inform the project design and development of the position paper: Karen Charnley, AIIHPC, Melanie Nugent, AIIHPC, Martina O’Reilly, HSE National Clinical Programme for Palliative Care, Lisa McGirr, St Francis Hospice Dublin, Niamh Donnelly, St Francis Hospice Dublin. Prof Fiona Ross CBE, Professor Emerita Health and Social Care, Kingston University, former Chair of Princess Alice Hospice, former Chair of Hospice UK Chairs Forum for London Hospices, Trustee Great Ormond Street Hospital Charity, provided expert advice to the research team. We thank all those who gave their time and contributed policy and practice insights to the project.
Funder
Funding for the research was provided by the Health Service Executive in the Republic of Ireland and the Public Health Agency in Northern Ireland.
Conflict of Interest
The authors declare no conflict of interest.
Supplementary Data
All of the data used in the paper is available in the full research report [13].
References
- Tiberini R, Hayes A (2024) How to adopt a rehabilitative palliative care approach. Nursing Times.
- Montagnini M, Javier NM, Mitchinson A (2020) The Role of Rehabilitation in Patients Receiving Hospice and Palliative Care. Rehabil Oncol 38: 9-21.
- Wilson C (2019) Rehabilitation Services and Palliative Care: An Oxymoron or Best Practice? Home Healthc Now 37: 174-175.
- Tiberini R, Richardson H (2015) Rehabilitative Palliative Care: Enabling People to Live Fully Until They Die. Hospice UK. London: Hospice UK; 2015. Report No.: ISBN 978-1-871978-91-9.
- Wæhrens EE, Brandt Å, Peoples H, Cour K (2020) Everyday activities when living at home with advanced cancer: A cross-sectional study. Eur J Cancer Care (Engl) 29: e13258.
- Radbruch L, De Lima L, Knaul F, Wenk R, Ali Z, et al. (2020) Redefining Palliative Care-A New Consensus-Based Definition. J Pain Symptom Manage 60: 754-764.
- Bradshaw A, Santarelli M, Mulderrig M, Khamis A, Sartain K, et al. (2021) Implementing person-centred outcome measures in palliative care: An exploratory qualitative study using Normalisation Process Theory to understand processes and context. Palliat Med 35: 397-407.
- Ramanjulu R (2020) Palliative rehabilitation: The essence of personalized care. Indian J Palliat Care 26: 399-400.
- World Health Organization (2023) Policy Brief on Integrating Rehabilitation into Palliative Care Services. Copenhagen: WHO Regional Office for Europe.
- World Health Organization (2020) Palliative Care.
- Van Den Block L, De Nooijer K, Pautex S, Pivodic L, Van Den Noortgate N, et al. (2025) A European Association for Palliative Care White Paper defining an integrative palliative, geriatric, and rehabilitative approach to care and support for older people living with frailty and their family carers: a 28-country Delphi study and recommendations. EClinicalMedicine 87: 103403.
- Morrow E, Lynch M (2025) All Ireland position paper on rehabilitative palliative care: green paper November 2025. Royal College of Surgeons in Ireland p. 518058 Bytes.
- Morrow E, Lynch M (2025) Rehabilitative palliative care - evidence to inform an all-Ireland position paper. Royal College of Surgeons in Ireland; p. 4276818 Bytes.
- Central Statistics Office (2023) Central Statistics Office System of Health Accounts.
- Arksey H, O’Malley L (2005) Scoping studies: towards a methodological framework. Int J Soc Res Methodol 8: 19-32.
- Levac D, Colquhoun H, O’Brien KK (2010) Scoping studies: advancing the methodology. Implement Sci 5: 69.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, et al. (2018) PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med 169: 467-473.
- Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z (2024) JBI Manual for Evidence Synthesis. JBI.
- Peters MDJ, Marnie C, Tricco AC, Pollock D, Munn Z, et al. (2021) Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth 18: 2119-2126.
- Peters MDJ, Godfrey C, McInerney P, Khalil H, Larsen P, et al. (2022) Best practice guidance and reporting items for the development of scoping review protocols. JBI Evid Synth 20: 953-968.
- Cooke A, Smith D, Booth A (2012) Beyond PICO: The SPIDER Tool for Qualitative Evidence Synthesis. Qual Health Res 22: 1435-1443.
- Clarke V, Braun V (2017) Thematic analysis. J Posit Psychol 12: 297298.
- Manson J (2025) What is the ideal model of adult community palliative rehabilitation - a realist review. Physiotherapy 126: 101683.
- Manson J, Taylor P, Mawson S, Bayly J, Keen C, et al. (2025) Identifying aspects of physiotherapy and occupational therapy provision in community palliative rehabilitation that could improve outcomes: A realist review. Palliat Med 39: 734-749.
- Preston G, Rampes S, Bayly J, Rice HT, Angelova R, et al. (2023) Using volunteers to improve access to community rehabilitation in palliative care: the St Christopher’s Living Well at Home Team. Front Rehabil Sci 4: 1229442.
- Bartolo M, Intiso D, Zucchella C (2023) Neurorehabilitation in brain tumours: evidences and suggestions for spreading of knowledge and research implementation. Curr Opin Oncol 35: 543-549.
- Chan HYL, Chung CKM, Tam SSC, Chow RSK (2021) Community palliative care services on addressing physical and psychosocial needs in people with advanced illness: a prospective cohort study. BMC Palliat Care 20: 143.
- Hasegawa T, Akechi T, Osaga S, Tsuji T, Okuyama T, et al. (2021) Unmet need for palliative rehabilitation in inpatient hospices/palliative care units: a nationwide post-bereavement survey. Jpn J Clin Oncol 51: 1334-1338.
- Hasegawa T, Sekine R, Akechi T, Osaga S, Tsuji T, et al. (2020) Rehabilitation for Cancer Patients in Inpatient Hospices/Palliative Care Units and Achievement of a Good Death: Analyses of Combined Data from Nationwide Surveys Among Bereaved Family Members. J Pain Symptom Manage 60: 1163-1169.
- Krill MK, Fogarty AE, Jacob S (2020) A 71-year-old man with a rare rhabdoid brain tumour: using a multidisciplinary medical and rehabilitative model of care. BMJ Case Rep 3: e231924.
- von Waldegg G, Pfisterer M (2019) Palliative needs of geriatric patients. Dtsch Med Wochenschr 144: 1686-1690.
- Blum M, Beasley A, Ikejiani D, Goldstein NE, Bakitas MA, et al. (2023) Building a Cardiac Palliative Care Program: A Qualitative Study of the Experiences of Ten Program Leaders from Across the United States. J Pain Symptom Manage 66: 62-69.e5.
- LaMarca A, Tse I, Keysor J (2023) Rehabilitation Technologies for Chronic Conditions: Will We Sink or Swim? Healthcare 11: 2751.
- Seng AWP, Tham SL (2022) Palliative rehabilitation in end-stage renal failure. Ren Replace Ther 8: 53.
- Laver K, Crotty M, Low L, Clemson L, Whitehead C, et al. (2020) Rehabilitation for people with dementia: a multi-method study examining knowledge and attitudes. BMC Geriatr 20: 531.
- Kunz R (2024) Characteristics of palliative care in the elderly. Ther Umsch 81: 107-114.
- Van den Noortgate N, Van den Block L (2022) End-of-life care for older people: the way forward. Age Ageing 51: afac078.
- Li YR, Anderson E, Ingelson B, Noorizadeh K (2017) Interdisciplinary palliative care services for cancer patients: Assessing quality of care and outcomes measures of successful intervention. J Clin Oncol 35: 127.
- Hwee Heng CS (2024) Collaborative goal setting in palliative rehabilitation: a case report. BMC Palliat Care 23: 179.
- Ibrahim AM, Wahba NMI, Zaghamir DEF, Mersal NA, Mersal FA, et al. (2024) Impact of a comprehensive rehabilitation palliative care program on the quality of life of patients with terminal cancer and their informal caregivers: a quasi-experimental study. BMC Nurs 23: 357.
- Finn A, Selvaraj V, Peterson E, Banerjee D, Lal A, et al. (2022) Management of the Patient with Chronic Critical Illness Part 1. J COMMUNITY Hosp Intern Med Perspect 12: 28-33.
- Finn A, Selvaraj V, Peterson E, Banerjee D, Lal A, et al. (2022) Management of the Patient with Chronic Critical Illness Part 2. J Community Hosp Intern Med Perspect 12: 6-10.
- Westermair A, Buchman D, Levitt S, Perrar K, Trachsel M (2022) Palliative psychiatry in a narrow and in a broad sense: A concept clarification. Aust N Z J Psychiatry 56: 1535-1541.
- Payne C, McIlfatrick S, Larkin P, Dunwoody L, Gracey J (2018) A qualitative exploration of patient and healthcare professionals’ views and experiences of palliative rehabilitation during advanced lung cancer treatment. Palliat Med 32: 1624-1632.
- Mills K, Payne A (2015) Enabling occupation at the end of life: A literature review. Palliat Support CARE 13: 1755-1769.
- Pryde K, Lakhani A, William L, Dennett A (2024) Palliative rehabilitation and quality of life: systematic review and meta-analysis. BMJ Support Palliat Care spcare-2024-004972.
- Chung RYN, Dong D, Chau NNS, Chau PYK, Yeoh EK, et al. (2020) Examining the Gaps and Issues of End-of-Life Care among Older Population through the Lens of Socioecological Model—A MultiMethod Qualitative Study of Hong Kong. Int J Environ Res Public Health 17: 5072.
- Leung DYP, Chan HYL (2020) Palliative and End-of-Life Care: More Work is Required. Int J Environ Res Public Health 17: 7429.
- Carpenter J, Berry P, Ersek M (2017) Nursing home care trajectories for older adults following in-hospital palliative care consultation. Geriatr Nur (Lond) 38: 531-536.
- Rezende G, Gomes-Ferraz CA, Bacon IGFI, De Carlo MMRDP (2023) The importance of a continuum of rehabilitation from diagnosis of advanced cancer to palliative care. Disabil Rehabil 45: 3978-3988.
- Pilegaard MS, Rossau HK, Lejsgaard E, Kjer Møller JJ, Jarlbaek L, et al. (2021) Rehabilitation and palliative care for socioeconomically disadvantaged patients with advanced cancer: a scoping review. Acta Oncol 60: 112-123.
- Nottelmann L, Groenvold M, Vejlgaard TB, Petersen MA, Jensen LH (2021) Early, integrated palliative rehabilitation improves quality of life of patients with newly diagnosed advanced cancer: The Pal-Rehab randomized controlled trial. Palliat Med 35: 1344-1355.
- Bayly J, Ahmedzai HH, Blandini MG, Bressi B, Caraceni AT, et al. (2023) Integrated Short-term Palliative Rehabilitation to improve quality of life and equitable care access in incurable cancer (INSPIRE): a multinational European research project. Palliat Care Soc Pract 17: 26323524231179979.
- Cheville AL, Morrow M, Smith SR, Basford JR (2017) Integrating Function-Directed Treatments into Palliative Care. PM&R 9: S335-S346.
- Javier NM, Montagnini M (2018) The Role of Palliative Rehabilitation in Serious Illness #364. J Palliat Med 21: 1808-1809.
- Barawid E, Covarrubias N, Tribuzio B, Liao S (2015) The Benefits of Rehabilitation for Palliative Care Patients. Am J Hosp Palliat Med 32: 34-43.
- Silver JK, Raj VS, Fu JB, Wisotzky EM, Smith SR, et al. (2015) Cancer rehabilitation and palliative care: critical components in the delivery of high-quality oncology services. Support Care Cancer 23: 3633-3643.
- Arantzamendi M, García-Rueda N, Carvajal A, Robinson CA (2020) People with Advanced Cancer: The Process of Living Well with Awareness of Dying. Qual Health Res 30: 1143-1155.
- Adorno G, Wallace C (2017) Preparation for the end of life and life completion during late-stage lung cancer: An exploratory analysis. Palliat Support Care 15: 554-564.
- Aljassem A, Spickler M, Kapur N (2024) A path to recovery for overlooked populations and their unique challenges: integrating rehabilitation in palliative care for patients with substance use disorders. Front Rehabil Sci 5: 1373857.
- Bierle RS, Vuckovic KM, Ryan CJ (2021) Integrating Palliative Care Into Heart Failure Management. Crit Care Nurse 41: e9-e18.
- Levy C, Balogh S, Perkins E (2016) Realizing the Potential of Rehabilitative Care for People with Complex Health Conditions: The Time Is Now. Healthc Q 19: 49-54.
- Brose JM, Willis E, Morgan DD (2023) The intentional pursuit of everyday life while dying: A longitudinal qualitative study of workingaged adults living with advanced cancer. Palliat Med 37: 1210-1221.
- Armstrong M, Okun M (20202) Diagnosis and Treatment of Parkinson Disease A Review. JAMA 323: 548-560.
- Chang PJ, Hendifar AE, Gresham G, Ngo-Huang A, Oberstein PE, et al. (2025) Exercise Guidelines in Pancreatic Cancer Based on the Dietz Model. Cancers 17: 630.
- Stout N, Santa Mina D, Lyons K, Robb K, Silver J (2021) A systematic review of rehabilitation and exercise recommendations in oncology guidelines. CA- Cancer J Clin 71: 149-175.
- Hart N, Galvao D, Newton R (2017) Exercise medicine for advanced prostate cancer. Curr Opin Support Palliat Care 11: 247-257.
- Malcolm L, Mein G, Jones A, Talbot-Rice H, Maddocks M, et al. (2016) Strength in numbers: patient experiences of group exercise within hospice palliative care. BMC Palliat Care 15: 97.
- Brose JM, Willis E, Morgan DD (2024) Occupational adaptation for adults living with advanced cancer: A phenomenological longitudinal study. Aust Occup Ther J 71: 52-63.
- Robinson CA (2017) Families Living Well With Chronic Illness: The Healing Process of Moving On. Qual Health Res 27: 447-461.
- Rubin M, Lewis A, Creutzfeldt C, Shrestha G, Boyle Q, et al. (2024) Equity in Clinical Care and Research Involving Persons with Disorders of Consciousness. Neurocrit Care 41: 345-356.
- Avery J, Mosher PJ, Kassam A, Srikanthan A, D’Agostino N, et al. (2020) Young Adult Experience in an Outpatient Interdisciplinary Palliative Care Cancer Clinic. JCO Oncol Pract 16: e1451-e1461.
- Daly S, Samson A, Gazzola N, Moreau K, Tucker T, et al. (2018) Family Caregiver Experiences: A Case Study of Caregiving for an Advanced Cancer Patient Enrolled in a Palliative Rehabilitation Program. J Pain Symptom Manage 56: e90-e91.
- Henry M, Bdira A, Cherba M, Lambert S, Carnevale F, et al. (2016) Recovering function and surviving treatments are primary motivators for health behavior change in patients with head and neck cancer: Qualitative focus group study. Palliat Support Care 14: 364-375.
- Olesen LK, La Cour K, With H, Mahoney AF, Handberg C (2022) A cross-sectional evaluation of acceptability of an online palliative rehabilitation program for family caregivers of people with amyotrophic lateral sclerosis and cognitive and behavioral impairments. BMC Health Serv Res 22: 697.
- Reina-Gamba NC, Medellin-Olaya J, Burbano-Rivera DV, MirandaRojas HM, Vargas-Escobar LM, et al. (2022) Health-Related Quality of Life in Primary Caregivers of People Receiving Palliative Home Care. J Hosp Palliat Nurs 24: E41-E47.
- Cerni J, Rhee J, Hosseinzadeh H (2020) End-of-Life Cancer Care Resource Utilisation in Rural Versus Urban Settings: A Systematic Review. Int J Environ Res Public Health 17: 4955.
- Runacres F, Gregory H, Ugalde A (2017) ‘The horse has bolted I suspect’: A qualitative study of clinicians’ attitudes and perceptions regarding palliative rehabilitation. Palliat Med 31: 642-650.
- Feldstain A, Lebel S, Chasen MR (2016) An interdisciplinary palliative rehabilitation intervention bolstering general self-efficacy to attenuate symptoms of depression in patients living with advanced cancer. Support Care Cancer 24: 109-117.
- Cour KL, Oestergaard LG, Pilegaard MS (2025) Everyday activity strategies perceived by people with advanced cancer: a qualitative explorative study. BMC Palliat Care 24: 30.
- Julião M, Chochinov HM, Samorinha C, Da Silva Soares D, Antunes B (2021) Prevalence and Factors Associated with Will-to-Live in Patients with Advanced Disease: Results From a Portuguese Retrospective Study. J Pain Symptom Manage 62: 820-827.
- Patel B, Raj V, Mitchell C, Rathore FA (2023) A Brief Review of Inpatient Palliative Rehabilitation. J Pak Med Assoc 73: 2501-2504.
- Rattner M, Cait CA (2024) Nonphysical Suffering: An Under-Resourced and Key Role for Hospice and Palliative Care Social Workers. J Soc Work End--Life Palliat Care 20: 8-25.
- McCann Klug L (2023) The Specialty Chaplain on the Palliative Care Team: A Narrative Review. Am J Hosp Palliat Med 40: 1021-1028.
- Roikjær S, Gärtner H, Timm H (2022) Use of narrative methods in rehabilitation and palliative care in Scandinavian countries: A scoping review. Scand J Caring Sci 36: 346-381.
- Ronald AH, Hooper LM, Head BA, Evans-Andris M, Estes EO (2020) Insights and experiences of chaplain interns and social work interns on palliative care teams. Death Stud 44: 141-151.
- Johnson R, Hauser J, Emanuel L (2021) Toward a clinical model for patient spiritual journeys in supportive and palliative care: Testing a concept of human spirituality and associated recursive states. Palliat Support Care 19: 28-33.
- Puchalski C, Jafari N, Buller H, Haythorn T, Jacobs C, et al. (2020) Interprofessional Spiritual Care Education Curriculum: A Milestone toward the Provision of Spiritual Care. J Palliat Med 23: 777-784.
- Blinderman CD, Schapiro AB (2016) Integrating contemplative and spiritual care in outpatient palliative care: A pilot study. J Clin Oncol 34: 247.
- Massey K, Barnes MJ, Villines D, Goldstein JD, Pierson ALH, et al. (2015) What do I do? Developing a taxonomy of chaplaincy activities and interventions for spiritual care in intensive care unit palliative care. BMC Palliat Care 14: 10.
- Timm H, Thuesen J, Clark D (2021) Rehabilitation and palliative care: histories, dialectics and challenges. Wellcome Open Res 6: 171.
- Schmit JM, Meyer LE, Duff JM, Dai Y, Zou F, et al. (2016) Perspectives on death and dying: a study of resident comfort with End-of-life care. BMC Med Educ 16: 297.
- Thiel M, Harden K, Brazier LJ, Marks AD, Smith MA (2020) Evaluation Tools for Interdisciplinary Palliative Care Learning Experiences: A Literature Review. J Palliat Med 23: 698-702.
- Henshaw AM, Winstead SR (2024) Building Bridges in Palliative Rehabilitation: An Evidence-Based Toolkit to Promote Collaboration. Am J Hosp Palliat Med 41: 601-609.
- Isenberg SR, Aslakson RA, Smith TJ (2017) Implementing EvidenceBased Palliative Care Programs and Policy for Cancer Patients: Epidemiologic and Policy Implications of the 2016 American Society of Clinical Oncology Clinical Practice Guideline Update. Epidemiol Rev 39: 123-131.
- Piil K, Juhler M, Jakobsen J, Jarden M (2016) Controlled rehabilitative and supportive care intervention trials in patients with high-grade gliomas and their caregivers: a systematic review. BMJ Support Palliat Care 6: 27-34.
- Tennison JM, Fu JB, Hui D (2024) Palliative Rehabilitation in Patients with Cancer: Definitions, Structures, Processes and Outcomes. Curr Oncol Rep 26: 1283-1292.
- Mah K, Chow B, Swami N, Pope A, Rydall A, et al. (2023) Early palliative care and quality of dying and death in patients with advanced cancer. BMJ Support Palliat Care 13: e74-e77.
- Bilek AJ, Borodin O, Carmi L, Yakim A, Shtern M, et al. (2021) Older patients with active cancer have favorable inpatient rehabilitation outcomes. J Geriatr Oncol 12: 799-807.
- Nottelmann L, Groenvold M, Petersen MA, Vejlgaard T, Jensen LH (2018) A single-center randomized clinical trial of palliative rehabilitation versus standard care alone in patients with newly diagnosed nonresectable cancer. J Clin Oncol 36: 75.
- Nottelmann L, Groenvold M, Vejlgaard TB, Petersen MA, Jensen LH (2017) A parallel-group randomized clinical trial of individually tailored, multidisciplinary, palliative rehabilitation for patients with newly diagnosed advanced cancer: the Pal-Rehab study protocol. BMC Cancer 17: 560.
- Feldstain A, MacDonald N, Bhargava R, Chasen M (2017) Reported distress in patients living with advanced cancer: changes pre-post interdisciplinary palliative rehabilitation. Support Care Cancer 25: 3191-3197.
- McMurray J, McNeil H, Lafortune C, Black S, Prorok J, et al. (2016) Measuring Patients’ Experience of Rehabilitation Services Across the Care Continuum. Part I: A Systematic Review of the Literature. Arch Phys Med Rehabil 97 104-120.
- Nordentoft S, Dieperink KB, Johansson SD, Jarden M, Piil K (2022) Evaluation of a multimodal rehabilitative palliative care programme for patients with high-grade glioma and their family caregivers. Scand J Caring Sci 36: 815-829.
- Giammalva G, Iacopino D, Azzarello G, Gaggiotti C, Graziano F, et al. (2018) End-of-Life Care in High-Grade Glioma Patients. The Palliative and Supportive Perspective. Brain Sci 8: 125.
- Bakitas MA, El-Jawahri A, Farquhar M, Ferrell B, Grudzen C, et al. (2017) The TEAM Approach to Improving Oncology Outcomes by Incorporating Palliative Care in Practice. J Oncol Pract 13: 557-566.
- Kavalieratos D, Corbelli J, Zhang D, Dionne-Odom JN, Ernecoff NC, et al. (2016) Association Between Palliative Care and Patient and Caregiver Outcomes: A Systematic Review and Meta-analysis. JAMA 316: 2104-2114.
- Sun V, Grant M, Koczywas M, Freeman B, Zachariah F, et al. (2015) Effectiveness of an interdisciplinary palliative care intervention for family caregivers in lung cancer. Cancer 121: 3737-3745.
- Parackal A, Ramamoorthi K, Tarride JE (2022) Economic Evaluation of Palliative Care Interventions: A Review of the Evolution of Methods From 2011 to 2019. Am J Hosp Palliat Med 39: 108-122.
- Neo HY, Yap CW, Teo LM, Lee LT, Tan HW, et al. (2021) Palliative Rehabilitation Improves Health Care Utilization and Function in Frail Older Adults with Chronic Lung Diseases. J Am Med Dir Assoc 22: 2478-2485.e1.
- Fukushima T, Tsuji T, Takashima K, Nakano J (2025) The current status of cancer rehabilitation provided by palliative care units in Japan: a nationwide survey. BMC Cancer 25: 451.
- Rosa WE, Lynch KA, Hadler RA, Mahoney C, Parker PA (2022) “Doing palliative care with my hands tied behind my back”: telepalliative care delivery for oncology inpatients during a COVID-19 surge. Transl Behav Med 12: 816-824.
- Harding Z, Hall C, Lloyd A (2022) Rehabilitation in palliative care: a qualitative study of team professionals. BMJ Support Palliat Care 12: e28-38.
- Brooks FA, Keeney T, Ritchie C, Tolchin DW (2021) Rehabilitation for Symptom Management for Patients with Cancer at the End of Life: Current Evidence and Barriers to Care. Curr Phys Med Rehabil Rep 9: 215-223.
- Brereton L, Clark J, Ingleton C, Gardiner C, Preston L, et al. (2017) What do we know about different models of providing palliative care? Findings from a systematic review of reviews. Palliat Med 31: 781-797.
- Juhrmann M, Butow P, Platts C, Boughey M, Simpson P, et al. (2024) Health professionals’ and caregivers’ perspectives on improving paramedics’ provision of palliative care in Australian communities: a qualitative study. BMJ Open 14: e086557.
- Ansari A, Baron A, Nelson-Becker H, Deamant C, Fitchett G, et al. (2022) Practice Improvement Projects in an Interdisciplinary Palliative Care Training Program. Am J Hosp Palliat Med 39: 831-837.
- Kostenko AM, Kupenko OV, Teslyk NM, Smiianova YO, Sahno KS (2022) Algorithm for Creating a Multidisciplinary Team in the Palliative Care System. Acta Balneologica 64: 178-182.
- Engel PT, Thavayogarajah T, Görlich D, Lenz P (2020) Establishment of a Palliative Care Consultation Service (PCCS) in an Acute Hospital Setting. Int J Environ Res Public Health 17: 4977.
- Gierach M, Brechtelsbauer D, Serfling J, Bloom K, Strickland G, et al. (2020) Students Practicing Interprofessional Collaboration in the Context of Hospice and Palliative Care. Am J Hosp Palliat Med 37: 1062-1067.
- Ferrell B, Buller H, Paice J, Anderson W, Donesky D (2019) End-ofLife Nursing and Education Consortium Communication Curriculum for Interdisciplinary Palliative Care Teams. J Palliat Med 22: 1082-1091.
- Ferrell BR, Buller H, Anderson W, Paice JA, Donesky D (2018) Interdisciplinary palliative care communication for quality palliative care: Outcomes of a statewide train-the-trainer course. J Clin Oncol 36: 83.
- Kolben T, Haberland B, Degenhardt T, Burgmann M, Koenig A, et al. (2018) Evaluation of an interdisciplinary palliative care inhouse training for professionals in gynecological oncology. Arch Gynecol Obstet 297: 767-773.
- Borneman T, Sun V, Williams AC, Fujinami R, Del Ferraro C, et al. (2015) Support for Patients and Family Caregivers in Lung Cancer: Educational Components of an Interdisciplinary Palliative Care Intervention. J Hosp Palliat Nurs 17: 309-318.
- Csikai EL, Bullock K (2024) The growth of social work in palliative and end-of-life care in the United States: how did we get here? Palliat Care Soc Pract 18: 26323524241263625.
- Ann-Yi S, Bruera E, Wu J, Liu DD, Agosta M, et al. (2018) Characteristics and Outcomes of Psychology Referrals in a Palliative Care Department. J Pain Symptom Manage 56: 344-351.
- Sun V, Kim JY, Irish TL, Borneman T, Sidhu RK, et al. (2016) Palliative care and spiritual well-being in lung cancer patients and family caregivers. Psychooncology 25: 1448-1455.
- Hoskin J (2021) Troubling norms? Adults and teenagers with a lifelimiting impairment in Denmark and England talk about their lives, support and future plans. Eur J Spec Needs Educ 36: 329-343.
- Yang S, McKernan D, Lynch M (2025) The ‘Art of Life’ project: stakeholder engagement report. Royal College of Surgeons in Ireland. p. 466499 Bytes.
- Padgett LS, Asher A, Cheville A (2018) The Intersection of Rehabilitation and Palliative Care: Patients with Advanced Cancer in the Inpatient Rehabilitation Setting. Rehabil Nurs 43: 219-228.
- Schmidt T, Gramkow MC, Poulsen DV, Miller LH, Wermuth L, et al. (2022) Study design of an interdisciplinary and participatory naturebased palliative rehabilitation intervention in a Danish nursing home for people with severe dementia. BMC Geriatr 22: 819.
- Palliative Care Commission (2025) Palliative Care and End-of-Life Care - Opportunities for England (Volume 1). England: Palliative Care Commission.
- Parola V, Coelho A, Neves H, Cardoso D, Almeida M, et al. (2020) Palliative rehabilitation interventions in palliative care: a scoping review protocol. JBI Evid Synth 18: 2349-2356.
- Modi J, Ghosh A, Pal R, Mohan R, Moscote-Salazar L, et al. (2021) Potential complications and sequelae of SARS-CoV-2 infection. Indian J Respir Care 10: 4-9.
- Harding Z, Hall C, Lloyd A (2022) Rehabilitation in palliative care: a qualitative study of team professionals. BMJ Support Palliat Care 12: E28-E38.
- Olesen LK, Cour KL, With H, Handberg C (2022) Reflections of family caregivers and health professionals on the everyday challenges of caring for persons with amyotrophic lateral sclerosis and cognitive impairments: a qualitative study. Palliat Care Soc Pract 16: 26323524221077702.
- Leung DYP, Chan HYL, Chiu PKC, Lo RSK, Lee LLY (2020) Source of Social Support and Caregiving Self-Efficacy on Caregiver Burden and Patient’s Quality of Life: A Path Analysis on Patients with Palliative Care Needs and Their Caregivers. Int J Environ Res Public Health 17: 5457.
- DeCoste-Lopez J, Madhok J, Harman S (2015) Curricular Innovations for Medical Students in Palliative and End-of-Life Care: A Systematic Review and Assessment of Study Quality. J Palliat Med 18: 338349.
- Robinson L, Matamoros C (2024) Applied patient-level palliative care interventions designed to meet the needs of sexual and gender minorities: A scoping review and qualitative content analysis of how to support sexual and gender minorities at end of life. Palliat Med 38: 69-84.
- Fettes L, Bone A, Etkind S, Ashford S, Higginson I, et al. (2021) Disability in Basic Activities of Daily Living Is Associated with Symptom Burden in Older People with Advanced Cancer or Chronic Obstructive Pulmonary Disease: A Secondary Data Analysis. J Pain Symptom Manage 61: 1205-1214.
- Buzgová R, Bar M, Bártová P, Kozáková R, Ressner P, et al. (2018) Neuropalliative and rehabilitative care in patients with an advanced stage of progressive neurological diseases. CESKA Slov Neurol Neurochir 81: 17-23.
- Gamskjaer T, Werlauff U, Handberg C (2022) Investigating job satisfaction in palliative rehabilitation: Reflections and perspectives of health professionals working with amyotrophic lateral sclerosis. J Eval Clin Pract 28: 108-119.
- Mittal A, Lowe E, Feldman C, Kogan A (2025) “I Don’t Want to Die on the Street”: Patient and Practitioner Perspectives on Street-Based Care for Older Adults Experiencing Unsheltered Homelessness. J Gen Intern Med 40: 3003-3012.
- Hinrichs KLM, Woolverton CB, Meyerson JL (2022) Help Me Understand: Providing Palliative Care to Individuals with Serious Mental Illness. Am J Hosp Palliat Med 39: 250-257.
- Fleisher JE, Klostermann EC, Hess SP, Lee J, Myrick E, et al. (2020) Interdisciplinary palliative care for people with advanced Parkinson’s disease: a view from the home. Ann Palliat Med 9: S80-S89.
- Lin RJ, Cohen AG, Stabler SM, Devlin SM, Elko TA, et al. (2020) Characteristics and Impact of Post-Transplant Interdisciplinary Palliative Care Consultation in Older Allogeneic Hematopoietic Cell Transplant Recipients. J Palliat Med 23: 1653-1657.
- Kumar TN (2016) Role of LTACH in Chronic Critical Illness in the Elderly. Zawada ET (Editor). 81 p. (Challenges in Elder Care).
- Hughes NM, Noyes J, Pritchard T, Stringer C (2025) Social Return on Investment Analysis: A Mixed Methods Approach to Assessing the Value of Adult Hospice Services. Value Health 28: 424-430.
- Carpenter JG (2022) Forced to Choose: When Medicare Policy Disrupts End-of-Life Care. J Aging Soc Policy 34: 661-668.
- Roessler M, Eulitz N (2018) Palliative medicine in emergency medical services. Anaesthesist 67: 366-374.
- Bayly J, Bradshaw A, Fettes L, Omarjee M, Talbot-Rice H, et al. (2022) Understanding the impact of the Covid-19 pandemic on delivery of rehabilitation in specialist palliative care services: An analysis of the CovPall-Rehab survey data. Palliat Med 36: 319-331.
- Chahal A, Chaudhuri P (2022). Smart health rehabilitation in palliative care during the COVID-19 era. Int J Palliat Nurs 28: 558-561.
- deLima Thomas J, Leiter RE, Abrahm JL, Shameklis JC, Kiser SB, et al. (2020) Development of a Palliative Care Toolkit for the COVID-19 Pandemic. J Pain Symptom Manage 60: e22-e25.
- Shih KK, Anderson AE, Brown J, Schuren N, Lyles MY, et al. (2022) Stay Home, Work Safe: Attitudes and Beliefs of Members of a Department of Palliative Care, Rehabilitation, and Integrative Medicine Regarding Remote Work during the COVID-19 Pandemic. J Palliat Med 25: 757-767.
- Winkler A, Kutschar P, Pitzer S, van der Zee-neuen A, Kerner S, et al. (2025) Avatar and virtual agent-assisted telecare for patients in their homes: A scoping review. J Telemed Telecare 31: 207-221.
- Gärtner H, Blix B, Raunkiær M, Timm H (2024) ‘There is nothing beautiful or life-affirming in it’: experiences of harm in a narrative course combining rehabilitative and palliative care approaches for people who have or have had cancer. Mortality 30: 695-711.
- Uleer C, Wight E, van Oorschot B, Panke J, Dauelsberg T, et al. (2022) Follow-up care, treatment of recurrences, psycho-oncological aspects, rehabilitation, physiotherapy and palliative care of endometrial cancer. GYNAKOLOGIE 55: 509-515.
- Vaughan VC, Martin P (2022) Multidisciplinary approaches to cancer cachexia: current service models and future perspectives. Expert Rev Anticancer Ther 22: 737-749.
- Graham-Wisener L, Crawford A (2025) Compassionate communities position paper: Fostering compassionate communities: A call to transform caregiving, dying, death and grieving on the island of Ireland [Position Paper]. All Ireland Institute for Hospice and Palliative Care & Queen’s University Belfast.
- Ross F (2018) Compassionate communities. Br J Community Nurs 23: 369.
- Steinhorn DM, Din J, Johnson A (2017) Healing, spirituality and integrative medicine. Ann Palliat Med 6: 237-247.
- Wang M, Ding X (2025) Integrated palliative care improves the quality of life of advanced cancer patients. BMC Palliat Care 24: 162.
- Keeney T, Wu C, Savini A, Stone S, Travis A, et al. (2024) Using Multiphase Optimization Strategy and Human-Centered Design to Create an Integrated Model of Palliative Care Skills in Home-Based Physical Therapy for Advanced Heart Failure. J Palliat Med 27: 526531.
- Koczywas M, Sun V, Hurria A, Cristea M, Raz DJ, et al. (2015) 1547 Interdisciplinary palliative care for lung cancer patients and family “Online Training Is Great but Human Interaction Is Better”: Training caregivers. Eur J Cancer 51: S220.
- 165. Caswell G, Pollock K, Harwood R, Porock D (2015) Communication between family carers and health professionals about end-of-life care for older people in the acute hospital setting: a qualitative study. BMC Palliat Care 14: 35.
- 166. Williams BR, Bailey FA, Goode PS, Kvale EA, Slay LA, et al. (2020) Preferences of VA Interdisciplinary Palliative Care Consult Teams. Am J Hosp Palliat Med 37: 800-808.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.