Vitamin D Levels in African American Adults Attending Family Practice Clinic at Howard University Hospital
by Lalita Kaul1, Nadia Yusuf1, Neeraj Kak1*, Hilal Alsaffar2, Samer Alhakak2, Fatima Abakaa2, Hala AlMossawi1,2
1Howard University, USA
2University of AlKafeel, Najaf, Iraq
*Corresponding author: Neeraj Kak, Howard University, USA
Received Date: 15 February, 2025
Accepted Date: 25 February, 2025
Published Date: 28 February, 2025
Citation: Kaul L, Yusuf N, Kak N, Alsaffar H, Alhakak S, et al. (2025) Vitamin D Levels in African American Adults Attending Family Practice Clinic at Howard University Hospital. J Community Med Public Health 9: 506. https://doi.org/10.29011/2577-2228.100506
Introduction
Vitamin D, a fat-soluble vitamin produced in the skin upon exposure to sunlight, plays a crucial role in maintaining bone health and has been increasingly recognized for its importance in cardiovascular health. Recent statistics indicate that Vitamin D deficiency is a global health issue, with a pooled analysis from 2000 to 2022 revealing that 47.9% of participants had serum 25-hydroxyvitamin D levels less than 50 nmol/L. In the United States, the prevalence of Vitamin D deficiency is similarly high, affecting between 30% and 50% of the general population. This deficiency is due to inadequate cutaneous production resulting from decreased exposure to sunlight (Figures 1 and 2).

Figure 1: Vitamin D metabolism. Source: https://www.precisionnutrition.com/all-about-vitamin-D
Historically, Vitamin D deficiency has been linked to rickets in the pediatric population and osteomalacia/osteoporosis in adults. Recent studies have demonstrated the presence of Vitamin D receptors on a variety of cells, including vascular endothelial cells and pancreatic beta cells, suggesting a broader role for Vitamin D in cardiovascular and insulin-related health. A significant amount of evidence currently suggests a connection between suboptimal levels of Vitamin D and negative cardiovascular outcomes such as hypertension, hyperlipidaemia, myocardial infarction, and stroke.
Vitamin D deficiency is much more prevalent among young African Americans, who often do not achieve optimal Vitamin D concentrations at any time of the year. This is mostly due to pigmentation reducing Vitamin D production in the skin, but also from lower dietary intake of Vitamin D-rich foods. From puberty onward, the median Vitamin D intake of American Black people is below the recommended intake in every age group. This increases the risk of diseases against which Vitamin D has a protective effect, including cardiovascular disease, diabetes, lupus, and some cancers (e.g., breast cancer).

{kind=link}
Recent studies have highlighted the broader implications of Vitamin D deficiency. For example, Vitamin D receptors have been found on various cells, including vascular endothelial cells and pancreatic beta cells, leading to further study of cardiovascular and insulin-related risks associated with Vitamin D deficiency. Additionally, there is a push for clinicians to take more initiative-taking in educating patients on the benefits of Vitamin D supplementation, especially in populations at higher risk of deficiency.
The significance of this study lies in its focus on an African American population, which is disproportionately affected by Vitamin D deficiency and its associated health risks. By investigating the association between suboptimal Vitamin D levels and lipid profiles in patients on and off statin drugs, this study aims to provide insights into the potential benefits of Vitamin D supplementation in improving cardiovascular health outcomes.

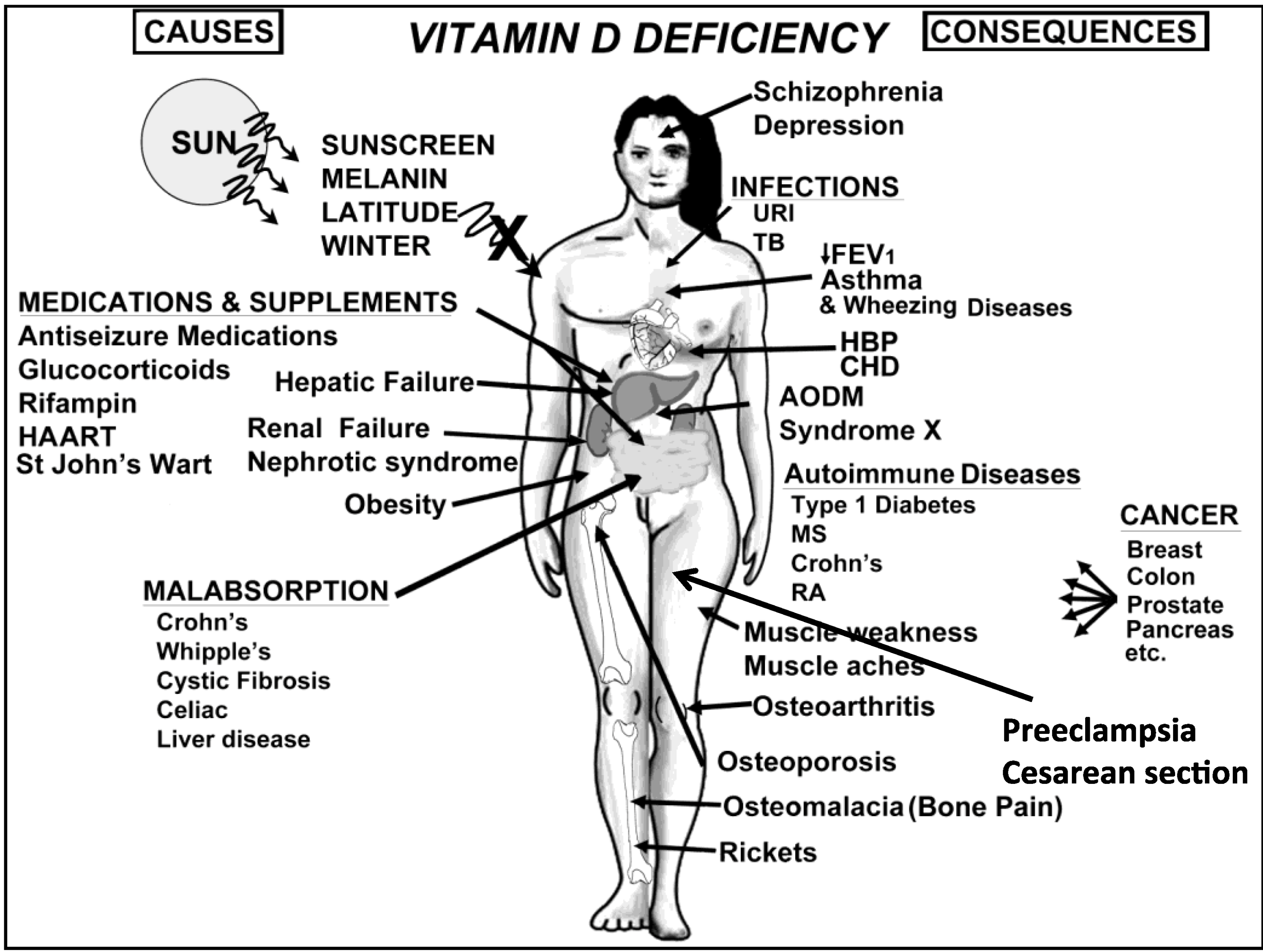
Figure 3: Vitamin D deficiency: causes and consequences. Source: https://www.mdpi.com/nutrients/nutrients-05-00111/article_deploy/ html/images/nutrients-05-00111-g006.png
{kind=link}
Vitamin D deficiency has been linked to various adverse health outcomes, including hypertension, hyperlipidaemia, myocardial infarction, and stroke. Recent studies have demonstrated the presence of Vitamin D receptors on a variety of cells, including vascular endothelial cells and pancreatic beta cells, suggesting a broader role for Vitamin D in cardiovascular and insulin-related health (Figure 3). Furthermore, Vitamin D deficiency is particularly prevalent among young African Americans, who often do not achieve optimal Vitamin D concentrations due to pigmentation reducing Vitamin D production in the skin and lower dietary intake of Vitamin D-rich foods. This increases their risk of cardiovascular diseases, diabetes, lupus, and certain cancers.
Objectives
The objectives of this study are:
- To investigate the association between suboptimal Vitamin D levels and lipid profiles in patients on and off statin drugs within an African American population attending a family medicine clinic in an urban location.
- To determine whether low Vitamin D levels correlate with poor lipid profiles even in patients on statin medication, thereby assessing the appropriateness and usefulness of Vitamin D supplementation in these patients.
This study aims to fill a gap in the existing literature by focusing on an African American population and comparing its findings with recent studies. For instance, a 2024 study assessed the relative importance of Vitamin D deficiency in cardiovascular health and found that traditional risk factors like blood pressure and BMI were more significant.
Methods
Study Design: This is an observational, cross-sectional study conducted at a Family Practice Clinic affiliated with Howard University Hospital in an urban location.
|
Section |
Details |
|
Participants |
Patients aged 35 to 76 attended the clinic between June and September 2013. Patients with known conditions affect Vitamin D metabolism (e.g., sarcoidosis, hyperparathyroidism). |
|
Data Collection |
Data collected includes serum 25-hydroxyvitamin D levels, total cholesterol, triglycerides, HDL, LDL, blood pressure, BMI, and history of cardiovascular events. Data was obtained from patient medical records. Serum 25-hydroxyvitamin D levels were measured using a chemiluminescent immunoassay. Lipid profiles were obtained through standard laboratory tests. |
|
Statistical Analysis |
Descriptive statistics used to summarize the data. T-tests will compare means between groups (patients on and off statins), and chi-square tests will analyze categorical variables. P-values < 0.05 considered statistically significant. Statistical analyses performed using SPSS version 25. Missing data will be addressed using multiple imputation methods. |
|
Ethical Considerations |
The study protocol was approved by the Institutional Review Board (IRB) of Howard University. Informed consent was obtained from all participants prior to data collection. |
Results
The results presented in Tables 1 and 2 below compare patients on and off statin. A comprehensive statistical analysis, incorporating p-values and confidence intervals, was conducted to substantiate the findings. Preliminary observations indicate no significant difference in LDL levels between the two groups, with both having an average LDL of 99. However, triglyceride (TG) levels were higher in the off-statin group, and HDL levels were higher in the off-statin group as well. Systolic blood pressure and BMI were slightly better in the off-statin group. Table 1 lists patients on statin therapy. Key results include:
- Age: The average age of patients on statins is 61.1 years, with a range spanning from 50 to 76 years. This indicates that older adults are more likely to be prescribed statins.
- Gender: 3 males and 6 females on statins, showing a higher prevalence in females.
- Vitamin D: The average Vitamin D level is 19.81 ng/ mL, with some patients having significantly low levels (as low as 11.7 ng/mL). This suggests a need for monitoring and possibly supplementing Vitamin D in these patients.
- Total Cholesterol: The average total cholesterol level is 170.44 mg/dL. Notably, some patients have high cholesterol levels, such as a patient with 216 mg/dL.
- Triglycerides (TG): The average triglyceride level is 102.89 mg/dL. While some patients have elevated levels, a few have significantly low levels.
- HDL (Good Cholesterol): The average HDL level is 52 mg/dL, with a minimum of 37 mg/dL and a maximum of 66 mg/ dL.
- LDL (Bad Cholesterol): The average LDL level is 99 mg/ dL. A few patients have elevated LDL levels, indicating a need for tighter control.
- Blood Pressure (BP): The average diastolic BP is 65 mmHg, and the average systolic BP is 124.9 mmHg. This shows generally controlled blood pressure among the patients.
- BMI: The average BMI is 31.86, which falls into the overweight category. This suggests that weight management could be an important aspect of these patients’ health plans.
Table 2 lists patients not on Statin therapy. Key results include:
- Age: The average age of patients not on statins is 51.1 years, with a range from 35 to 64 years. This indicates a younger population compared to those on statins.
- Gender: The gender distribution is equal, with 6 males and 6 females.
- Vitamin D: The average Vitamin D level is 19.25 ng/mL. There is a notable variation, with some patients having levels as low as 9.6 ng/mL.
- Total Cholesterol: The average total cholesterol level is 184.45 mg/dL. Some patients have very high levels, such as a patient with 295 mg/dL.
- Triglycerides (TG): The average triglyceride level is 128.82 mg/dL. Several patients have elevated levels, indicating potential risk factors for cardiovascular issues.
- HDL (Good Cholesterol): The average HDL level is 61 mg/dL, which is higher than the HDL levels of patients on statins.
- LDL (Bad Cholesterol): The average LDL level is 99 mg/dL. Similar to patients on statins, this indicates a need for monitoring.
- Blood Pressure (BP): The average diastolic BP is 74 mmHg, and the average systolic BP is 120.4 mmHg. These values indicate well-controlled blood pressure overall.
- BMI: The average BMI is 36.83, which indicates obesity in the patient population. This underscores the importance of weight management and lifestyle interventions.
|
Patient Initials |
Age |
Gender |
Vit D |
Total Cholesterol |
TG |
HDL |
LDL |
BPd |
BPs |
BMI |
History of Events |
|
EN |
56 |
M |
16.8 |
201 |
75 |
37 |
149 |
70 |
140 |
27.99 |
No |
|
IDE |
69 |
F |
16 |
190 |
61 |
66 |
112 |
62 |
102 |
33.12 |
Palpitations |
|
RB |
57 |
F |
17.4 |
140 |
92 |
48 |
74 |
80 |
140 |
46.07 |
No |
|
RH |
56 |
M |
UNK |
130 |
22 |
51 |
77 |
63 |
101 |
UNK |
No |
|
JO |
76 |
F |
26.5 |
198 |
108 |
52 |
124 |
74 |
142 |
36.54 |
No |
|
RJ |
58 |
M |
16.9 |
178 |
76 |
66 |
103 |
60 |
110 |
20.94 |
No |
|
JD |
59 |
F |
11.7 |
140 |
129 |
47 |
67 |
70 |
110 |
37.89 |
TIA |
|
DH |
50 |
F |
23.2 |
141 |
135 |
57 |
57 |
87 |
161 |
38.82 |
No |
|
BAF |
69 |
F |
30 |
216 |
228 |
45 |
125 |
78 |
118 |
42.40 |
No |
|
Averages |
61.1 |
3M,6F |
19.81 |
170.444444 |
102.889 |
52 |
99 |
65 |
124.9 |
31.86 |
Table 1: Patients on Statin therapy.
|
Patient Initials |
Age |
Gender |
Vit D |
Total Cholesterol |
TG |
HDL |
LDL |
BPd |
BPs |
BMI |
History of Events |
|
GF |
52 |
F |
21 |
196 |
53 |
93 |
92 |
80 |
120 |
49.5 |
PE/CP |
|
PQH |
48 |
F |
18.9 |
199 |
71 |
46 |
139 |
78 |
123 |
30.48 |
No |
|
BJ |
58 |
M |
29.7 |
UNK |
UNK |
43 |
69 |
68 |
122 |
25.60 |
No |
|
ME |
48 |
F |
15.1 |
140 |
132 |
42 |
72 |
50 |
110 |
29.26 |
No |
|
JH |
64 |
F |
22.7 |
295 |
224 |
110 |
140 |
70 |
120 |
25.58 |
No |
|
AD |
52 |
M |
15.2 |
114 |
69 |
39 |
61 |
74 |
120 |
30.81 |
h/o pericarditis |
|
JK |
35 |
M |
23.6 |
182 |
62 |
67 |
103 |
62 |
114 |
24.00 |
No |
|
TB |
60 |
M |
13.6 |
173 |
227 |
41 |
87 |
64 |
112 |
37.57 |
No |
|
AH |
52 |
M |
9.6 |
144 |
151 |
56 |
58 |
94 |
146 |
31.52 |
No |
|
SK |
45 |
M |
16 |
219 |
176 |
68 |
116 |
80 |
120 |
28.4 |
No |
|
JG |
51 |
F |
28.4 |
139 |
64 |
56 |
70 |
72 |
114 |
33.32 |
No |
|
CB |
48 |
F |
17.2 |
228 |
188 |
69 |
181 |
90 |
124 |
23.92 |
No |
|
Averages |
51.1 |
6M, 6F |
19.25 |
184.454555 |
128.818 |
61 |
99 |
74 |
120.4 |
36.83 |
Table 2: Patients not on Statin therapy.
Discussion
The study examines the detailed data of patients on statin therapy and those not on statin therapy. The analysis includes various metrics such as age, gender, Vitamin D levels, cholesterol levels, blood pressure, BMI, and history of events.
- Age: The average age of patients on statins is 61.1 years, with a range from 50 to 76 years. This indicates that older adults are more likely to be prescribed statins, which aligns with the increased risk of cardiovascular diseases in this age group. In contrast, the average age of patients not on statins is 51.1 years, ranging from 35 to 64 years. This younger demographic may suggest that they have not yet reached the threshold for statin therapy or their cardiovascular risk factors are managed through other means.
- Gender: Among the patients on statins, there are 3 males and 6 females, showing a higher prevalence of statin use among females. This might be due to higher cholesterol levels or other risk factors in females within this patient group. On the other hand, the gender distribution in the non-statin group is equal, with 6 males and 6 females.
- Vitamin D Levels: The average Vitamin D level for patients on statins is 19.81 ng/mL, with some patients having significantly low levels (as low as 11.7 ng/mL). This suggests a need for monitoring and possibly supplementing Vitamin D in these patients. For the non-statin group, the average Vitamin D level is 19.25 ng/mL, with a notable variation, including some patients having levels as low as 9.6 ng/mL. Both groups indicate the importance of addressing Vitamin D deficiency.
- Total Cholesterol: The average total cholesterol level for patients on statins is 170.44 mg/dL. Notably, some patients have high cholesterol levels, such as a patient with 216 mg/dL. In the non-statin group, the average total cholesterol level is higher at 184.45 mg/dL, with some patients having very high levels, such as a patient with 295 mg/dL. This suggests more stringent cholesterol management is necessary for the non-statin group.
- Triglycerides (TG): The average triglyceride level for the statin group is 102.89 mg/dL, with some patients having elevated levels. The non-statin group has a higher average triglyceride level of 128.82 mg/dL, indicating potential risk factors for cardiovascular issues. This calls for enhanced monitoring and lifestyle interventions to manage triglyceride levels.
- HDL (Good Cholesterol): The average HDL level for the statin group is 52 mg/dL, with a range from 37 mg/dL to 66 mg/ dL. For the non-statin group, the average HDL level is higher at 61 mg/dL. Higher HDL levels are generally beneficial, and efforts should be made to maintain or increase these levels through diet and exercise.
- LDL (Bad Cholesterol)
- The average LDL level for both groups is the same at 99 mg/dL. This indicates a need for continuous monitoring and management to prevent elevated LDL levels and associated cardiovascular risks.
- Blood Pressure (BP): In the statin group, the average diastolic BP is 65 mmHg, and the average systolic BP is 124.9 mmHg. This shows generally controlled blood pressure. In the non-statin group, the average diastolic BP is 74 mmHg, and the average systolic BP is 120.4 mmHg, indicating well-controlled blood pressure as well.
- BMI: The average BMI for the statin group is 31.86, which falls into the overweight category. For the non-statin group, the average BMI is higher at 36.83, indicating obesity. This underscores the importance of weight management and lifestyle interventions for both groups.
The study’s findings aligned with recent research indicate that Vitamin D supplementation does not significantly reduce cardiovascular risk. For example, a 2024 study found that Vitamin D supplementation did not significantly reduce cardiovascular risk. Potential mechanisms by which Vitamin D deficiency might influence cardiovascular health include its role in regulating calcium metabolism, inflammation, and endothelial function.
The D-Health Trial, a large-scale, randomized controlled trial conducted by the QIMR Berghofer Medical Research Institute in Australia, further supports these findings. The trial involved over 21,000 participants aged 60-84 years and found that monthly doses of Vitamin D did not significantly reduce the rate of major cardiovascular events compared to a placebo. This trial highlights the need for further research to understand the mechanisms by which Vitamin D influences cardiovascular health and to develop effective interventions.
The study’s limitations include the small sample size and the lack of detailed statistical analysis due to ongoing data collection. Future research should address these limitations by expanding the sample size and conducting more comprehensive statistical analyses.
Conclusion
The study highlights several health challenges faced by both patient groups, including Vitamin D deficiency, elevated cholesterol and triglyceride levels, and high BMI. Statin users tend to be older, and the medication is more prevalent among females. Although both groups have well-controlled blood pressure, BMI and cholesterol management remain critical areas for improvement. This study emphasizes the importance of monitoring Vitamin D levels in African American patients and those with cardiovascular issues.
Key recommendations include:
- Regular monitoring of Vitamin D levels and supplementation to address deficiencies.
- Managing cholesterol levels through dietary changes, physical activity, and medications.
- Emphasizing lifestyle interventions such as a healthy diet and regular exercise to control triglyceride levels.
- Implementing weight management programs to assist patients in attaining a healthier BMI.
- Continuous monitoring of cholesterol, triglyceride levels, blood pressure, and BMI to prevent cardiovascular diseases.
- Tailored interventions to address the unique health needs of males and females in both groups.
- Encouraging patients to undergo regular health check-ups to detect and manage potential health issues early on.
- Educating patients on the importance of maintaining a balanced diet rich in vitamins and minerals to support overall health.
- Providing mental health support and counselling to help patients cope with stress and improve their overall well-being.
- Developing social and behavior change programs to raise awareness about the significance of cardiovascular health and the role of Vitamin D.
- Initiating education and promotion programs to inform patients about the benefits of proper nutrition, physical activity, and regular medical check-ups.
- Implementing nutrition programs that focus on incorporating essential nutrients, such as Vitamin D, into daily diets to support heart health and overall well-being.
While the findings suggest potential benefits from Vitamin D supplementation, further research is essential to establish clear guidelines. Clinicians are encouraged to assess baseline Vitamin D levels in at-risk populations and provide appropriate supplementation based on evidence-based practice.
References
- Thompson B, Waterhouse M, English DR, McLeod DS, Armstrong BK, et al. (2023) Vitamin D supplementation and major cardiovascular events: D-Health randomised controlled trial. BMJ 381: e075230.
- Vitamin D Recommendations: Are current vitamin D recommendations enough for heart health? Knowledge. January 26, 20253.
- Vitamin D and Type 2 Diabetes: Almost half of people with type 2 diabetes are vitamin deficient. Everyday Health. January 29, 20254.
- Elamin MB, Abu Elnour NO, Elamin KB, Fatourechi MM, Alkatib AA, et al. (2011) Vitamin D and cardiovascular outcomes: a systematic review and meta-analysis. J Clin Endocrinol Metab 96: 1931-1942.
- Gupta A, Thompson PD (2011) The relationship of vitamin D deficiency to statin myopathy. Atherosclerosis 215: 23-29.
- Michos ED, Martin S, Jones S (2013) 25- hydroxyvitamin D levels and lipoprotein cholesterol subfractions: the very large database of lipidsvitamin D study. J Am Coll Cardiol 61: E1452.
- Milewicz A (2012) Obesity, carbohydrate, lipid metabolism and polymorphisms (Fok, Bsm) of vitamin D receptor gene in aging population: POLSENIOR study.
- Pittas AG, Chung M, Trikalinos T, Mitri J, Brendel M, et al. (2010) Systematic review: vitamin D and cardiometabolic outcomes. Ann Intern Med 152: 307-314.
- Ponda MP, Huang X, Odeh MA, Breslow JL, Kaufman HW (2012) Vitamin D may not improve lipid levels: a serial clinical laboratory data study. Circulation 126: 270-277.
- Rajakumar K, de las Heras J, Chen TC, Lee SJ, Holick MF, et al. (2011) Vitamin D status, adiposity, and lipids in Black American and Caucasian children. J Clin Endocrinol Metab 96: 1560-1567.
- Vanga SR, Good M, Howard PA, Vacek JL (2010) Role of vitamin D in cardiovascular health. Am J Cardiol 106: 798-805.
- Shahar DR, Schwarzfuchs D, Fraser D, Vardi H, Thiery J, et al. (2010) Dairy calcium intake, serum vitamin D, and successful weight loss. Am J Clin Nutr 92: 1017-1022.
- Wang L, Manson JE, Song Y, Sesso H (2010) Systematic review: Vitamin D and calcium supplementation in prevention of cardiovascular events. Ann Intern Med 152: 315-323.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.