You’re Just Fat”: Diagnostic Overshadowing in Gynecology due to Obesity: A Case Report of 36 cm Ovarian Cyst Causing Torsion
by Anita Udabor1*, Chase Beverley Becker2, James Moir3, Jan Becker4
1University of Nicosia in Partnership with St George’s University of London, Medical School, Makedonitissis 46, 2417 Nicosia, Cyprus; Swedish Hospital. OB/GYN Dept., 5140 N California Ave, Chicago, IL 60625, USA.
2University of Nicosia in partnership with St George’s University of London, Medical School, Makedonitissis 46, 2417 Nicosia, Cyprus; Midwife Vision Global, Clinical Global Champion Training Dept, Yandina Creek, QLD 4561, Australia.
3Obstetrician, Gynaecologist, Retired Fertility Specialist Sunshine Coast, QLD, Australia Midwife Vision Global, Tanzania.
4Clinical Midwife Midwife Vision Global Champion Training Dept, Tanzania.
*Corresponding author: Anita Udabor, University of Nicosia in Partnership with St George’s University of London, Medical School, Makedonitissis 46, 2417 Nicosia, Cyprus; Swedish Hospital. OB/GYN Dept., 5140 N California Ave, Chicago, IL 60625, USA.
Received Date: 22 February 2024
Accepted Date: 27 February 2024
Published Date: 01 March, 2024
Citation: Udabor A, Becker CB, Moir J, Becker J (2024) You’re Just Fat”: Diagnostic Overshadowing in Gynecology due to Obesity: A Case Report of 36 cm Ovarian Cyst Causing Torsion. Gynecol Obstet Open Acc 8: 187. https://doi.org/10.29011/2577-2236.100187
Abstract
Background: Ovarian cysts are common in premenopausal women but can present with vague, and non-specific symptoms. Additionally, obesity can make discovery even more challenging. Diagnostic overshadowing due to obesity led to misdiagnosis of the presenting symptoms and signs. Most ovarian cysts are benign and resolve spontaneously; however, they can present, as in this case, as ovarian torsions, which is a gynecological emergency. Case presentation: A twenty-year-old female had presented over 3–4 times per year for the last 6 years to her primary doctor citing intermittent abdominal pain, irregular menstruation, dyspnea, and an enlarging abdomen circumference. The doctor stated, she was “just fat” and could, benefit from a “special camp to lose weight”, so she stopped mentioning her concerns. Upon presenting to the emergency department with acute onset abdominal pain, a computed tomography scan showed a large cyst lesion filling the abdominal and pelvic cavities. Its origin appeared to be from the left adnexa. Surgery was performed, and an acute ovarian torsion caused by a 36 cm craniocaudal left ovarian cyst was found and removed along with the left fallopian tube and 16 L of fluid. Conclusions. In this case, the patient presented recurring pelvic/abdominal concerns, and irregular menstruation, which warranted further investigation to safeguard fertility and prevent errors of omission. However diagnostic overshadowing due to obesity, hindered the care and standards procedures which could have resulted in early recognition and effective management.
Keywords: Ovarian Torsion; Large Cyst; Acute Abdomen; Case Report; Fertility; Third Presentation rule; Ovarian Serous Cystadenoma; Diagnostic Process in Primary Care, Case Report, Obesity, Medical Overshadowing
Introduction
An ovarian cyst is a common condition with a wide range of etiologies, particularly among premenopausal women [1]. The majority of these cysts are asymptomatic and resolve spontaneously; however, those measuring over 10 cm are considered large [2].
The presenting symptomatology of ovarian cysts can be subtle, for example, gradual undefined pelvic pain, early satiety, bloating, enlarging abdomen, and irregular menstrual history. Addressing these concerns is an important step for primary physicians to maintain trusting relationships in patients’ care [1, 3]. Large ovarian cysts with the most common types being benign ovarian serous cystadenomas, are rare, due to more effective multiscreening methods [4, 5]. However, they can lead to torsion and present as abdominal pain in over 58% of cases [4, 6].
This report will discuss a case of a large cystic structure ovarian cyst that developed over 6 years, which led to acute emergency surgery for ovarian torsion. Additionally, this case will explore the history and management of this patient—including from the patient’s first-hand perspective. Further, we explore the clinical significance of diagnostic overshadowing which is highlighted in this case study [1]. Diagnostic overshadowing links clinical bias which can be harmful to the patient because of delays and or disparity in diagnosis and care [2, 3].
The importance of considering the differential diagnoses of acute abdomen in women of reproductive age, obtaining accurate imaging, and considering the appropriate surgical techniques may prevent adverse consequences, such as the loss of fertility, complications from rupture and hemorrhage, or from exploratory laparotomy, or even death [8-10].
Case Presentation
The patient, a 20-year-old Hispanic nulliparous female, presented to the emergency department one hour after the onset of a severe “stabbing” pain in the lower left quadrant and non-radiating pain in her abdomen after feeling the urge to defecate. Further, she had several episodes of non-bloody, non-bilious emesis. She was afebrile on admission, with no chest pain, no acute shortness of breath, or any urinary frequency or pain. From a gynaecological perspective, the patient was a virgin, with first menarche at 11 years old, a history of oligomenorrhea (2 months apart), and her last menstrual period was 29 days before presentation. There was no vaginal discharge or bleeding on admission. The patient had a current history of breathlessness which had been attributed to mild asthma managed with a prescribed inhaler, used occasionally.
There was a surgical history of an appendectomy in 2006 with an unremarkable recovery. The patient had no allergies, was a nonsmoker, no illicit substance use, and drank alcohol socially. There was no relevant family history for ovarian malignancies or BRCA1 and 2 mutations. The patient worked in the childcare profession whilst attending her second year of university studies.
On examination, the patient appeared to be obese, welldeveloped, anxious, and cooperative. She was not able to tolerate a speculum examination due to the pain. There was no pulsatile abdominal mass, guarding of the abdomen, nor any generalized and/or rebound tenderness or rigidity. The lower left quadrant of the patient’s abdomen was tender with mild distention and normal bowel sounds were heard. An elevated blood pressure on admission (145/89) was noted. The urinalysis was unremarkable. Blood analysis showed hypochromic, microcytic anemia (10.3 g/ dL) with +1 anisocytosis (generally associated with iron deficiency anemia [11], and mild elevated chloride (109 mEq/L) and elevated glucose (109 mg/dL) levels. A pelvic ultrasound reported a normal uterus with no endometrial abnormalities, and the right ovary appeared normal. The left ovary was not visualized (Figures 1 and Figure 2). A large cystic structure was seen, whose origin was unknown. An abdominal/pelvic computerized tomography (CT) with contrast found a 36 cm cyst lesion filling the abdominal and pelvic cavity which appeared to originate from the left adnexa with a complicated hyperdense fluid or debris focus noted in the inferior margin of the cyst (Figure 3). The surrounding structures appeared unremarkable. There was a trace amount of fluid in the Pouch of Douglas. (Figure 4).
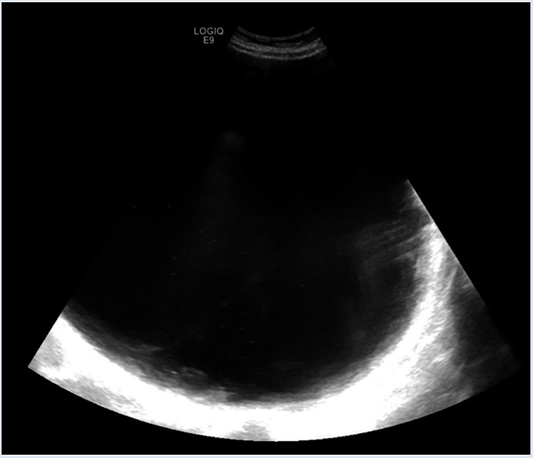
Figure 1: Image of the cyst on transabdominal ultrasound. Due to the size of the cyst, it could not be visualized entirely within the same image.
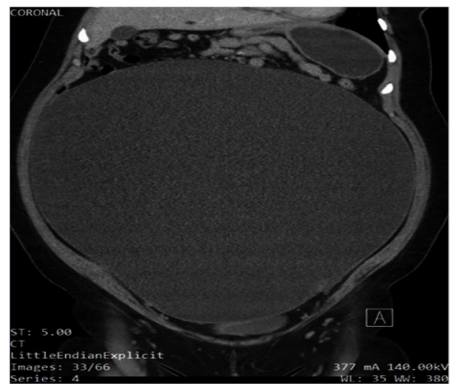
Figure 2: Ultrasound image showing the cyst’s complex blood supply. This complexity raised suspicion for malignancy
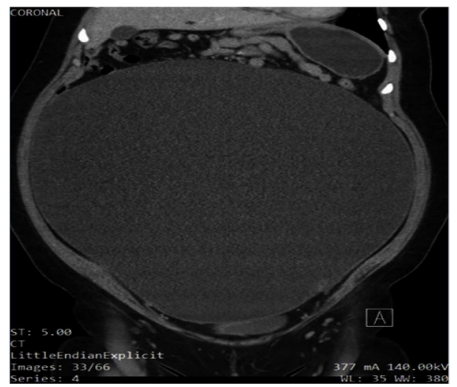
Figure 3: Sagittal slice of the patient’s abdomen on non-contrast CT showing the cyst occupying most of the abdominal cavity.
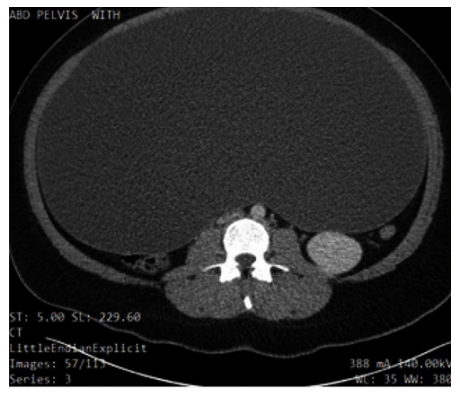
Figure 4: Coronal slice of non-contrast CT of abdomen demonstrating the compression of the neighboring structures up to the thoracic cavity, which explains some of the patient’s symptoms, such as shortness of breath.
The cyst was isolated in a bag, allowing half of its volume (eight liters) to be drained. A left salpingo-oophorectomy was performed, and the cyst was removed (along with a further 8 L of fluid) without rupture, with minimal blood loss (100 milliliters). The pathology report described the presence of a benign hemorrhagic serous cystadenoma (with a hemorrhagic left fallopian tube) from interoperative frozen section.
The patient tolerated surgery without complications and her postoperative recovery went well. During her stay, her anaemia (haemoglobin was >100 g/dL) was not treated. In the months following surgery, the patient’s menstruation became “more regular” with approximately five days of heavy bleeding. The patient’s breathlessness resolved immediately after surgery, obviating the need for an inhaler. She lost further weight following the surgery and felt she has seen psychological improvements.
Approximately 12 months following the surgery, due to concerns of dizziness (suspected to be related to anaemia), she was started on oral contraceptives to reduce her heavy menstrual bleeding. However, no iron supplements were prescribed. The patient subsequently discontinued the oral contraceptive due to her apprehensions of side effects, such as weight gain.
During her recovery, the patient wanted to share her history leading up to the emergency surgery. From when she was 12 to 13 years old, she presented to her primary care doctor at least three times per year due to pain when lifting heavy objects, and intermittent rigidity of her abdomen (specifically umbilical). Further, she was concerned that her abdomen was enlarging, and she noted menstrual irregularities and dyspnoeal. She was advised by her doctor that her symptoms were due to obesity (told “you’re just fat”). At no time during the nine years since the commencement of menses and bringing these concerns to her doctor, were any investigations, scans, or blood tests undertaken. Nor was she referred to a gynaecologist where her age, duration of her symptomology (6–7 years), and otherwise general health may have identified a complicated benign ovarian cyst that had failed to involute, which turned out to be the case. Her Body Mass Index (BMI) was not documented. No genetic testing was undertaken. The patient eventually stopped presenting her concerns to her doctor over fears that the medical professionals were going to send her to a “special camp to lose weight”.
Discussion
Ovarian cysts are most commonly occur in women of reproductive age and are usually benign [8]. In these women, endogenous hormone production may stimulate the growth of such cysts during pregnancy [9]. In postmenopausal women and in women whose cysts are not simple (e.g., solid), a malignancy is more likely [12]. Whether the process of cyst formation occurs due to the failure of the dominant follicle to rupture or whether the immature follicles fail to involute is not known; however, the conclusion is the same [13]. These cases usually result in the formation of functional cysts, such as corpus luteum cysts, thecalutein cysts, or follicular cysts [9]. Moreover, genetic mutations such as Lynch II syndrome or BRCA-1 and 2 mutations may play a role in the development of more malignant cysts [8,14].
Due to the nature of ovarian cysts being mostly asymptomatic or spontaneously involuting, epidemiological data are difficult to ascertain [1]. The occurrence of ovarian cysts is estimated to be 35% in premenopausal women and 17% in postmenopausal women [15].
The small percentage of premenopausal women who experience rare, grossly enlarged cysts may have associated risk factors such as a history of early menarche, endometriosis, polycystic ovary syndrome (PCOS), pregnancy, or treatment for infertility. However, the patient in this case study had no associated risks [6,16].
She experienced compression and distortion of abdominal– pelvic structures, which presented as bloating, pain, and difficulty breathing.. She bought all these concerns to her physician’s attention over many years, but due to many potential factors (such as the doctor’s time constraints or factors like the financial incentive programs for physicians in US for faster patient throughput), along with seemingly vague symptoms, patient care was hindered [4,18,19].
Nonetheless, re-presentations in over three visits should have raised a red flag and at the very least, some investigations should have been carried out [1,20].
To enable physicians in primary care to diagnose and manage patients’ symptoms, a “point of care” database could be used which can be directly impact patient care [18].
Primary health care plays a vital role in the health and wellbeing of the population, so any tools that assist in the management of this care can be of benefit [21]. Yet, many doctors’ express concerns that they have inadequate time to address all of the patients’ concerns [22].
A therapeutic alliance between the primary physician and patient is a cornerstone of clinical care [23]. Research has found that doctors miss many cues [23] which can be addressed with training in communication to strengthen patient–doctor relationships and therapeutic trust [24, 25].
In all situations, a thorough clinical history and physical examination are required, with a specific emphasis on gynaecological and gastrointestinal etiologies (e.g. menstruation, pregnancy, bowel movements, etc.). However, the initial stabilization takes precedence over a more in-depth history of a patient in need of emergency care.
In this patient’s case, her primary care doctor may not have addressed her symptomatology, as they were non-specific, mild, and without any red flags. However, her oligo menorrhoea, significant weight gain, umbilical pain when lifting objects, and the patient’s growing concerns and repeated presentation should have warranted more investigation.. Certainly, the patient did not feel heard or even acknowledged, eventually “giving up” trying to address her concerns with her primary care doctor. Two factors interconnect in primary care: the patient’s concerns being articulated clearly and the physician’s response to enable better care outcomes; in this case, the patient lost faith and trust in the physician [23, 26]. Further, she felt judged for her obesity and repeatedly unheard in her concerns which she articulated during her hospital recovery.
The patient specifically wished to convey to the researchers that present and future clinicians should “double-check” the patient’s test results, as well as listen to their concerns regarding their presenting complaints which has been highlighted by other patients in other clinical settings [7,27].
The lack of a trusting relationship due to poor communication on the physician’s side has been shown to be detrimental in future patient–doctor relationships and therefore the patient’s future health [28,29].
Cysts that are >5 cm or have a complex pathology are unlikely to involute and therefore require surgical removal (if surgery is not contraindicated) [16,30]. Emergency presentations, such as rupture, haemorrhage, or torsion, are indications for emergency surgical intervention. Laparoscopic surgery utilizes smaller incisions and is more desirable for stable, simple cysts, as they have a reduced risk profile and recovery time [6]. However, exploratory laparotomy, such as in this patient, may be required because of the complexity and size of the cyst, the presentation of the patient, and the fluid volume within the cyst [31,32].
When a cyst is likely benign (e.g., in a premenopausal woman who has plans to have children in the future), fertility-preserving surgery should be performed [10]. Although the patient expressed her worries about conceiving in the future, she was comforted by knowing that her remaining ovary was still functional and unaffected by the surgery.
The clinical presentation and radiological or gross findings of the mass can be provisionally diagnostic for an ovarian cyst. The type of cyst (can be confirmed by histopathology). This patient had a common serous cystadenoma with some hemorrhagic debris, which likely caused a complex appearance in the radiological images. Her prognosis is reassuring considering that there has been no proven link between cystadenomas and conversion to ovarian cancer, with an overall survival of approximately 85% at 5 years [8].
The cyst was twisted around the left fallopian tube, which was likely facilitated by its size, and it would have been present for an extended period of time before acute manifestations occurred. The larger a cyst is, the higher the risk of torsion [30]. The likelihood of torsion of an ovarian cyst was the primary reason for emergency surgery and the acute presentation in this case. The management of an enlarged ovarian cyst depends on the pathology of the cyst, its complexity (the radiological features including size, the histopathology, etc.), its effect on the adjacent structures, and the life-stage of the woman (pre- vs. postmenopausal) (Table 1) [34]. In a premenopausal woman, if a cyst is not complex and does not adversely affect the patient (e.g., does not compress the adjacent pelvic structures), then the cyst can be monitored, as it is likely to resolve spontaneously [34]. However, explorative laparoscopy or laparotomy is indicated if the cyst enlarges (or is >5 cm in size), becomes more complex, or begins to adversely affect the patient [10]. In the case of this patient who presented with acute abdominal pain, the immediate management was laparotomy due to the possibility of a hemorrhagic cyst, the rupture of the cyst, or an ovarian torsion. as well as its uncharacteristically large size [32].
Table 1: Management of acute adnexal masses in stable, unwell women (adaptation of ACOG and RCOG guidelines) [8, 15].
When a malignancy is suspected in postmenopausal women or in older women with bilateral cysts, more radical management is undertaken, such as a frozen section biopsy during surgery, a bilateral oophorectomy, and a blood analysis for tumor markers (including serum CA- 125) [34]. When cases appear more complex, such as in this patient, the radiological findings can be used to give a preoperative risk stratification score. The Ovarian– Adnexal Reporting and Data System (O-RADS) is a valuable risk stratification and management tool for USA-based patients [35]. The Risk Malignancy Index (RMI), which is based on the ultrasound scanning parameters set out by the International Ovarian Tumor Analysis (IOTA) Group, is the primary radiological stratification tool that is used in the UK [8,10]. The prognosis for ovarian cysts is reassuring in the long term; however, there is an increased risk of ovarian cancer in premenopausal women if endometriosis is present (which was not the case for this patient).
Conclusions
Ovarian cysts are a common gynecological manifestation in premenopausal women. If the cysts are less than 10 cm in diameter, they tend to involute spontaneously without symptoms, however surgery can be considered if over 5cm. However, in rare cases of enlarged cysts, patients can present with symptoms that are consistent with the gradual compression of abdominal and/or pelvic structures or, as in the case of this patient, an emergency case of ovarian torsion. With an ovarian cyst of this size, there is a possibility of rupture, with potentially serious complications.
This case also highlights the importance of the harm that can stem from cognitive bias. Further, diagnostic overshadowing in the primary care, setting impacts many patients who are autistic, have low health literacy, mental health issues, obesity and dementia. By attributing physical clinical signs and symptoms to a preexisting condition like obesity the primary care physicians can mistakenly pre-judge the diagnosis.
In this patient, earlier diagnosis could have avoided the emergency admission for surgery and may have not adversely affected the patient’s future fertility plans.
Limitations
It may be difficult to generalize the details of this case report to a broader population because the case is unusual.
The patient was interviewed and gave her account, but the primary care physician was not interviewed so there is a potential for patient-centric bias.To reduce the limitations and improve the quality of this report, it was written adhering to the ConsensusBased Clinical Case Reporting (CARE) Guidelines.
Author Contributions: A.U. and C.B.B. agreed on the study conception, study design, and data analysis. Data collection was completed by A.U. Initial drafts were completed by A.U. and C.B.B. Reviews and further editing were performed by A.U., C.B.B., JB and J.M. AJE and MDPI services were used for final editing, formatting and figure formatting before submission for publishing. A.U., C.B.B., JB, and J.M. approved the final version and consented to publish. All authors have read and agreed to the published version of the manuscript.
References
- Oliver A, Overton C (2014) Detecting ovarian disorders in primary care. Practitioner 258: 15-19.
- Pramana C, Almarjan L, Mahaputera P, Wicaksono S A, Respati G, et al. (2022) A Giant Ovarian Cystadenoma in A 20-Year-Old Nulliparous Woman: A Case Report. Front Surg 9: 895025-385.
- Kappen T, van Dulmen S (2008) General practitioners‘ responses to the initial presentation of medically unexplained symptoms: a quantitative analysis. BioPsychoSocial Medicine 2, 22.
- PV Attinàx, Spadola G, Caltabiano S, Farina R, Palmucci S, et al. (2016) MR imaging of ovarian masses: classification and differential diagnosis. Insights Imaging 7: 21-41.
- Diop B, Niang MM, Ba PA, Toure PS, Sy A, et al. (2016) Management of Giant Ovarian Cysts: A Review of 5 Case Reports. Journal of Gynecologic Surgery 32: 162-166.
- Peters S, Rogers A, Salmon P, Gask L, Dowrick C, et al. (2009) What do patients choose to tell their doctors? Qualitative analysis of potential barriers to reattributing medically unexplained symptoms. J Gen Intern Med 24: 443-449.
- Royal College of Obstetricians and Gynaecologists. Management of Suspected Ovarian Masses in Premenopausal Women (2011) 14.
- Mobeen S, AR (2023) Ovarian Cyst; StatPearls Publishing: Treasure Island, FL.
- Terzic M, Aimagambetova G, Norton M, Della Corte L, Marín-Buck A, et al. (2021) Scoring systems for the evaluation of adnexal masses nature: current knowledge and clinical applications. J Obstet Gynaecol 41: 340-347.
- Chai AL, Huang OY, Rakočević R, Chung P (2021) Critical iron deficiency anemia with record low hemoglobin: a case report. J Med Case Rep 15: 472.
- Mustafin C, Vesnin S, Turnbull A, Dixon M, Goltsov A, et al. (2022) Diagnostics of Ovarian Tumors in Postmenopausal Patients. Diagnostics (Basel) 2022, 12: 2619.
- Hall G H, Turnbull L W, Richmond I, Helboe L, Atkin S L (2002) Localisation of somatostatin and somatostatin receptors in benign and malignant ovarian tumours. Br J Cancer 87: 86-90.
- Fostira F, Papadimitriou M, Papadimitriou C (2020) Current practices on genetic testing in ovarian cancer. Ann Transl Med 8: 1703.
- Gynecologists. A.C.o.O.a. Practice Bulletin No. 174: Evaluation and Management of Adnexal Masses (2016) 128: e210-e226.
- Ross E K, Kebria M (2013) Incidental ovarian cysts: When to reassure, when to reassess, when to refer. Cleve Clin J Med 80: 503-514.
- Sutton RT, Pincock D, Baumgart DC, Sadowski DC, Fedorak RN, et al. (2020) An overview of clinical decision support systems: benefits, risks, and strategies for success. npj Digital Medicine 6: 3
- Abu Sulb A, Abu El Haija M, Muthukumar A (2016) Incidental finding of a huge ovarian serous cystadenoma in an adolescent female with menorrhagia. SAGE Open Medical Case Reports 4: 2050313X16645755.
- Protus B M (2014) BMJ Best Practice. J Med Libr Association 102: 224-225.
- Chawla D, Thukral A, Kumar P, Deorari A (2021) Harnessing mobile technology to deliver evidence-based maternal-infant care. Seminars in Fetal and Neonatal Medicine.
- Eide H, Quera V, Graugaard P, Finset A (2004) Physician–patient dialogue surrounding patients’ expression of concern: applying sequence analysis to RIAS. Social Science & Medicine 59: 145-155.
- Levinson W, Gorawara-Bhat R, Lamb J (2000) A Study of Patient Clues and Physician Responses in Primary Care and Surgical Settings. Jama 284: 1021-1027
- Roter DL, Hall JA, Kern DE, Barker LR, Cole KA, et al. (1995) Improving physicians‘ interviewing skills and reducing patients‘ emotional distress: a randomized clinical trial. Archives of internal medicine 155: 1877-1884.
- Axelrod DA, Goold SD (2000) Maintaining Trust in the Surgeon-Patient Relationship: Challenges for the New Millennium. Archives of Surgery 135: 55-61.
- Detmar S, Aaronson N, Wever L, Muller M, Schornagel J (2000) How are you feeling? Who wants to know? Patients’ and oncologists’ preferences for discussing health-related quality-of-life issues. Journal of clinical oncology 18: 3295-3301.
- Love T, Fahey T (2003) Defining diagnosis: screening and decision making in primary care. Br J Gen Pract 53: 914-915.
- Hall J A, Irish J T, Roter D L, Ehrlich C M, Miller L H (1994) Satisfaction, gender, and communication in medical visits. Medical care 32: 12161231.
- Graugaard PK, Holgersen K, Eide H, Finset A (2005) Changes in physician–patient communication from initial to return visits: a prospective study in a haematology outpatient clinic. Patient education and counseling 57: 22-29.
- Huang C, Hong MK, Ding DC (2017) A review of ovary torsion. Ci Ji Yi Xue Za Zhi 29: 143-147.
- Leite C, Barbosa B, Santos N, Oliveira A, Casimiro C (2020) Giant abdominal cyst in a young female patient: A case report. Int J Surg Case Rep 72: 549-555.
- Lo L M, Chang SD, Horng SG, Yang T Y, Lee CL, et al. (2008) Laparoscopy versus laparotomy for surgical intervention of ovarian torsion. J Obstet Gynaecol Res 34: 1020-1025.
- Ravishankar TN, Makarand Jadhav H, Satheesh Kumar N, Ambala S, Pillai NM (2023) A deep learning approach for ovarian cysts detection and classification (OCD-FCNN) using fuzzy convolutional neural network. Measurement: Sensors 27: 100797.
- Biggs WS, Marks ST (2016) Diagnosis and Management of Adnexal Masses. Am Fam Physician 93: 676-681.
- Andreotti RF, Timmerman D, Strachowski LM, Froyman W, Benacerraf BR, et al. (2020) O-RADS US Risk Stratification and Management System: A Consensus Guideline from the ACR Ovarian-Adnexal Reporting and Data System Committee. Radiology 294: 168-185.
- Zhang J-J, Cao D-Y, Yang J-X, Shen K (2020) Ovarian metastasis from nongynecologic primary sites: aretrospective analysis of 177 cases and 13-year experience. Journal of Ovarian Research 13: 128.
- Elusive and Rare. Clinician Beware, Giant Ovarian Cysts are Elusive and Rare Cureus (2020) 12: e6753.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.