The Use of Endo‑SPONGE® in Anastomotic Leaks after TME for Middle‑Low Rectal Cancer without Ileostomy
by Lo Bianco S1*, Petruzzellis C2, Catarella D2, Capuzzo G3, Basile G3, Bordonaro R4, Piazza L1, Leonardi A1
1Department of Oncological Surgery, ARNAS Garibaldi, Catania, Italy
2Department of Gastroenterology, ARNAS Garibaldi,Catania, Italy
3Department of General Surgery and Medical Surgical Specialties, G. Rodolico, Catania, Italy
4Department of Medical Oncology, ARNAS Garibaldi, Catania, Italy
*Corresponding author: Lo Bianco S, Department of Oncological Surgery, ARNAS Garibaldi, Catania, Italy
Received Date: 18 November 2024
Accepted Date: 22 November 2024
Published Date: 25 November 2024
Citation: Lo Bianco S, Petruzzellis C, Catarella D, Capuzzo G, Basile G, et al. (2024) The Use of Endo-SPONGE® in Anastomotic Leaks after TME for Middle-Low Rectal Cancer without Ileostomy. J Surg 9: 11187 https://doi.org/10.29011/2575-9760.011187
Abstract
Anastomotic leaks are a frequent complication in patients undergoing low rectal resection and TME for rectal cancer. There have been many methods of the treatment of rectal anastomotic leaks, including: medical management, ileostomy, endosponge, endovac. A men 49 years old, had a rectal cancer approximately 8-10 cm from the anal margin. The patient underwent robotic anterior rectal resection with TME (Total mesorectal excision). No protective ileostomy was performed. On the second postoperative day was noted a leakage of enteric fluid from the drainage was noted, it was decided for conservative treatment with Endosponge application.
Keyword: Anastomotic leak, rectal cancer, endosponge, ileostomy, tme
Introduction
Anastomotic leaks are a frequent complication in patients undergoing low rectal resection and TME for rectal cancer. The reported anastomotic leak rates is 3-19% [1]. Anastomotic leaks have some can have consequences for patients [2]. The choice of the treatment of leaks can also affect the general and oncological outcomes [3]. There have been many methods of the treatment of rectal anastomotic leaks, including: medical management, ileostomy, endosponge, endovac. The most feared complication is peritonitis. Patients with general peritonitis require a laparotomy, washing, draining and resection of the anastomosis with ileostomy o colostomy [4]. The procedure is a major physiological insult for the patients. The use of an endoluminal vacuum system as a treatment option for rectal anastomotic leaks has been suggested as a minimally invasive method of treatment with a higher success rate.
Case Report
A men 49 yeras old, performs colonoscopy for rectal bleeding which documents a formation approximately 8-10 cm from the anal margin. The patient undergoes biopsies, which demonstrate the presence of rectal adenocarcinoma. A staging computed tomography and magnetic resonance imaging are performed, demonstrating the presence of a T2 N+ intraperitoneal tumor. The patient underwent robotic anterior rectal resection with TME (Total Mesorectal Excision), after discussion at the gastroenterological GOM. No protective ileostomy was performed and a perianastomotic abdominal drain was placed. After the surgery the patient had early canalization. On the second postoperative day was noted a leakage of enteric fluid from the drainage was noted. After gastroenterological consultation, it was decided for conservative treatment with Endosponge application. The patient underwent 10 treatments, each every 4 days.
During the hospitalization the patient was monitored and the reduction of the anastomotic fistula flow was noted, until complete closure. At the end of the treatment the patient was subjected to abdominal CT scan, which demonstrated clinical improvement.
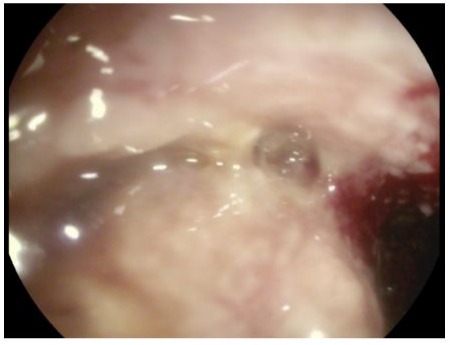
Figure 1: Anastomotic dehiscence after treatment.
Discussion
In the literature, the rate of anastomotic leakage in rectal anastomoses has been reported to be 7-11% [5,6]. The use of endosponge medical therapy in the treatment of these patients has shown that the rate of resolution was 11.8%. Most of the studies are small number case series or single case report with many bias. In these manuscripts it has been demonstrated that patients who started the treatment early (within 6 weeks from onset) have significantly higher rate of success. In the case of chronic leak and late therapy start, the cavity is less susceptible to vacuum therapy. Furthermore, the use of radiotherapy prior to surgery not only increases the risk of anastomotic leak but also influences the success rate of Endosponge therapy [7,8]. In literature, it is described to perform ileostomy with endosponge therapy [9,10]. In our work, we treated the fistula without making ileostomy.
Conclusion
In selected patients with anastomotic leakage after middle-low rectal resection, Endosponge appears to be a good solution, even without making an ileostomy. EndoSPONGE® works best when therapy is started early and in patients without preoperative radiotherapy. Treatment with Endosponge without making an ileostomy, requires further evaluation with more cases.
References
- Rullier E, Laurent C, Garrelon JL, Michel P, Saric J, et al. (1998) Risk factors for anastomotic leakage after resection of rectal cancer. Br J Surg 85: 355-358.
- Chadi SA, Fingerhut A, Berho M, DeMeester SR, Fleshman JW, et al. (2016) Emerging trends in the etiology, prevention, and treatment of gastrointestinal anastomotic leakage. J Gastrointest Surg 20: 20352051.
- Chambers WM, Mortensen NJMC (2004) Postoperative leakage and abscess formation after colorectal surgery. Best Pract Res Clin Gastroenterol 18: 865-880.
- Phitayakorn R, Delaney CP, Reynolds HL, Champagne BJ, Heriot AG, et al. (2008) Standardized algorithms for management of anastomotic leaks and related abdominal and pelvic abscesses after colorectal surgery. World J Surg 32: 1147-1156.
- Karanjia ND, Corder AP, Bearn P, Heald RJ (1994) Leakage from stapled low anastomosis after total mesorectal excision for carcinoma of the rectum. Br J Surg 81: 1224-1226.
- Vignali A, Fazio VW, Lavery IC, Milsom JW, Church JM, et al. (1997) Factors associated with the occurrence of leaks in stapled rectal anastomoses: a review of 1,014 patients. J Am Coll Surg 185: 105113.
- Matthiessen P, Hallböök O, Andersson M, Rutegård J, Sjödahl R (2004) Risk factors for anastomotic leakage after anterior resection of the rectum. Colorectal Dis 6: 462-469.
- Barnett GC, West CML, Dunning AM, Elliott RM, Coles CE, et al. (2009) Normal tissue reactions to radiotherapy: Towards tailoring treatment dose by genotype. Nat Rev Cancer 9: 134.
- Verlaan T, Bartels SAL, van Berge Henegouwen MI, Tanis PJ, Fockens P, et al. (2011) Early, minimally invasive closure of anastomotic leaks: a new concept. Color Dis 13: 18-22.
- Glitsch A, von Bernstorf W, Seltrecht U, Partecke I, Paul H, et al. (2008) Endoscopic transanal vacuum-assisted rectal drainage (ETVARD): an optimized therapy for major leaks from extraperitoneal rectal anastomoses. Endoscopy 40: 192-199.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.