Total Implantable Venous Access Devices: Single Incision for Implantation via Cephalic/Subclavian Vein. SingleSurgeon Experience
by Barba A*
Department of Angiology and Vascular Surgery. IMQ Zorrotzaurre University Hospital. Bilbao. Basque Country. Spain
*Corresponding Author: Ángel Barba, Angiology and Vascular Surgery Department. IMQ Zorrotzaurre University Hospital. Bilbao. Basque Country. Spain
Received Date: 10 March 2026
Accepted Date: 13 March 2026
Published Date: 16 March 2026
Citation: Barba Á (2026) Total Implantable Venous Access Devices: Single Incision for Implantation via Cephalic/Subclavian Vein. Single-Surgeon Experience. J Surg 11: 11583 DOI: https://doi.org/10.29011/2575-9760.011583
Abstract
Background: The purpose of this study is to present the outcomes of a single incision intervention in the deltopectoral fold for the implantation of Total Implantable Venous Access Devices (TIVADs) via the Cephalic Vein (CV) or the Subclavian Vein (SV).
Methods: Preoperative ultrasound of the CV in the deltopectoral fold was carried out. The Cephalic Vein Cut-Down (CVC) technique was used for implantation via the CV, and the Anatomical Landmarks Technique (ALT) was used for Subclavian Vein Puncture (SVP). This is a description of the surgical technique and the results obtained between 2008 and 2025.
Results: A total of 1300 TIVADs implanted in 1249 patients were studied; 781 were women (62.5%). The mean age was 62.4±11.6 years, and was higher in men than in women. In 68 (5.2%) cases, there was no CV; the mean diameter of the CV in the remaining cases was 3.8± 0.5 mm, and the mean depth was 13.7± 6.7 mm. In 1084 cases (83.4%), the implant was placed on the left side, and in 886 cases (81.7%) via CVC. The mean operative time was 23.3±3.6 minutes. Success rates were 99.6% for both CVC and SVP. There were 15 (1.2%) intraoperative complications: 4 (0.4%) via CVC and 11 (5.0%) via SVP. There were 12 (0.9%) postoperative complications: 6 (0.6%) via CVC and 6 (2.7%) via SVP, the most frequent being deep vein thrombosis (0.4%). Complications were significantly lower on the left side (1.6%, n=17) than on the right side (4.7%, n=10).
Conclusions: The single-incision approach is suitable for both CVC and ALT routes. CVC is a technique with an excellent success rate and minimal complications. Left-sided implantation presents fewer complications than right-sided implantation.
Keywords: Cephalic Vein Cut-Down; Total Implantable Venous Access Devices; Single incision
Introduction
Two key historical moments for the implantation of Total Implantable Venous Access Devices (TIVADs) were that until the 1960s/70s, Cephalic Vein Cut-Down (CVC) in the deltopectoral fold was the primary route for pacemaker implantation [1], and that in 1982 Niederhuber implanted the first TIVAD via CVC in this location [2]; in both cases, a single incision was made. The other main route for TIVAD implants is the subclavian vein, following the technique described by Seldinger [3] in 1953.
However, in this case, two incisions are made, either via the infraclavicular approach described by Aubaniac [4] in 1952 or the supraclavicular approach by Yoffa [5] in 1965. Until the end of the 20th century, the Subclavian Vein Puncture (SVP) technique using anatomical landmarks was usually carried out ‘blind’, without direct visualization of the vessel. However, from that point onward, intraoperative ultrasound was used to localize the vessel, thereby increasing success rates and decreasing complications. Before beginning to implant TIVADs in our setting, a literature review was conducted, revealing two key findings: that the success rate with the CVC technique was less than 85% in most series [6], with lack of success due to alterations or absence of the Cephalic Vein (CV), and that ultrasound imaging improved these rates [7]. Therefore, from the outset of this study, all patients scheduled for TIVAD implantation underwent preoperative ultrasound imaging of the CV. This study aims to demonstrate that a TIVAD can be implanted with a single incision via both CVC and SVP, and that the preoperative use of CV ultrasound significantly increases CVC success rate and reduces postoperative complications.
Methods
This is a retrospective observational cohort design study carried out between 2008 and 2025 in the Oncology Department of the private IMQ Zorrotzaurre Hospital in the Basque Country (Spain), which covers a population of 250,000 inhabitants. The protocol followed for the implants was the preoperative measurement of the diameter, depth, and characteristics of the cephalic vein in both upper extremities using a MyLab50 color Doppler ultrasound (Esaote). If the diameter was ≥3.2 mm, the implant was performed via CVC, as this diameter corresponds approximately to the 9.6F gauge of the catheter used in this work, a NuPort HP* System (PHS MEDICAL) with a single-chamber titanium port and silicone catheter. Otherwise, implantation was performed using the SVP technique. For this approach, a 21-gauge needle from a Micropuncture set (AngioDynamics) was first used to cannulate the vein, followed by the NuPort set. Intraoperative radiological monitoring was performed using a BV Bracelet (Philips). All patients had a preoperative anesthetic evaluation deemed suitable for the procedure and were informed about the technique to be performed; they subsequently signed the corresponding informed consent form.
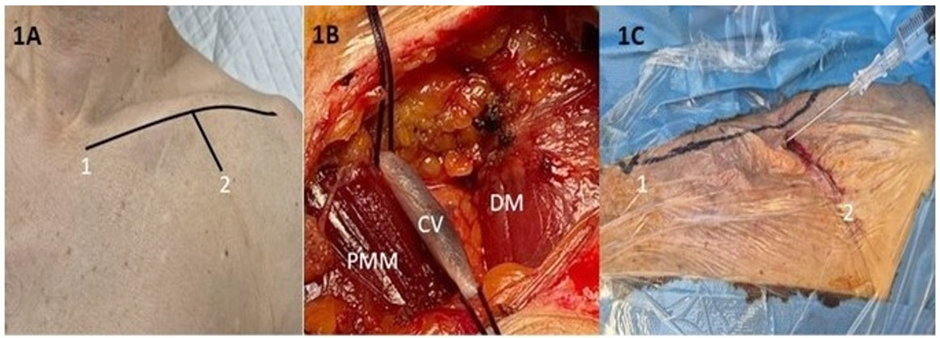
Figure 1: Surgical Technique. 1A: Inferior border of clavicle (1) and incision in the deltopectoral groove (2) - 1B: Cephalic Vein (CV) dissection - DM: Deltoid Muscle- PMM: Pectoralis Major Muscle -1C: Subclavian Vein Access by Anatomical Landmarks
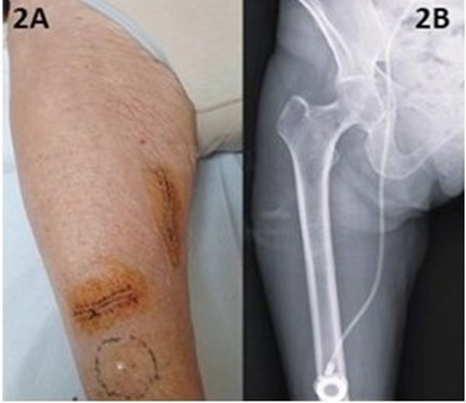
Figure 2: Implant via Great Saphenous vein; 2A: Surgical technique -2B: Radiographic Control
To determine if there were any differences in the procedures, the results were divided into two time periods: 2008–2016 and 2017– 2025. Finally, it should be noted that all ultrasound explorations and implantations were performed by the same vascular surgeon. For the statistical analysis, the baseline characteristics of the study groups used means with their corresponding Standard Deviations (SD) for continuous variables, and frequencies and percentages for categorical variables. Differences between sexes were compared according to sociodemographic, clinical variables and vein characteristics. Differences in operating time and complications between periods (2008-2016 versus 2017-2025) were compared. If the compared variable was numerical, the Wilcoxon rank-sum test was used, since data was not normally distributed, and if the variable was categorical, Chi-squared or Fisher’s exact test was used, as appropriate. Statistical significance was set at P value ≤ 0.05 and statistical analysis was performed by using RStudio® version 4.3.1.
Results
From January 2008 to December 2025, 1300 TIVADs were implanted in 1249 patients, with 51 patients (4.1%) receiving 2 or 3 TIVADs. 62.5% were women, and the mean age was 62.4
years, and significantly higher in men than in women. Colorectal cancer was the most frequent type of neoplasia in men (39.3%), while breast cancer was the most frequent type in women (44.6%). 151 patients (12.1%) had had a previous neoplasm; 63 were men, with urological cancers the most frequent (34 cases, 54.0%), and 88 were women, with gynecological cancers the most frequent (19 cases, 21.6%) (Table 1).
Table 1: General Characteristics.
|
All |
Male |
Female |
P |
|
|
Gender, n (%) |
1249 (100) |
468 (37.5%) |
781 (62.5%) |
<0.0001 |
|
Age, years (mean ± SD) |
62.4± 1.6 |
65.9±11.0 |
60.4±11.4 |
<0.0001 |
|
Neoplasm location, n (%) |
||||
|
Oropharyngeal |
41 (3.3) |
27 (5.8) |
13 (1.7) |
<0.0001 |
|
Colorectal |
365 (29.2) |
184 (39.3) |
181 (23.2) |
<0.0001 |
|
Gastroesophageal |
100 (8.0) |
65 (13.9) |
35 (4.5) |
<0.0001 |
|
Hematologic |
24 (1.9) |
12 (2.6) |
12 (1.5) |
0.0333 |
|
Hepatopancreatic |
102 (8.2) |
55 (11.8) |
47 (6.0) |
<0.0001 |
|
Breast |
367 (28.0) |
2 (0.4) |
348 (44.6) |
<0.0001 |
|
Reproductive organ |
82 (6.6) |
13 (2.8) |
69 (8.8) |
<0.0001 |
|
Lung |
126 (10.1) |
67 (14.3) |
60 (7.7) |
0.0013 |
|
Urologic |
36 (2.9) |
32 (6.8) |
4 (0.5) |
<0.0001 |
|
Other |
23 (1.8) |
11 (2.4) |
12 (1.5) |
0.3194 |
|
Previous neoplasm, n (%) |
151 (12.1) |
63 (13.5) |
88 (11.3) |
0.2963 |
SD: Standard Deviation
Both the diameter and mean depth of the CVs were significantly larger in men. The CV was absent in 5.2% of the scans, and in 59 cases (4.5%), some anomaly was found that would prevent subsequent implantation via CVC, with crossing stenosis the most frequent, occurring in 3.5% of the scans. In 4 patients (0.3%), ultrasound studies were not performed because implantation via RGSV was chosen. Ultimately, 1074 CVs (82.8%) were candidates for CVC implantation and 222 (17.2%) for SVP implantation (Table 2).
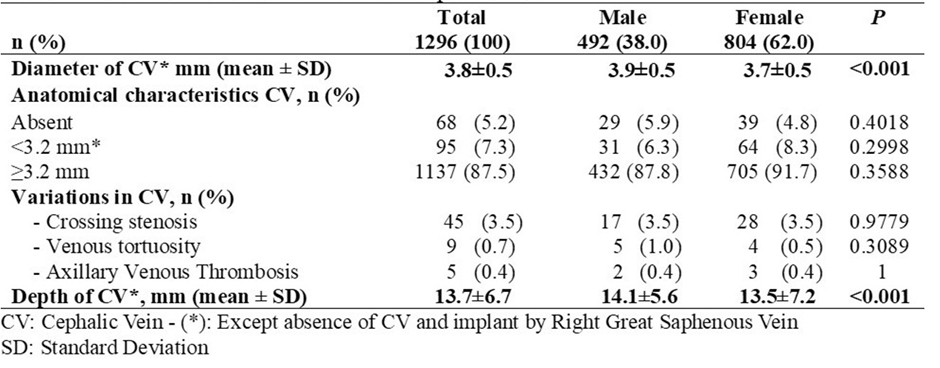
Table 2: Anatomical Characteristics of the Cephalic Veins.
The results were classified according to the recipient vein, the side of the implant, and the implantation period. In 1084 cases (83.4%), the TIVAD was implanted via left venous access, and of these, 81.7% were via CVC. Two hundred and twelve TIVADs were implanted on the right side, and the main reasons for this were previous breast surgery with left lymphadenectomy in 118 cases (55.7%) and previous TIVAD implantation via a left-sided SVP in 51 cases (24.1%). Thirty patients were left-handed, representing 14.2% of the implants and 2.4% of the overall study population. Four TIVADs (0.3%) were implanted via the right great saphenous vein, all in women due to venous and/or lymphatic pathology in both upper extremities. Table 3 presents the distribution of surgical time and access routes by period, showing that procedures are significantly shorter in the 2017-2025 period, but access routes do not show major differences.
There were 1065 TIVADs scheduled via CVC (81.9%), but on 4 occasions (0.4%) surgery could not be performed due to a large irreversible spasm of the CV, resulting in a 99.6% success rate. Of the 231 implanted via SVP (17.5%), 227 were scheduled, and 4 were CVC reversals. On one occasion (0.4%), a significant arterial injury occurred that required endovascular repair and the implant was discontinued, resulting in a 99.6% success rate for both techniques (Table 3).
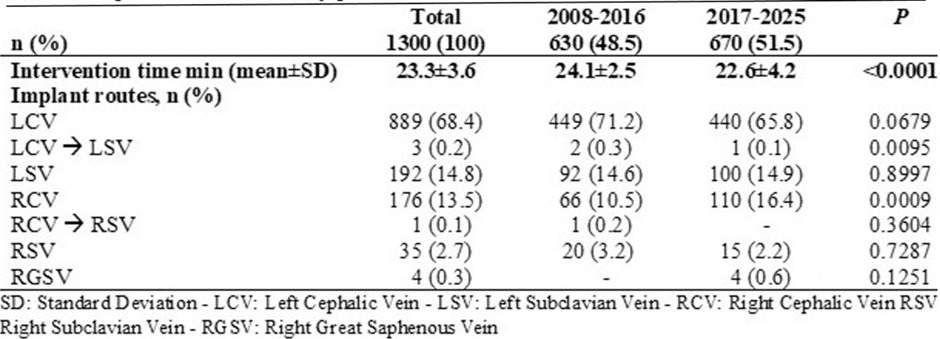
Table 3: Impalant access routes by period.
There were 27 complications (2.1%), 15 (1.2%) of which were intraoperative and 12 (0.9%) postoperative. Of the 15 intraoperative complications (1.2%), 4 (0.3%) were from CVCs and 11 (4.7%) from SVPs, of which SVP complications were significantly more frequent, primarily due to pneumothorax. Six (0.5%) patients were men and 9 (0.7%) were women. Furthermore, 10 (0.9%) complications occurred on the left side compared to 5 (2.4%) on the right, a statistically significant difference (p < 0.005).
Of the 12 postoperative complications, 5 occurred in men (0.4%) and 7 in women (0.5%), while 7 (0.6%) occurred on the left side and 5 (2.4%) on the right, also a statistically significant difference (p < 0.005). The main postoperative complication was ipsilateral subclavian DVT (1.7%), which, although more frequent with SVPs, was statistically significant. In the overall count, complications were significantly higher for SVP (Table 4). No complications occurred with RGSV implantation.
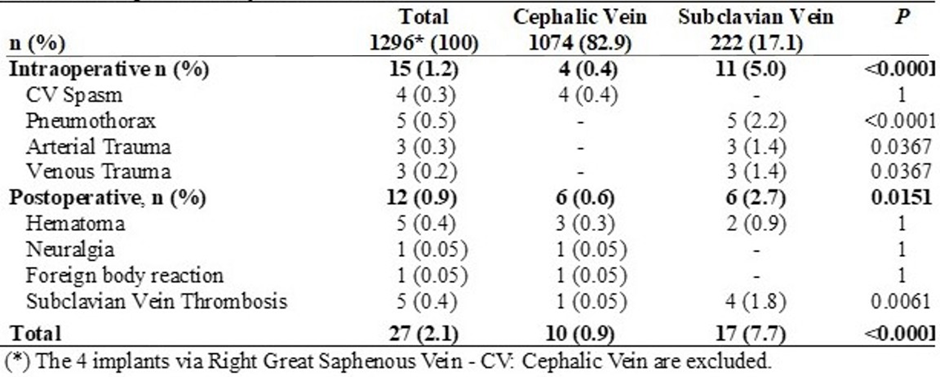
Table 4: Complications by Access Route.
Finally, no significant differences were found in complications related to the time periods (Table 5), although a significant decrease in all complications was observed in the second period.
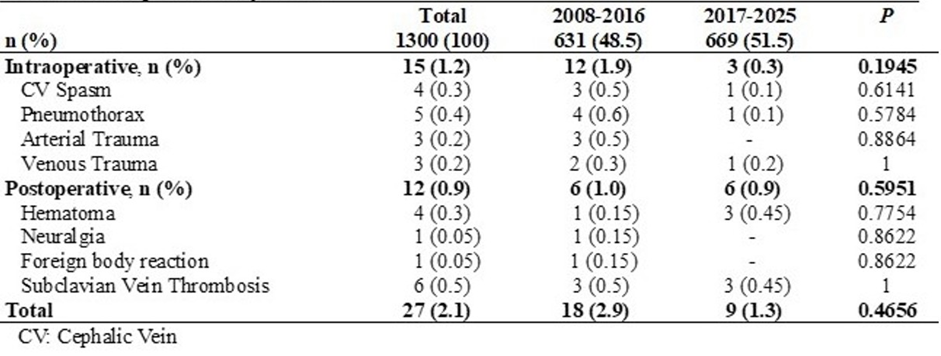
Table 5: Complications by period
Discussion
Although authors such as Atti [6] state that CVC is the best route for pacemaker implantation and consequently for TIVAD, in the current literature, for many, such as Kilic [7], this route does not even exist. This is primarily due to two factors: first, the numerous non-surgical
specialists now involved in TIVAD implantation (e.g. radiologists, anesthesiologists, oncologists); and second [8], the anatomical alterations of the cephalic vein (e.g. absence, small size, beaded veins) observed during implantation, which in some cases reached 18.3% due to absence or small caliber [9], and in the present study is 9.8%. This second factor favored implantation via SVP due to the low success rate and the high conversion rate of CVC [10]. As has been demonstrated, performing preoperative ultrasound reduces complications and increases the success rate. In terms of the laterality of the implant, although approximately 10% of the population is left-handed [11] and in this study 14%, left CVC is the preferred approach primarily because the catheter curve is much smaller than on the right side, which reduces the number of kinks. Furthermore, in right-handed patients, continuous limb movement and alterations in the costoclavicular space tend to cause pinch-off syndrome [12,13]. In the literature consulted, authors who perform a single incision in the deltopectoral fold for CVC implantation make it more distal to the clavicle, while for the other approaches, they use two incisions, generally on the right side [14]. With a single, high incision, as shown in Figure 1, the CV and SV are easily accessed without the need for two incisions. The same literature search did not find any published studies in which a TIVAD was implanted via RGSV. When implantation was performed blind via CVC, the success rate of this approach did not exceed 85% [15]. However, with the use of preoperative ultrasound, this rate approached excellence (>95%), as demonstrated first by Otsubo [16] when comparing the two CVC techniques with and without preoperative ultrasound: 97.2% versus 87.2%, and subsequently by the PORTAS-3 study [10]. In the present study, the success rate was 99.6%. There are significant differences in surgical time, presumably depending on the definitions used. Di Carlo [17] is the most skilled and fastest, with a time of 15 minutes, while Hataoka [8] reports a time of 53 minutes. In the present study, the mean time was 23.3 minutes.
No studies were found comparing complication rates across various time periods, but based on the results of this study, it can be stated that experience improves outcomes by increasing the success rate and decreasing complications, although not significantly. A review of the literature revealed only two studies comparing CVC and SVP access routes with success rates and intraoperative and postoperative complications. Both Pérez [18] and Otsubo [16] concluded that the success rate is higher with SVP, but that both intraoperative and postoperative complications are lower with CVC, as is the case in this study. It should be noted that DVT is the most significant postoperative complication, sometimes requiring TIVAD explantation. Studies such as Knorr’s [19], involving 2703 patients who underwent pacemaker implantation via both CVC and SVP, concluded that CVC implantation results in fewer DVT events in the SV than via SVP, as did the present study. It should be noted that in none of the reviewed studies was CV spasm considered a complication for CVC implantation; however, it was included here because it necessitated a change in access route. Had it not been included as an intraoperative complication, the success rate would have been 100%, and intraoperative complications would have been 0.0%. Finally, we agree with the meta-analysis by Klaiber [10] comparing CVC and SVP implantation that “when comparing techniques, the percentage of complications is more important than the success rate”.
Conclusion
We affirm that a single incision for TIVAD implantation via CVC or SVP is a simple technique requiring little surgical time. CVC with preoperative ultrasound has a success rate equal to SVP with or without intraoperative ultrasound. Both intraoperative and postoperative complications of CVC with preoperative ultrasound are lower than those of SVP in this study.
Declarations
Declaration of conflicting interests:
The author declares that they have no competing interests.
Funding: The author received no financial support for the research, authorship, and/or publication of this article
References
- Parsonnet V (1999) The Cephalic Vein Cutdown Versus Subclavian Puncture for Pacemaker/ICD Lead Implantation. Pacing and Clinical Electrophysiology 22: 695-697.
- Niederhuber JE, Ensminger W, Gyves JW, Liepman M, Doan K, et al. (1982) Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery 92: 706-712.
- Seldinger SI (1953) Catheter Replacement of the Needle in Percutaneous Arteriography: A New Technique. Acta Radiologica 39: 368-376.
- Aubaniak CR (1952) L’injection intraveineuse sous-claviculaire; avantages et technique 60: 1456.
- Yoffa D (1965) Supraclavicular subclavian venepuncture and catheterisation. Lancet 2: 614-617.
- Atti V, Turagam MK, Garg J, Koerber S, Angirekula A, et al. (2020) Subclavian and Axillary Vein Access Versus Cephalic Vein Cutdown for Cardiac Implantable Electronic Device Implantation: A MetaAnalysis. JACC Clin Electrophysiol 6: 661-671.
- Kılıç B, İlhan B, Karanlık H (2025) Totally implantable venous access devices: A fifteen-year single-center experience. Eur Res J 11: 260269.
- Hataoka T, Sanmoto Y, Kinuta S (2024) Cephalic Vein Cut-Down Method for Totally Implantable Venous Access Ports: A SingleInstitution Experience. Ann Vasc Surg 98: 244-250.
- Rademakers LM, Bracke FA (2021) Cephalic vein access by modified Seldinger technique for lead implantations. Pacing Clin Electrophysiol 44: 607-613.
- Hüttner FJ, Bruckner T, Hackbusch M, Weitz J, Bork U, et al. (2020) Primary Open Versus Closed Implantation Strategy for Totally Implantable Venous Access Ports: The Multicentre Randomized Controlled PORTAS-3 Trial (DRKS 00004900). Ann Surg 272: 950960.
- Ocklenburg S (2024) The Lateralized Brain: The Neuroscience and Evolution of Hemispheric Asymmetries.Academic Press 2024
- Norese, M, Andersen, Sinagra D (2021) Fractura de catéter implantable con reservorio por síndrome de pinch-off. Revista Argentina de Cirugía 113: 258-262.
- Ben Kridis W, Toumi N, Khanfir A (2020) Causes of Fracture at Catheter of Totally Implantable Venous Access Port: A Systematic Review. Acta Med Iran 57: 686-689.
- Mu C, Zhu Z, Miao D, Wu Q, Chen L, et al. (2025) Clinical efficacy and safety of a new single-incision axillary vein puncture technique for totally implantable venous access ports. Sci Rep 15: 7281.
- Klaiber U, Grummich K, Jensen K, Saure D, Contin P, et al. (2015) Closed cannulation of subclavian vein vs open cut-down of cephalic vein for totally implantable venous access port (TIVAP) implantation: protocol for a systematic review and proportional meta-analysis of perioperative and postoperative complications. Syst Rev 4: 53.
- Otsubo R, Hatachi T, Shibata K, Yoshida T, Watanabe H, et al. (2016) Evaluation of totally implantable central venous access devices with the cephalic vein cut-down approach: Usefulness of preoperative ultrasonography. J Surg Oncol 113: 114-119.
- Di Carlo I, Cordio S, La Greca G, Privitera G, Russello D, et al. (2001) Totally implantable venous access devices implanted surgically: a retrospective study on early and late complications. Arch Surg 136: 1050-1053.
- Pérez Calvo J, Castellví Valls J, Crusellas O, Petrone P (2020) Comparative study of access routes for Port-A-Cath® implantation. Cir Esp (Engl Ed) 98: 79-84.
- Knorr D, Bandorski D, Bogossian H, Iliodromitis K, Schiedat F, et al. (2024) Cephalic Vein Cutdown Is Superior toSubclavian Puncture as VenousAccess for Patients with CardiacImplantable Devices after Long-Term Follow-Up. J. Clin. Med 3: 1044.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.