The Safety of A New Device as A Monopolar Electrosurgical Unit in Carotid Endarterectomy: A Single Center Case Series
by Ascoli Marchetti Andrea*, Ciattaglia Riccardo, Oddi Fabio Massimo, Fazzini Stefano, Martina Battistini, Ippoliti Arnaldo
Department of Biomedicine and Prevention, Vascular Surgery Unit, University of Rome Tor Vergata, Rome, Italy Viale Oxford 81 00133 Rome Italy
*Corresponding author: Andrea Ascoli Marchetti, Department of Biomedicine and Prevention, Vascular Surgery Unit, University of Rome Tor Vergata, Rome, Italy
Received Date: 21 November 2024
Accepted Date: 26 November 2024
Published Date: 28 November 2024
Citation: A Ascoli Marchetti, R Ciattaglia, FM Oddi, S Fazzini F, M Battistini. A. Ippoliti (2024) The Safety of A New Device as A Monopolar Electrosurgical Unit in Carotid Endarterectomy: A Single Center Case Series. J Surg 9: 11191 https://doi.org/10.29011/2575-9760.011191.
Abstract
Surgical preparation of the carotid vessels involves some ligature of the vessels and the repeated coagulation of tissues in a region with numerous nerve fibers adjacent to the carotid vessels. The surgeon must take great care to avoid causing lesions that may involve the vagus nerve, the hypoglossal nerve, the glossopharyngeal nerve, the spinal accessory nerve, which may be found during the preparation of the carotid vessels or be adjacent to the surgically explored regions. Small caliber vessels require ligatures and sections, as an alternative to the more rapid use of the electrosurgical unit, in order to avoid dispersion of the electric current which can cause very annoying complications for the patient in the post-operative period such as swallowing disorders and deficits in lifting the shoulder or dysphonia. The use of an electrocautery capable of performing the section without the electrical dispersion of the traditional handpiece was safely employed in two cases of carotid endarterectomy.
Keywords: Carotid surgery; Endarterectomy; Surgical exposure; Vessel ligation
Introduction
The purpose of the study was the evaluation of ERBE’s Biclump® as a new application in vascular surgery. The possibilities of the device developed for each type of surgery has allowed the improvement of the execution times of the single procedures and the reduction of the relative costs. In thyroid and liver surgery, good results have already been reported in the recent past, [1,2] but no data are reported in the literature regarding possible use in surgical approach in carotid vessel exposure. We therefore chose two standard approaches, in non-replicated packages, to test the initial validity of BiClamp and test its capabilities. This experience was conducted on two cases of carotid endarterectomy, in which we used the device during the anatomic multi-layered next dissection of a lateral cervicotomy within the preliminary surgical preparation for vascular exposure before carotid endarterectomy (Figure 1).
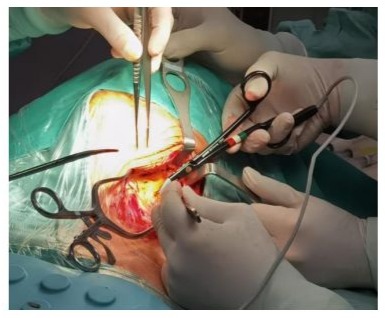
Figure 1: Introperative BiClamp® (ERBE) image during vessel cauterization.
Cases Report
At the University Hospital of Tor Vergata in Rome, in July 2022, two patients, a 78-year-old man and an 81-year-old woman, with comorbidities in line with the standard vascular patient: systemic arterial hypertension, both smokers and affected by chronic ischemic heart disease. The male patient also suffered from diabetes mellitus. Both patients had not undergone previous neck surgery or local radiotherapy. They have been classified with ASA class II/III. [3] (Table 1). Both patients were asymptomatic at the time of diagnosis of carotid stenosis, which occurred in the context of routine ultrasound color-Doppler instrumental evaluations. The lesions in both cases presented a hemodynamic stenosis with severe flow-meter turbulence. Both cases were performed under general anaesthesia. We performed a lateral cervicotomy, along the anterior margin of the sternocleidomastoid muscle, incising the skin of the neck, and deepening through the subcutis and the superficial cervical fascia until reaching the sheath of the vascularnerve bundle. After the skin incision, by crossing the underlying planes, it may be necessary to ligate or coagulate vessels with a diameter ranging from 2 to 10 mm in diameter (average RVD 5 mm), including the thyroid-lingual-facial venous trunk, as previous described by Griepp [4].
|
gender Male Famale |
||
|
Age |
78 years old |
81 years old |
|
comorbilities |
systemic arterial hypertension, smoker and affected by chronic ischemic heart disease, diabetes |
systemic arterial hypertension, smoker and affected by chronic ischemic heart disease |
|
Asa classification |
II/III |
II/III |
|
Clinical condition |
asymptomatic |
asymptomatic |
|
diagnosis |
Carotid stenosis |
Carotid stenosis |
|
hemodynamically significant |
hemodynamically significant |
|
|
Anesthesia |
general |
general |
|
In both procedures we noted a decrease in the time necessary (from about 30 ‘to 1215’) this means a reduction of 57% of the surgical time to the exposure of the common, internal and external carotid arteries. |
||
Table 1: Demographic and clinical findings of the patients.
Once the internal and external common carotid artery was exposed, a transmedial endarterectomy with angioplasty was performed in both cases by interposing a polyurethane patch sutured with Prolene 5/0. In our experience we have found in both procedures a decrease in the time necessary (from about 30 ‘to 12-15’, a reduction of 57% of the surgical time to the exposure of the common, internal and external carotid arteries [5,6]. The endarterectomy was uneventfully and, in both cases, and no hemorrhagic or nerve complications was noted. No ligature was performed during vessels preparation and postoperative surgical hemostasis before wound closure (Figure 2). The hospital stays was two days. The 48-month follow-up documented the absence of central and peripheral neurological lesions and the patency of the unobstructed internal carotid arteries
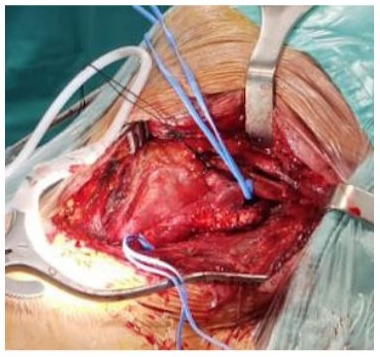
Figure 2: Intraoperative image: no ligature was done before and after surgical angioplasty.
Discussion
BiClamp® (ERBE, Tübingen, Germany) would be an innovative bipolar coagulation system with an adjustable current modulation and intelligent self-control. Such as it could transform electrical energy into heat, thus attaining an ideal energy-based vessel seal, with a minimum dissipation of the heat produced and electrical dispersion in terms of surface yield on the area involved. This evidence probably positively impacted the outcome of the procedure by significantly reducing the rate of inflammation and the imbibition of adjacent soft tissues (Figure 3). The use in thyroid, hepatic and gynecological surgery has already been successfully tested [1,2,7]. Vessels with a diameter ≤7 mm can be successfully sealed by BiClamp alone. ERBE’s BiClamp® is a reusable, cost-effective instrument. Such device has been widely used in other types of surgical procedures, such as thyroidectomies, hysterectomies, and breast surgery, with proven efficacy and safety. [7-9] The jaws of instrument allowed a dissection of the tissues like a common dissector, ensuring the simultaneous possibility of safely coagulating any sources of bleeding. The reference target for the mean caliber of the vessels we cauterized was about 5.2 mm (RVD 3.8 ± 1.4) (Reference Vascular Diameter). The alternative methods in larger caliber vessels is ligatures with Vycril 3/0 (Ethicon®) upstream of the cleavage or vascular clips (B.Braun Vascular Clips®). In both our cases no traditional ligature was used.

Figure 3: Elettrosurigical monitor unit: energy transmission has been set and there is not spread beyond the point of cauterization.
However, experience using the BiClamp® applied in vascular surgery is very limited. The possibility of dissecting cleavage planes, orienting the structures through the prongs of the clump, streamlines the surgical practice, especially if associated with the resolution by coagulation of any bleeding sources. The bipolar functioning of the electro-conduction allows to be used also in proximity of excitable structures such as nerve fibers of various sizes at the peripheral level, with the minimum impact from the pathophysiological point of view. We found no significant differences in the efficacy of cauterization between arterial and venous vessels. In addition, it was possible to evaluate the cross section after cutting the vascular structures underlining a complete collapse of the collagen structure of the vessel wall with a precise sclerotization in the absence of necrosis. A low dispersion is generally required in case of use of monopolar electrosurgery try limiting the scarring of the most important extracranial nerves, such as VII, X, XI and XII.
Although rare, the nerve injuries are often one of the most frequent causes of postoperative complications and result in an evident discomfort for the patient who in the most serious cases also reaches evident impairments in daily life [10,11]. Furthermore, the great ability to adjust the cut with a customizable electroconductance in relation to the type of lysed tissue, to the structural components, such as density, thickness, quantity of fluids and the relationships between the planes, considerably increases the speed of preparation of the field and exposure of the target structures, minimizes the extent of complications and subsequent comorbidities in the post-operative period, as a adjuvant modality to decrease hospitalization times and helping to improve the outcome of the procedure.
The technique affords quicker operative times, less blood loss, minimal intraoperative morbidity, and acceptable surgical outcomes. The reduced post-operative pain or peripheral neurological events such as paresthesia observed, confers more rapid mobilization and improved recovery, especially in patients with pacemakers. In our experience, we did not find any complications in the immediate postoperative period and after the six months follow up in both patients.
Conclusion
Overall, ERBE’s BiClamp® would be a safe, effective alternative to conventional suture ligation in carotid surgical approach, with a good outcome, comparable or even better, for this kind of procedure, than that obtained with standard and widely used surgical instrumentation. Our experience, albeit on a limited sample of cases and extended to a single type of surgical approach, seems to suggest the possibility of expanding this method also at the level of vascular surgery procedures. The results obtained need to be confirmed on much larger case series, with samples stratified over time also in the number of procedures. The increase in the rate of experience in other confident surgical branches will open the space for increasingly widespread and standardized approaches with this method, which is also simple to use, may be also to applies to other kind of surgery.
References
- Del Rio P, Lazzari G, Rossini M, Nisi P, Perrone G, et al. (2015) The use of energy devices for thyroid surgical procedures. Harmonic Focus versus Biclamp 150. Ann Ital Chir 86: 553-559.
- Zhao YJ, Zhou DC, Liu FB, Zhao HC, Wang GB, et al. (2017) BiClamp® vessel-sealing device for open hepatic resection of malignant and benign liver tumours: a single-institution experience. BMC Cancer 17: 554.
- Doyle DJ, Hendrix JM, Garmon EH (2024)American Society of Anesthesiologists Classification 2024.
- Griepp DW, Sajan A, Diraimo R, Starikov L, Márquez S (2021) Quantitative Prediction of the Location of Carotid Bifurcation and Neurovascular Structures in the Carotid Region: A Cross-Sectional Cadaveric Study 2021.
- Taboada CR, Duran Mariño JL, Garcia Colodro JM, Pena Holguin J, Martinez Gallego EL (2016) Clinical Outcomes after Carotid Endarterectomy in Patients with Contralateral Carotid Occlusion. Ann Vasc Surg 32: 83-87.
- Azhar B, Wafi A, Budge J, Loftus I (2020) Timing of carotid endarterectomy and clinical outcomes. Ann Transl Med 8: 1267.
- Blayney GV, Beirne JP, Hinds L, Quinn D, Dorman GJ (2017) Vaginal Hysterectomy using the ERBE BiClamp® Bipolar Vessel Sealing System: A Case Series. Ulster Med J 86: 2017.
- Li L, Qie MR, Wang XL, Huang J, Zhang Q, et al. (2012) BiClamp(®) forceps was significantly superior to conventional suture ligation in radical abdominal hysterectomy: a retrospective cohort study in 391 cases. Arch Gynecol Obstet 286: 457-463.
- Takeuchi H, Saeki T, Shigekawa T, Sano H, Nakamiya N, et al. (2010) BiClamp Forceps Signifi cantly Shorten the Operation Time for Breast Surgery. Surg Today 40: 706-710.
- Maertens V, Maertens H, Kint M, Coucke C, Blomme Y (2016) Complication Rate after Carotid Endarterectomy Comparing Patch Angioplasty and Primary Closure. Ann Vasc Surg 30: 248-252.
- Kakisis JD, Antonopoulos CN, Mantas G, Moulakakis KG, Sfyroeras G, et al. (2017) Cranial Nerve Injury After Carotid Endarterectomy: Incidence, Risk Factors, and Time Trends. Eur J Vasc Endovasc Surg 53: 320-335.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.