The Rare Case of Bowel Obstruction Due to Meckel Diverticulum in A 55-Year-Old Patient
by Catarina Alicia Bracamonte1*, Anna-Maria Sauer Durand2
1Assistant Physician, KSA Cantonal Hospital Aarau, Kantonsspital Aarau, 5000 Aarau Switzerland
2Senior Physician, Department of General and Vascular Surgery, KABEG Landeskrankenhaus Villach, Austria
*Corresponding author: Catarina Alicia Bracamonte, Assistant Physician, KSA Cantonal Hospital Aarau, Kantonsspital Aarau, 5000 Aarau Switzerland
Received Date: 18 March 2026
Accepted Date: 24 March 2026
Published Date: 26 March 2026
Citation: Bracamonte CA, Sauer Durand AM (2026) The Rare Case of Bowel Obstruction Due to Meckel Diverticulum in A 55-YearOld Patient. Ann Case Report. 11: 2574. DOI: https://doi.org/10.29011/2574-7754.102574
Abstract
The Meckel diverticulum is the most common congenital gastrointestinal anomaly with an estimated prevalenc of 0.3-4%. However, the majority of the Meckel diverticulum are asymptomatic and are only discovered incidentally during abdominal surgery for another reason or during autopsies. Symptomatic diverticula appear mostly in children. In this case report we present the rare case of a 55-year old patient with intestinal obstruction due to a symptomatic Meckel diverticulum, which was discovered during surgery.
Keywords: Meckel’s diverticulum, bowel obstruction, abdominal pain, diverticulectomy
Introduction
Meckel’s Diverticulum is the most common congenital gastrointestinal anomaly. [1-8] It was first described in 1598 by Wilhelm Fabricius Hildanus, a German surgeon. However, the diverticulum is named after Johann Friedrich Meckel, a German anatomist who first described the embryological origin and pathological features of the Meckel diverticulum in 1809. [1-3] Meckel diverticulum is a true diverticulum resulting from the incomplete obliteration of the vitelline duct between the 5th and 7th week of gestation. [3,5,8] The diverticulum is on average located 53 cm orally of the ileocecal valve (range 7-200cm) with a diameter of 15.8 cm (range 0.3-7cm) and a length of 3.05 cm (range 0.4-11cm) [1,8].
The estimated prevalence of the Meckel diverticulum varies between 0.3-4% [1,4,5,8,] with most autopsy studies describing a prevalence of 1.2%. [4,5] Most of the Meckel diverticula are asymptomatic and found incidentally during an abdominal surgery for a different reason [2-8].
The estimated life-time risk of a symptomatic Meckel diverticulum is 4 %1 with an estimated current mortality rate related to Meckel’s diverticulum of 0.0016% [4,5].
Symptomatic Meckel’s diverticulum is more common in male patients compared to female patients with a rate of 1.5-4 :1 and most common in pediatric patients [7].
The most common complications due to Meckel’s diverticulum are bleeding, inflammation with or without perforation and mechanical obstruction of the bowel due to intussusception, volvulus, entrapment of the diverticulum within an inguinal hernia (Littre’s hernia), entrapment of a bowel loop beneath the mesodiverticular band or by a band stretching between the Meckel’s diverticulum and the base of the mesentery, bezoar and tumors [1,2,8].
Case Presentation
A 55-year-old man presented himself in the emergency department with abdominal pain (VAS 10/10) which appeared suddenly and lasted for a couple of hours. There was no nausea or vomiting. The patient has been hospitalized because of a small bowel obstruction four years earlier which was treated conservatively. In prior patient history there were two incidents where the patient presented himself in the emergency department because of abdominal pain. Once it was interpreted as obstipation the other time as gastritis. There was no history of previous abdominal operations. In the physical examination the abdomen was soft with slightly decreased bowel sounds in the right hemiabdomen and tenderness in the right lower quadrant. Vital signs were normal. Laboratory results showed a white blood cell count of 10.4 G/l and a slighty elevated lactate of 3.6 mmol/l with otherwise normal results. Because of the sudden onset of the pain and the elevated lactate a CT-scan was performed to check for mesenteric ischemia. The scan showed a closedloop obstruction of the small bowel with reduced perfusion and adjoining fluid (Figure 1).
We decided to perform an exploratory laparoscopy. We found a distended small intestine loop, slightly venously congested, which appeared to pass under another small intestine loop. A full revision of the small intestine was not possible as the incarcerated loop could not be pulled out from under the other small intestine loop. After converting to a laparotomy, the reason for the mechanical obstruction could be identified as a Meckel diverticulum where the tip of the diverticulum adhered to the peritoneum in the right lower quadrant and built an arch under which the small intestine loop incarcerated itself. We dissected the Meckel diverticulum from the peritoneum and performed a diverticulectomy by wedge resection. The incarcerated small intestine loop was still vital and didn’t need to be resected. (Figure 2) The Meckel diverticulum was about 7 cm long and was located about 80 cm orally of the ileocecal valve (Figure 3).
The postoperative period was without complication with an unproblematic oral food intake up to a normal diet. The patient was discharged 5 days after the operation.
Histologically there was no ectopic tissue or malignancy found in the diverticulum.
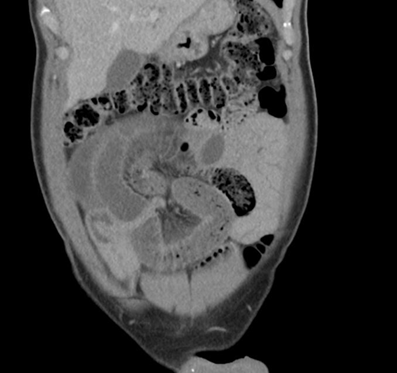
Figure 1: CT-scan that showed a closed-loop obstruction of the small intestines.
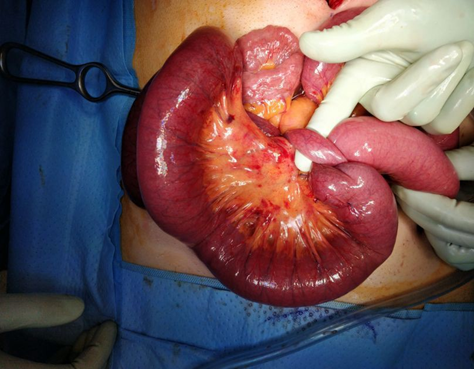
Figure 2: Incarcerated small bowel loop under the Meckel diverticulum.
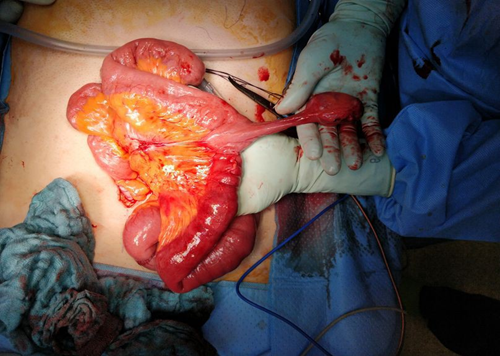
Figure 3: Meckel diverticulum.
Conclusion
Meckel’s diverticulum (MD) is the most common congenital anatomical gastrointestinal anomaly with a prevalence of about 0.3-4% in the population and about 1-2% post mortem in autopsy studies. [2,5,8] 70-80% of the diverticula are silent and symptomatic diverticulum is most common in children (4% in children under four years). Symptoms include mechanical obstruction, lower GIbleeding, non-specific abdominal pain and inflammation. The risk of a complicated MD decreases with age (about 1% for patients in their forties and practically absent for patients in their seventies). [8] The life-time risk for a complication by a MD is 4-6% with 2550% of those being children under ten years old [2,5].
Symptoms in adults range from bleeding (8-63%) mostly caused by ectopic gastric mucosa and the formation of an ulcer to mechanical obstruction (14-40%) like intussusception, volvulus obstruction or hernial incarceration to inflammation (30-58%). Rare complications are perforation or neoplasm [8].
The incidence of a symptomatic MD is difficult to detect because of a lack of a simple screening technique for MD in the general population. It is only possible via population estimates. [5] Risk factors for a complicated MD are age under 45-50 years, male, diverticulum length over 2cm and the presence of abnormal tissue. [2,5,7] If one of these criteria apply there’s a 17% risk of a symptomatic MD, if all four criteria apply the risk of a complicated MD is 70%. [1,5] Additional risk factors include broad-based diverticulum and fibrous bands attached to the diverticulum [7].
Most MDs get diagnosed incidentally during an abdominal operation for a different reason. [8] Only 5.7% of the MD (symptomatic or asymptomatic) are diagnosed before surgery [1].
The diagnosis of an asymptomatic MD through songraphy or CT-scan is very difficult. An actively bleeding diverticulum can be diagnosed by an angiography with an accuracy rate of about 59%. A mesenteric arteriography CT-scan has a specificity of 92% with a sensitivity of 85% in an active bleeding. Other possible diagnostics for an MD are technetium-99 pertechnetate scanning which has an affinity for gastric mucosa with a specificity of 95% and a sensitivity of 80-90% in children and a specificity of 9% and a sensitivity of 62.5% in adults. If there is active bleeding, there’s a risk of false negative results due to a dilution of the radiotracer and lower delivery due to vasoconstriction in the MD.
Another possible diagnostic tool is capsule endoscopy and doubleballoon endoscopy with a detection rate of 68.1% of a bleeding diverticulum. An advantage of the double-balloon endoscopy is being a diagnostic and therapeutic tool of a bleeding MD at the same time.
Another possible detection method is a CT- or MR enterography which is more reliable for lesions in small intestines than a regular CT-scan. An advantage of the MR enterography is the lack of radiation [1,2,5].
The therapy of a complicated MD is resection, either by diverticulectomy or resection of an ileum segment depending on intraoperative findings. If the diverticulum has a broad base or is actively bleeding, a segment resection should be performed because the bleeding often originates from the adjacent ileum. If there is suspicion of malignancy a wider resection of the intestines should be performed [2,5].
There are no clear recommandations regarding resection of asymptomatic MDs. Postoperative complications after resection include SSI, mechanical obstruction due to adhesions and anastomotic leackage. A literature review by Zani et al. showed a significantly higher complication rate of 5.3% in patients where an asymptomatic MD was resected vs non resection with a complication rate of 1.3% [1,7,8].
The life-time risk of a hospitalisation due to a complicated MD is 4% and the life-time risk of an operation due to a complicated MD is 3%. [8] The number needed to resect to avoid one death due to MD overall is 800 depending on the patient’s age. Varying from 758 in pediatric patients, to 781 in 15-44-year-olds, 771 in 45-65-year-olds, 911 in 66-75-year-olds and even less in patients over 75 years old, where 1111 individuals needed surgery to evite one fatal case. [1,4] The estimated mortality rate related to MDresection is around 0.001% [5].
Conclusion
Even though a symptomatic Meckel diverticulum is rare, especially in adults it should be considered as a differential diagnosis that presents with a bowel obstruction without prior abdominal surgeries.
If an asymptomatic MD is found incidentally during a procedure, especially in old patients, resection can be reconsidered due to higher complication rates in resection versus omitting.
Acknowledgments: None.
Ethics and patient consent: Informed consent was obtained from the patient for the publication of this manuscript.
Conflict of Interest Statement: The authors report no conflict of interest in connection with this article.
References
- Hansen CC, Søreide K. (2018). Systematic review of epidemiology, presentation and management of Meckel’s diverticulum in the 21st century. Medicine (Baltimore). 97: e12154.
- Kuru S, Kismet K. (2018). Meckel’s diverticulum : clinical features, diagnosis and management. Rev Esp Enferm Dig. 110: 726-732.
- Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. (2005). Meckel’s Diverticulum, The Mayo Clinic Experience With 1476 Patients (1950-2002). Ann Surg. 241: 529-533.
- Zani A, Eaton S, Rees CM, Pierro A. (2008). Incidentally Detected Meckel Diverticulum : To resect or not to resect? Ann Surg. 247: 276281.
- David PJ, Pauli EM. (2025). Meckel’s diverticulum. UpToDate.
- Lindeman RJ, Søreide K. (2020). The Many Faces of Meckel’s Diverticulum : Update on Management in Incidental and symptomatic patients. Curr Gastroenterol Rep. 22: 3.
- Rahmat S, Sangle P, Sandhu O, Aftab Z, Khan S. (2020). Does an Incidental Meckel’s Diverticulum Warrant Resection? Cureus. 12: e10307.
- Zyluk A. (2019). Management of incidentally discovered unaffected Meckel’s diverticulum – a review. Pol Przegl Chir. 91: 41-46.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.