The Utilization of a Topical Nitric Oxide Generating Serum in Aesthetic Medicine
Gregory Chernoff BSc, MD, FRCS(C)*
Private Practice, Chernoff Cosmetic Surgeons, Ascension St. Vincent Hospital, Indianapolis IN, USA
*Corresponding author: Gregory Chernoff, Private Practice, Chernoff Cosmetic Surgery, Ascension St. Vincent Hospital, Indianapolis IN, USA
Received Date: 18 August, 2020; Accepted Date: 24 August, 2020; Published Date: 28 August, 2020
Citation: Chernoff G (2020) The Utilization of a Topical Nitric Oxide Generating Serum in Aesthetic Medicine. J Surg 5: 1329. DOI: 10.29011/2575-9760.001329
Abstract
Key Points:
1. A Nitric oxide serum can be safely formulated without the generation of nitric dioxide and is necessary for optimal cellular health.
2. Nitric oxide serum can be topically applied for many cosmetic purposes, and also has anti-inflammatory and ant-bacterial properties.
3. Nitric oxide is a free radical gas. It is produced endogenously and is synthesized from arginine by nitric oxide synthase.
4. Nitric oxide mediates vasodilation, inhibits platelet aggregation, induces disaggregation of aggregated platelets, and inhibits platelet adherence to endothelial cells. As a result, Nitric oxide is a potent vasodilator, and increases blood flow via capillary recruitment.
5. Topical Nitric Oxide Serum by itself, yields improvement in fine lines and wrinkles, and enhances the tone, texture of the skin.
6. When used prior to any other topical, the vasodilatory property primes the skin to enhance the absorption of other products.
Methods: One hundred patients were enrolled into a two center, multi-limb study. Ages ranged from 15 to 76 years. The effect of a Nitric Oxide generating topical serum was studied on 100 patients in two Centers between December 2018 and December 2019. There were 82 females and 18 males. The population consisted of 42 Caucasian, 18 Asian, 8 African American, 12 Hispanic, 14 Mediterranean, and 6 Indian patients.
Patients were enrolled under four categories: 1) Aging Skin; 2) Acne; 3) Scar Therapy; and 4) Wound Care. The Aging skin population utilized NO serum bid after cleansing. Photographs were taken monthly for 4-12 weeks. Linear analog scales were administered examining skin tone, wrinkles, clarity and color variation. No other products were used concomitantly.
The Active acne patients were divided into mild, moderate and severe states based on nodule and pustule counts. NO serum was applied am and pm after cleansing. Photographs were taken weekly for 4-12 weeks. Pustule and nodule counts were recorded weekly. NO serum was applied bid in the treatment of atrophic scars, striae, acne scars, hypertrophic scars post Needle Radiofrequency, and around the CO2 laser excised keloid scar beds. Photographs were taken weekly for 4-12 weeks. Several wound types were examined: Surgical incisions, healing surgical flaps, diabetic ulcers, and smoking induced, vascular compromised skin. NO serum was applied qid daily. Photographs were taken at 4, 8, and 12 weeks.
Results: The Aging skin population reported improvement in fine lines, wrinkles, pore size, skin tone and texture, coloration and oiliness. A high level of product satisfaction with significant improvement in self-esteem was noted. The Acne population showed a range in pustule and nodule reduction ranging from 20% to 84%. The average reduction was 68%. The Scar therapy population showed positive trends. The atrophic scar patients and those with striae improved the most. Softening of hypertrophic scar tissue was noted. Keloid wound beds healed anecdotally faster than non-treated patients. Improved vascularity is speculated. The Wound healing population without exception showed excellent results. Rhytidectomy, Blepharoplasty, and Rhinoplasty patients displayed less bruising, edema, and more rapid healing. Non-healing ulcers healed within 30-45 days. Revascularization was routinely evident in compromised flaps.
Conclusion: It is possible to deliver clinically relevant bioactive nitric oxide via a dual chamber NO generating delivery device. This Pilot Study shows valid proof of concept to warrant further IRB approved studies in the areas of aging skin, acne, wound healing and scar therapy.
Keywords
Nitric oxide; Regenerative medicine; Topical applications
Introduction
Nitric Oxide (NO), is an important biological messenger in human physiology. This multifunctional signaling molecule takes part in the control of vasodilation [1], and is involved in the inhibition of platelet aggregation and platelet adhesion to vascular endothelium [2,3]. Several human skin studies have indicated that NO is involved in the proliferation and differentiation of epidermal cells, regulation of innate immune reactions and inflammatory responses, the control of allergic skin manifestations, microbicidal activity, and antigen presentation [4,5]. NO is also a key molecule in wound healing regulation and tissue regeneration due to its gene regulatory properties, as well as its influence on the proliferation and differentiation of fibroblasts, keratinocytes, monocytes and macrophages [6-13].
Bryan has written extensively on the science of NO and the importance of NO in human health [14-16]. By the age of 40, most adults produce only 50% of the NO produced endogenously at the age of 20. Studies have shown that diminished NO can be an early marker of chronic disease. Given the importance of NO and its’ natural depletion over time, research was performed yielding the subsequent development of a patented NO lozenge, Neo40 (humanN, Austin TX). Peer-reviewed, placebo- controlled studies demonstrated that the NO lozenge could modify cardiovascular risk factors in patients over age 40, reduce triglycerides, and reduce blood pressure. These studies demonstrate the safety and efficacy of restoring NO production in humans. The importance of nitric oxide in cellular medicine, regenerative and stem cell therapy has also been highlighted in the literature [17]. The role of NO in stem cell biology is revealing novel strategies for NO repletion prior to, during, and after stem cell deployment, exosome administration, in order to optimize metabolism for regenerative or healing outcomes.
NO is a short-lived free radical produced enzymatically by Nitric Oxide Synthase (NOS) endogenously. NOS converts the amino acid precursor L-arginine to NO and L-citrulline with the help of several co-factors such as tetrahydrobiopterin, Flavine Mononucleotide (FMN), Flavine Adenine Dinucleotide (FAD), Nicotinamide-Adenine-Dinucleotide Phosphate (NADHP) and an oxygen molecule [18,19]. Nitric oxide is synthesized and released by many skin cells including fibroblasts, keratinocytes, melanocytes, endothelial cells, macrophages, neutrophils, and adipocytes [20-28]. NO is a hydrophobic molecule with a stoke radius of 3-4A that can diffuse across most biological membranes.
Given the success of oral repletion, many studies also looked at topically applied NO generating formulations. The diffusion coefficient of NO has been shown to be comparable to other small diatomic molecules such as dioxygen or carbon monoxide [29]. A diffusion distance of 500 microns was estimated for NO in tissues [29]. This is sufficient for NO to penetrate the dermis and reach the microcirculation of the upper horizontal plexus, and the upper dermis after topical application [30]. EPR spectroscopy studies using an acidified - 15N-labelled nitrite confirmed a transcutaneous absorption of 15,000 ppb NO to 3mm into human dermis [31,32]. The transcutaneous application in vivo of a formula generating NO, was shown to significantly increase circulatory nitrite and S-nitroso-concentrations resulting in improvement of hemodynamic parameters [32]. These included increased blood flow, reduced platelet aggregation, and a decrease in arterial blood pressure.
In the Aesthetic and Reconstructive patient population, the dermal application of a NO generating serum has a wide range of potential uses. The “aging skin” population would benefit from improved circulation and absorption of fibroblast enhancing ingredients. The “Acne prone” and the “COVID” mask-induced dermatitis” patient would benefit from the anti-bacterial benefits of NO [32,33]. Other chronic fungal or viral inflictions could also see benefit. Diabetic ulcers plague millions of patients yearly. NO formulations, improving circulation in this population would prove life-changing [34]. Other “compromised” circulation conditions such as Raynaud’s Syndrome [35], and Localized Sclerosis [36] have seen benefit. Cutaneous skin cancer at times requires partial thickness grafts, full thickness grafts, local flaps, regional flaps or free flaps for reconstruction. The concomitant application of a NO delivery serum would improve the donor site and recipient site prior, during and after graft or flap reconstruction [37].
This study looks at the potential application of a novel “Patent Pending” dual chamber delivery system serum, (Pneuma Nitric Oxide; Austin, TX) which produces NO in clinically sufficient dosage and decay profile to examine its’ benefit in the Facial Aging, Acne, Wound Healing, and Scar Therapy patient populations.
Study Population
The effect of a Nitric Oxide generating topical serum was studied on 100 patients in two Centers between December 2018 and December 2019. There were 82 females and 18 males. The population consisted of 42 Caucasian, 18 Asian, 8 African American, 12 Hispanic, 14 Mediterranean, and 6 Indian patients.
Exclusion criteria in this study included an unwillingness to avoid excessive sunlight or wear protective clothing and sunscreen, unwillingness to forgo any other topical dermatological or drug therapy, the use of topical corticosteroid, alpha and beta-hydroxy acids, retinoids, or vitamin C containing topicals within 30 days before, as well as throughout the course of the study. Washout periods adhered to by subjects in this study included 6 months free from dermabrasion, deep chemical peels, ablative laser treatments, neurotoxin or filler injections: 3 months free from non-ablative laser, light, radiofrequency or ultrasound treatments; and 1 month free from microdermabrasion, light and medium depth peels.
Methods
A novel “Patent Pending” NO generating dual chamber mixing serum was examined for preliminary efficacy and proof of concept. Nitric oxide was detected and quantified using an ozonebased gas phase Chemiluminescent Detector (CLD) (EcoPhysics, Michigan USA). Contents of both chambers of the NO generating serums were dispensed and mixed on the skin. The CLD detector was placed within one inch from the skin after contents from both chambers of the product were mixed, nitric oxide gas was released, and detected. Initial nitric oxide levels reached over 15,000 ppb during the mixing period and then exhibited normal decay kinetics. Nitric oxide could still be detected emitting from the skin 30 minutes after the initial application. The efficacy was evaluated by visual and instrumental methods at 4- week intervals over a 12 week period.
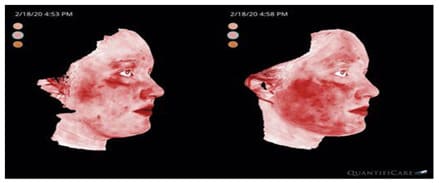
One hundred patients were enrolled into a two center multilimb study. Patients were enrolled under four categories: Aging Skin (40 patients), Active Acne (30 patients), Scar Therapy (15 patients), and Wound Care (15 patients). The Aging Skin population used the NO serum morning and evening after cleaning their skin with a gentle cleanser. Photographs were taken at 4- week intervals for 12 weeks. Patient linear analog scales were administered. Tissue attributes examined included wrinkles, pores, skin clarity, quality, and pigmentation. Patients were also given a linear analog examining product satisfaction. Quantification of wrinkle improvement, pore size, oiliness, evenness, red spots and brown spots were calculated using 3-dimentional image analysis of LifeViz App (QuantifiCare, France) and then compared to QuantifiCare’s reference population database of normal aging skin: adjusted for age, sex, and skin type; the 3-dimentional high resolution micro-imaging of skin surface of those participants were taken using a micro imaging system (Quantificare, France).
The Active Acne population was divided into mild, moderate and severe based upon nodule and pustule counts. The NO serum was applied morning and evening after cleaning their skin with a gentle cleanser. Photographs were taken weekly for 30 days. Pustule and nodule counts were recorded weekly. Linear analog scales were administered. The Scar Therapy population consisted of atrophic scars, striae, acne scars, hypertrophic scars and excised keloid scar beds. The NO serum was applied twice daily for 12 weeks. Photos were taken at 4- week intervals. Linear analog scales were administered to both patients and physicians to examine scar quality improvement. Several Wound Healing scenarios were examined. Surgical incision sites were pre-treated and treated after completion. Healing surgical local and regional flaps were treated. Non-healing diabetic ulcers, burn wounds, and smoking-induced vascular-compromised wounds were examined. NO serum was applied 4 times daily. Photographs were taken daily for the surgical patients and weekly for 4 weeks for the remainder of the population to examine any benefit.
Results
There were no hypersensitivity, allergic, or irritant reactions reported by any of the test subjects.
The Aging Skin population results were consistently favorable and increasingly positive with greater duration of use. Sixty percent of subjects noticed a decrease in visible wrinkles at 4 weeks, 68% by 8 weeks, and 84% by 12 weeks. Decreased pore size was reported by 45% of patients at 4 weeks, 55% of patients at 8 weeks, and 68% of patients at 12 weeks. An increase in skin tone was perceived by 72% of patients at 4 weeks, 80% by 8 weeks, and 83 % by 12 weeks. Textural improvement was reported by 68% of patients at 4 weeks, 83% at 8 weeks, and 88% at 12 weeks. Unwanted pigment variation was improved in 55% of patients at 4 weeks, 65% by 8 weeks, and by 78% of patients at 12 weeks. A decrease in skin oiliness was perceived by 72% of subjects at 4 weeks, 80% by 8 weeks, and 85% by 12 weeks. Unwanted vasculature such as telangiectasia or rosacea-related erythema was improved in 20% of patients at 4 weeks, 38% by 8 weeks, and 53% by 12 weeks.
RESULTS - Aging Skin
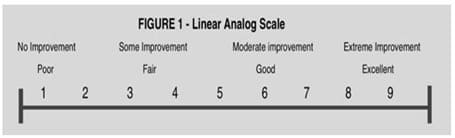
Linear analog scales were administered to reflect the patients’ perception of skin quality, and that of the treating physician.
RESULTS - Aging Skin
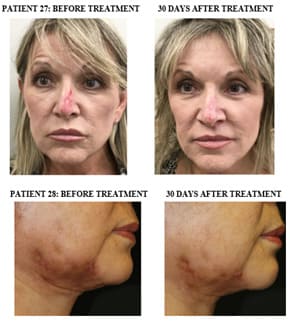
Improvement in tone and texture of skin afer 30 days of using NO serum twice daily.
RESULTS - Aging Skin
Improvement in tone, texture, and quality of skin after 30 days using NO Serum twice daily.
RESULTS - Aging Skin
Improvement in fine lines and wrinkles after 60 days using NO Serum twice daily.
RESULTS - Aging Skin
Improvement in tone and clarity of skin after 30 days using NO Serum twice daily.
RESULTS - Aging Skin
Improvement in tone and clarity of skin after 30-60 days of using NO Serum twice daily.
RESULTS - Aging Skin
Improvement in tone and clarity of skin after 30-90 days of using NO Serum twice daily.
RESULTS - Aging Skin
Improvement in skin quality and clarity in rocacea and exzema after 30-60 days using NO Serum twice daily.
RESULTS – Aging Skin
Reduction of fine line and pore size 30-90 days after using NO Serum twice daily.
RESULTS - Acne
Linear analog scales were administered to reflect the patients’ perception of skin quality, and that of the treating physician. Photographs were taken to document results.
RESULTS - Acne
Reducton in pustules and comedones 30-90 days after using NO Serum twice daily.
RESULTS - Acne
Reduction of pustules 30 days after using NO Serum twice daily.
RESULTS - Acne
Reduction of pustules, comedones, and nodles 30-90 days after lesing NO Serum twice daily.
RESULTS - Acne
Reduction of pustules and comedones 30 days after using NO Serum twice daily.
RESULTS -Acne
Improvement of cyctic acne 60 days after using NO Serum three times daily.
RESULTS - Acne
Reduction of pustules comedones, and cyctic lesions 30-90 days after using NO Serum three times daily.
RESULTS – Scar Therapy
Linear analog scales were administered to reflect the patients’ perception of skin quality, and that of the treating physician. Photographs were taken to document results.
RESULTS – Scar Therapy
Improvement in tone, quality of skin and reduction of acne scars 90 days after using NO Serum three times daily.
RESULTS - Wound Healing
Linear analog scales were administered to reflect the patients’ perception of skin quality, and that of the treating physician. Photographs were taken to document results.
RESULTS - Wound Healing
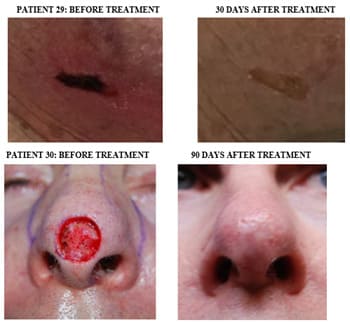
Re-epithelialization of previously non-healing wounds 30-days after using NO Serum twice daily.
RESULTS – Wound Healing
Re-epithelialization of vascular compromised diabetic ulcers occured and improved healing of full thickness skin grafts 30-90 days after using NO Serum.
The Active Acne population showed very promising results for utilizing nitric oxide topically. Seventy-five per cent reported a decrease in pustules and nodules by 4 weeks, 83% reported improvement by 8 weeks, and 85% by 12 weeks.
The Wound Healing population without exception showed excellent results. Rhytidectomy, blepharoplasty, and rhinoplasty patients displayed less bruising, edema, and faster re-epithelialization on the treated side when compared to the contralateral untreated control side. Previously non-healing diabetic ulcers and pressure ulcers healed within 30-45 days. Compromised local and regional flaps showed improved vascularization and viability within 30 days.
The Scar Therapy population showed positive trends, worthy of further investigation. Atrophic scars and striae, particularly abdominal and breast showed the most improvement with 37% describing less visibility of striae at 4 weeks, 49% at 8 weeks, and 72% by 12 weeks. Softening of hypertrophic scars was noted at 4 weeks, with some scar volume reduction noted by 12 weeks. Improved vascularity in these latter scars is postulated.
Discussion
The fields of Cellular Medicine, Regenerative and Stem Cell Therapy are growing rapidly [17]. Much has been written on the multiple health benefits of Nitric Oxide [16]. This multifunctional signaling molecule may prove to be the cornerstone of the stem cell regenerative medicine world [17]. NO is recognized as the requisite signal for stem cell mobilization and differentiation into target cell types. Endogenous production is a highly complex, twopronged, regulated process that is significantly reduced by 40 years of age [14]. This makes studies examining exogenous modes of administration intriguing. An oral replacement lozenge is available which has shown tremendous benefit [14,15,16].
Much has been written on the challenges of formulating a topically applied product which generates sufficient NO to absorb into the dermis, does not decay too rapidly, or produce adverse physiological byproducts [29-32]. There have been many studies demonstrating the metabolic effects of NO on the major components of skin and tissue including: fibroblasts, melanocytes, endothelial cells, keratinocytes, macrophages, neutrophils, and adipocytes [20-26].
To our knowledge, this is the first Pilot Study examining a novel, dual chamber, Nitric oxide generating serum for aging skin, acne, wound healing and scar therapy. Our findings indicate that the topical application of nitric oxide, when optimized, has a positive effect on improving vascularity to skin, as well as, the general tone, quality and texture of skin. This fact explains the observed reduction in fine lines, wrinkles, and pore size that was shown. Improvement in unwanted hyper-pigmentation and erythema was also observed.
Skin care can be likened to working out at a gym. If one goes regularly, the results will be better than if one goes sporadically. If one uses all of the equipment at the gym, the results will be better than if one only uses the biceps machine. A NO generating, topically applied serum is akin to hiring a “tissue personal trainer”. The fact that the majority of skin cells emit NO and are therefore depleted over time suggests their function is compromised over time, hence “aging skin”. The replenishment of NO, via this serum, reinvigorates the cells, allowing for improved function, postulating the positive aesthetic results shown in this study.
Topically applied Nitric oxide generating serum showed a positive effect in the acne population. The anti-inflammatory and ant-bacterial benefits of NO have been described [32,33]. As it relates to inflammatory conditions, acne vulgaris and subsequent sequalae, lead in conditions having a negative impact on a patients’ self- esteem. Acne vulgaris is a chronic inflammatory disease that affects 40-50 million Americans per year, and hundreds of millions of patients worldwide per year. Acne patients present an excellent model for studying scar pathophysiology. The complex interactions of infection, inflammation, tissue injury, wound healing and the propensity for scar formation allow scientists a unique opportunity to investigate alternate forms of therapy.
Acne is characterized by comedones, pustules, and papules. Left untreated, saucerized and pitted scars can form. The pathogenesis of acne is multifactorial. Four primary factors play a pivotal role in the formation of acne lesions: excess sebum production, abnormal keritanization, inflammation, and bacterial colonization of Propionibacterium acnes in the pilosebaceous unit. While a general concensus exists on the pathogenetic factors, the developmental sequence of events has been controversial. A traditional belief was that abnormal keritanization results in the microcomedone, the earliest subclinical acne lesion. Sebaceous gland activation by androgens, led to excess sebum production, with a keratin plug being formed. P acnes colonization induced the innate immune system, culminating in the visible inflammation [17].
It is now felt that subclinical inflammation precedes microcomedone formation. Immunohistochemical studies show significant inflammation around normal follicles of uninvolved skin of acne patients PRIOR to follicular hyperkeritanization. Another study showed inflammatory cell infiltrates without clinically visible inflammatory lesions. This is thought to be via the proinflammatory cytokine IL1alpha, independent of colonization [17]. Given this theory, it is understandable why topical NO has a beneficial effect on acne.
The Wound Healing and Scar therapy patient populations also showed positive trends worthy of further study. Examining the concept of 'scarless' wound healing, as in the Axolotl Salamander model, one sees a rapid re-epithelialization, and short inflammatory phase with TGFB3 playing a major role [38]. The modulatory effect that NO has on skin stem cells and communicating messengers such as exosomes can suggest why a topically applied NO serum would accelerate wound healing and play a vital role in multi-modality scar therapy.
Interestingly, as seen in Table 2, no patients were unhappy with NO serum. The majority were satisfied to extremely satisfied. This also had a spillover effect on the question of self-esteem with 55% of study subjects reporting an increase in self-esteem due to their appearance at 4 weeks, 78% at 8 weeks, and 85% at 12 weeks!
Conclusion
It is possible to deliver clinically relevant bioactive nitric oxide via a dual chamber NO generating delivery device. This Pilot Study shows valid proof of concept to warrant further studies in the areas of aging skin, acne, wound healing and scar therapy.

















|
|
Percentage |
||
|
Measured
Feature |
4 Wks |
8 Wks |
12 Wks |
|
Decreased
Wrinkles |
60% |
68% |
84% |
|
Decreased
Pore Size |
45% |
58% |
68% |
|
Increased
Skin Tone |
72% |
80% |
83% |
|
Improved
Skin Texture |
68% |
83% |
88% |
|
Decreased
Pigmentation |
55% |
65% |
78% |
|
Decreased
Oiliness |
72% |
80% |
85% |
|
Decreased
Erythema |
20% |
38% |
53% |
|
Decreased
Acne |
75% |
83% |
85% |
|
Decreased
Striae |
37% |
49% |
72% |
|
|
Percentage |
||
|
Satisfaction |
4 Wks |
8 Wks |
12 Wks |
|
Unhappy |
0 |
0 |
0 |
|
Satisfied |
75 |
20 |
10 |
|
Very
Satisfied |
19 |
72 |
6 |
|
Extremely
Happy |
6 |
8 |
84 |
References
- RF Furchgott, PM Vanhoutte (1989) Endothelium-derived relaxing and contracting factors. Faseb J 3: 2007-2018.
- MW Radomski, RM Palmer, S Moncada (1987) Endogenous nitric oxide inhibitshuman platelet adhesion to vascular endothelium. Lancet 2: 1057-1058.
- S Moncada (2000) Nitric oxide and cell respiration: physiology and pathology. Verh K Acad Geneeskd Belg 62: 171-179.
- R Weller (2003) Nitric oxide: a key mediator in cutaneous physiology. Clin Exp Dermatol 28: 511-514.
- MM Cals-Grierson, AD Ormerod (2004) Nitric oxide function in the skin. NitricOxide 10: 179-193.
- S Frank, H Kampfer, C Wetzler, J Pfeilschifter (2002) Nitric oxide drives skin repair:novel functions of an established mediator. Kidney Int 61: 882–888.
- R Weller, RJ Price, AD Ormerod, N Benjamin, C Leifert (2001) Antimicrobial effect of acidified nitrite on dermatophyte fungi, Candida and bacterial skin pathogens. J Appl Microbiol 90: 648-652.
- M Rizk, MB Witte, A Barbul (2004) Nitric oxide and wound healing. World Journal of Surgery 28: 301-306.
- FY Liew, FE Cox (1991) Nonspecic defence mechanism: the role of nitric oxide. Immunol Today 12: A17-A21.
- S Frank, H Kampfer, C Wetzler, J Pfeilschifter (2002) Nitric oxide drives skin repair: novel functions of an established mediator. Kidney Int 61: 882-888.
- FC Fang (1999) Nitric oxide and infection. Kluwer Academic/Plenum Publishers 1999.
- G Deliconstantinos, V Villiotou, C Fassitsas (1992) Ultraviolet-irradiated human endothelial cells elaborate nitric oxide that may evoke vasodila- tory response. J Cardiovasc Pharmacol 20: S63-S65.
- S Frank, B Stallmeyer, H Kampfer, N Kolb, J Pfeilschifter (1999) Nitric oxide triggers enhanced induction of vascular endothelial growth fac- tor expression in cultured keratinocytes (HaCaT) and during cutane- ous wound repair. FASEB J 13: 2002-2014.
- Bryan NS, Bian K, Murad F (2009) Discovery of the nitric oxide signaling pathway and targets for drug devel- opment. Front Biosci 14: 1–18.
- Bryan NS, Tribble G, Angelov N (2017) Oral microbiome and nitric oxide: the missing link in the manage- ment of blood pressure. Curr Hypertens Rep 19: 33.
- Bryan NS, Bill Gottlieb B, Zand J (2011) The Nitric Oxide Solution. Neogenis Labs 11: 1.
- Chernoff WG, Bryan NS, Andrea M Park (2018) Mesothelial Stem Cells and Stromal Vascular Fraction Use in Functional Disorders, Wound Healing, Fat Transfer, and Other Conditions. Facial Plastic Surgery Clinic N Am 26: 487-501.
- MM Cals-Grierson, AD Ormerod (2004) Nitric oxide function in the skin. Nitric Oxide 10: 179-193.
- RG Knowles, S Moncada (1994) Nitric oxide synthases in mammals. Biochem J 298: 249-258.
- C Nathan (1992) Nitric oxide as a secretory product of mammalian cells. FASEB 6: 3051-3064.
- A Papapetropoulos, G Garcia-Cardena, JA Madri, WC Sessa (1997) Nitric oxide production contributes to the angiogenic properties of vascular endothelial growth factor in human endothelial cells. J Clin Invest 100: 3131-3139.
- J MacMicking, QW Xie, C Nathan (1997) Nitric oxide and macrophage function. Annu Rev Immunol 15: 323-350.
- Y Yui, R Hattori, K Kosuga, H Eizawa, K Hiki, et al. (1991) Calmodulin-independent nitric oxide synthase from rat polymorphonuclear neutrophils. J Biol Chem 266: 3369-3371.
- DE Heck, DL Laskin, CR Gardner, JD Laskin (1992) Epidermal growth factor suppresses nitric oxide and hydrogen peroxide production by keratinocytes. Potential role for nitric oxide in the regulation of wound healing. J Biol Chem 267: 21277-21280.
- K Ivanova, IC Le Poole, R Gerzer, W Westerhof, PK Das (1997) Effect of nitric oxide on the adhesion of human melanocytes to extracellular matrix components, J Pathol 183: 469-476.
- M Jackson, F Frame, R Weller, RC McKenzie (1998) Expression of nitric oxide synthase III (eNOS) mRNA by human skin cells: melanocytes but not keratinocytes express eNOS mRNA. Arch Dermatol Res 290: 350-352.
- Esper RJ, Nordaby RA, Vilarin ̃oJO, Antonio Paragano, José L Cacharrón, et al. (2006) Endothelial dysfunction: a comprehensive appraisal. Cardiovasc Diabetol 5: 4.
- Zand J, Lanza F, Garg HK, Nathan S Bryan (2011) All-natural nitrite and nitrate containing dietary supplement promotes nitric oxide production and reduces triglycerides in humans. Nutr Res 31: 262-269.
- JR Lancaster Jr (1994) Simulation of the diffusion and reaction of endogenouslyproduced nitric oxide. Proc Natl Acad Sci 91: 8137-8141.
- CV Suschek, T Schewe, H Sies, KD Kroncke (2006) Nitrite, a naturally occurringprecursor of nitric oxide that acts like a ‘prodrug’. Biol Chem 387: 499-506.
- Opländer C, CM Volkmar, A Paunel-Görgülü, EE van Faassen, C Heiss, et al. (2009) Whole body UVAirradiation lowers systemic blood pressure by release of nitric oxide fromintracutaneous photolabile nitric oxide derivates. Circ Res 105: 1031-1040.
- R Weller, RJ Price, AD Ormerod, N Benjamin, C Leifert (2001) Antimicrobial effectof acidified nitrite on dermatophyte fungi Candida and bacterial skinpathogens. J Appl Microbiol 90: 648-652.
- P Lopez-Jaramillo, MY Rincon, RG Garcia, SY Silva, E Smith, et al. (2010) A controlled, randomized-blinded clinical trial to assess the efficacy of a nitric oxidereleasing patch in the treatment of cutaneous leishmaniasis by Leishmaniapanamensis (V.). Am J Trop Med Hyg 83: 97-101.
- SY Silva, LC Rueda, GA Marquez, M Lopez, DJ Smith, et al. (2007) Double blind, randomized, placebo controlledclinical trial for the treatment of diabetic foot ulcers, using a nitric oxidereleasing patch: Pathon. Trials 8: 26.
- AT Tucker, RM Pearson, ED Cooke, N Benjamin (1999) Effect of nitric-oxide-generating system on microcirculatory blood flow in skin of patients withsevere Raynaud’s syndrome: a randomised trial. Lancet 354: 1670-1675.
- ME Anderson, TL Moore, S Hollis, MI Jayson, TA King, AL Herrick (2002) Digital vascular response to topical glyceryl trinitrate, as measured by laser Dopplerimaging, in primary Raynaud’s phenomenon and systemic sclerosis. Rheumatol (Oxford) 41: 324-328.
- C Oplander, A Romer, A Paunel-Gorgulu, T Fritsch, EE van Faassen, et al. (2012) Dermalapplication of nitric oxide in vivo: kinetics biological responses andtherapeutic potential in humans. Clin Pharmacol Ther 91: 1074-1082.
- Seifert, James R Monaghan, S Randal Voss, Malcolm Maden (2012) Skin regeneration in adult axolotls: a blueprint for scar-free healing in vertebrates. PloS one 7: e32875.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.