The Evolution of Chronic Primary Angle Closure Glaucoma in the Inuit and Oriental Eye
Paul Arthur Price1*, Melissa Lannon2
1Department of Ophthalmology Dalhousie University, Canada
2Residency in Neurosurgery, Memorial University, London Ontario, Canada
*Corresponding author: Paul Arthur Price, Department of Ophthalmology Dalhousie University, Canada
Received Date: 02 February, 2023
Accepted Date: 15 February, 2023
Published Date: 20 February, 2023
Citation: Price PA, Lannon M (2023) The Evolution of Chronic Primary Angle Closure Glaucoma in the Inuit and Oriental Eye. J Community Med Public Health 7: 290. DOI: https://doi.org/10.29011/2577-2228.100290
Abstract
Primary Angle Closure has a high incidence in both China and amongst Inuit. Genetic Study along with both linguistic medical anthropology and anatomical studies support this connection. An increase in resulting mental health issues is documented. A case study is presented showing the usefulness of Swept Source OCT with clear three-dimensional imaging is useful in diagnosis, treatment, and follow-up. Glaucoma is reported as the leading etiology of irreversible blindness, and is most commonly seen in Asian populations. One form of glaucoma in particular, primary angle closure glaucoma (PACG) is likely responsible for the high prevalence of glaucoma reported in China, given that over 80% of PACG cases are found in the region [1,2]. It is believed that the increased incidence of PACG in this population is secondary to plateau iris, which carries a higher prevalence among Asian populations [3]. PACG carries a higher rate of morbidity with irreversible blindness than Primary Open Angle Glaucoma (POAG), and therefore is a significant population health concern in the region.
Keywords: Primary angle closure glaucoma; Inuit; China; Anthropology; Swept source OCT; Argon laser iridoplasty
Introduction
Plateau iris is most often an anatomical variant found in Asian populations, particularly in Mongolia, an area with a particularly high prevalence of PACG. But this trait has followed the migration pattern of Asian populations, extending to Greenland, as well as North America. Analyses of mitochondrial DNA and the nonrecombining portion of the Y-chromosome have tracked these migration patterns from the evolution of Homo sapiens in Africa 200 000 years ago to present (Figure 1). These analyses revealed a northbound migration pattern from Asia into Siberia approximately 30 000 years ago. The Inuit populations inhabiting the northern region from Alaska to Greenland are considered descendants of a migrating population that crossed the Bering Land Bridge from north-east Asia approximately 13 000 years ago [4].
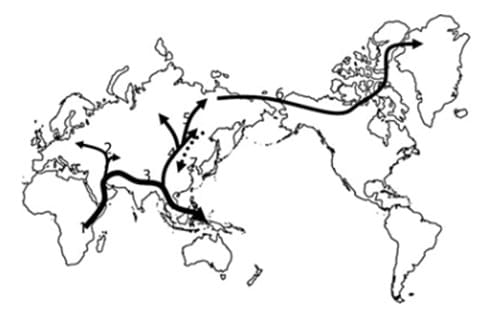
Figure 1: Migration Patterns Preceding the Evolution of PACG in Inuit Populations [4].
The four Inuit groups that resulted from this migration from Asia (Greenland Inuit, Siberian, Alaskan, and Canadian), have remained largely genetically isolated from the time of migration. As a result, the shallow anterior chamber, consistent with plateau iris associated with PACG, is considered most shallow in this population. (Figure 2) [4].
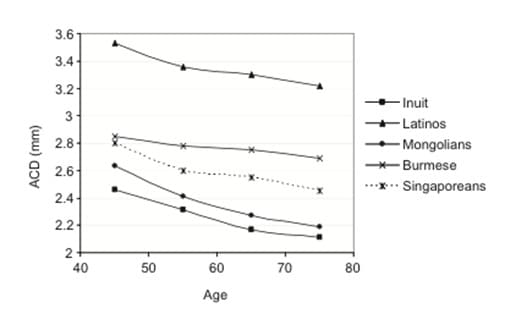
Figure 2: Anterior Chamber Depth in Various Populations [4].
One proposed evolutionary explanation for this genetic drift suggests that the shallow anterior chamber observed in this population may be an adaptation to cold climates. Alsbirk proposed that corneal freezing and desiccation keratitis results from prolonged exposure to extreme cold with high wind speeds, as in Arctic climates. He suggested that a shallow anterior chamber decreases the distance between the cornea and the vascular iris, preventing blindness as a result of freezing. He suggested that prevention of this morbidity produced an effective enough advantage to allow proliferation of this trait over time [5]. Unfortunately, this trait carried the disadvantage of PACG, seen in these populations today.
In 1921, Knud Rasmussen left Copenhagen, Denmark, on an expedition to ascertain the origin of the Eskimo race. He, along with a group of ethnographers, travelled to Greenland, and across the Canadian Arctic. The only population he did not visit inhabited the coast of Labrador, a group that one of his colleagues later visited to collect data for the report. Rasmussen’s most significant discovery was a common language known or used by the Eskimo throughout all of Alaska and Canada [6]. Linguistic and medical anthropological evidence reveal a connection between Northern China specifically, and Inuit populations. Therefore, the incidence of PACG among these populations can be dated back thousands of years.
A 2006 review proposes that PACG originates from a different disease process in East Asian populations in comparison with European populations. The study reports the predominant clinical manifestation of PACG as chronic angle closure in Asian populations, while this is not a common finding in European patients. They also report anatomical differences that may account for an etiological basis for PACG in Asian populations. The risk factors cited with respect to eye anatomy were small size, shallow anterior chamber, small corneal diameter, short axial length, steep curvature, thick, anterior lens, shallow limbal chamber, and plateau iris. Finally, and perhaps most importantly, the two mechanisms by which PACG occurs differ between populations. In European populations, pupil block is considered the primary etiology in the majority of patients, whereas this mechanism accounts for only 38% of PACG in Chinese patients. 54% of disease in this population could not be attributed to pupil block alone, but was considered a result of pupil block and flat iris, taking into account the anatomical differences described previously. It is of particular consideration that these anatomical differences were maintained throughout migration patterns that led to Inuit populations today.
This anatomical commonality has led to a significant burden of care in China, where blindness from PACG remains a source of morbidity in the population. Decreased quality of life as a result of PACG has even been reported as increased incidence of mental illness among patients with PACG. One study revealed an increased report of depression and anxiety in this population. This finding was specifically attributed to PCAG in contrast with POAG and controls [7].
In Canadian Inuit populations, a similar burden of disease is apparent. A large population study investigating ophthalmic conditions in Nain, Labrador revealed that 10.8% of 52-85 year olds in the study population were legally blind. This is in stark contrast to the Framingham Eye Study, where only 0.6% prevalence of legal blindness was found in the same age group in a population from Massachusetts. It was determined in 1984 that the prevalence of angle closure glaucoma in the Labrador Inuit population aged 40 years and over was 3.0% [8]. Similar prevalence rates were found in all Inuit populations along the migratory path described previously, in Greenland (4.8%), the Canadian Arctic (2.9%), and Alaska (2.65%) [9].
Decreasing burden of disease in Inuit populations is of high priority in Canadian health care at this time. The 2006 Canadian Census revealed that Canadian Inuit are the youngest and fastest growing population in Canada, with a 26% increase (total 50,485) in the number of Canadian citizens who identify as Inuit from the previous census in 1996. The census also found that the median age of the Inuit population was 22 years, compared with 40 for the non-Aboriginal population [10]. This evidence was corroborated by data specifically from the Nunatsiavut Inuit population in Labrador. In 2011 with the National Household Survey, revealing that at that time, the Nunatsiavut Inuit population was comprised of 2,330 individuals, increasing by 8%. Nearly half (44%) of that population were under the age of 25 at that time [11]. Given that this population is young and quickly growing, it demands early intervention for prevention of PACG, to decrease the high burden of ophthalmic disease in this population in the future.
The literature surrounding prevention and treatment of PACG is growing, particularly with the introduction of technologies allowing for improved diagnosis and treatment. Johnson and Foster reported in 2005 that screening for prevention should be determined specifically for individual at risk populations [9]. Therefore, we propose a screening and prevention program for PACG in the Nunatsiavut Inuit population of Labrador.
Case Presentation
A 67-year-old male of Inuit descent in Labrador was seen for a routine diabetes mellitus screening in ophthalmology clinic. Screening in this clinic includes tonometry, gonioscopy and fundus imaging with swept source optical coherence tomography (DRI OCT-1 Triton). There was no evidence of diabetic retinopathy in this patient. Increased pressure was observed on tonometry and a decreased angle was noted on ‘Radial Anterior Segment’ scan protocol, performed limbus to limbus using a 6mm, 2D scanning modality, producing scan resolution of 1024x12 of the cornea. Figure 3 and Figure 4 used this scanning modality prior to intervention to demonstrate the shallow anterior chambers of this patient, consistent with plateau iris commonly seen in the Inuit population. The patient provided consent for the utilization of this case for research.
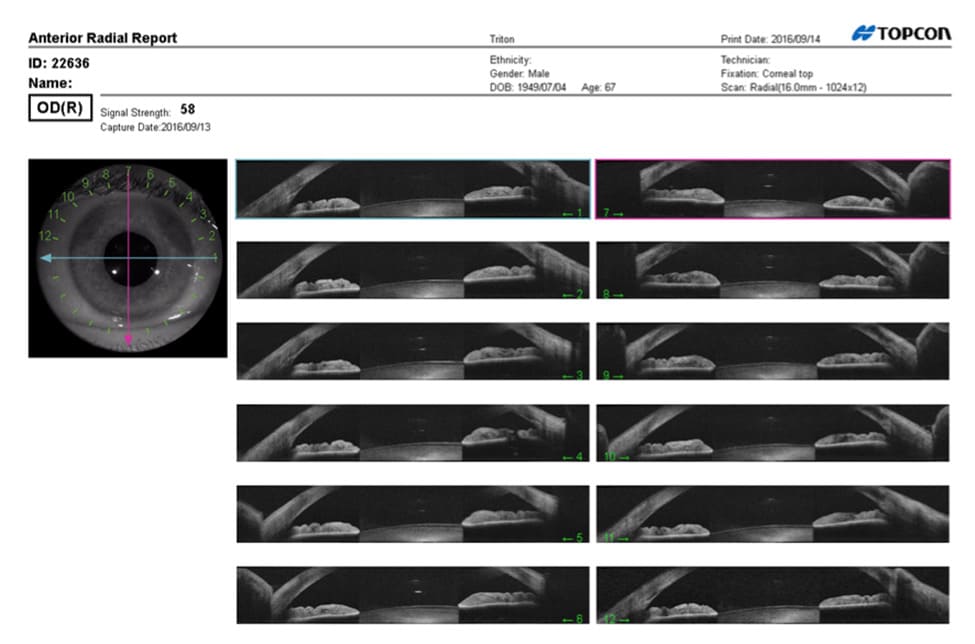
Figure 3: Radial Anterior Segment, OD, Pre-Treatment.
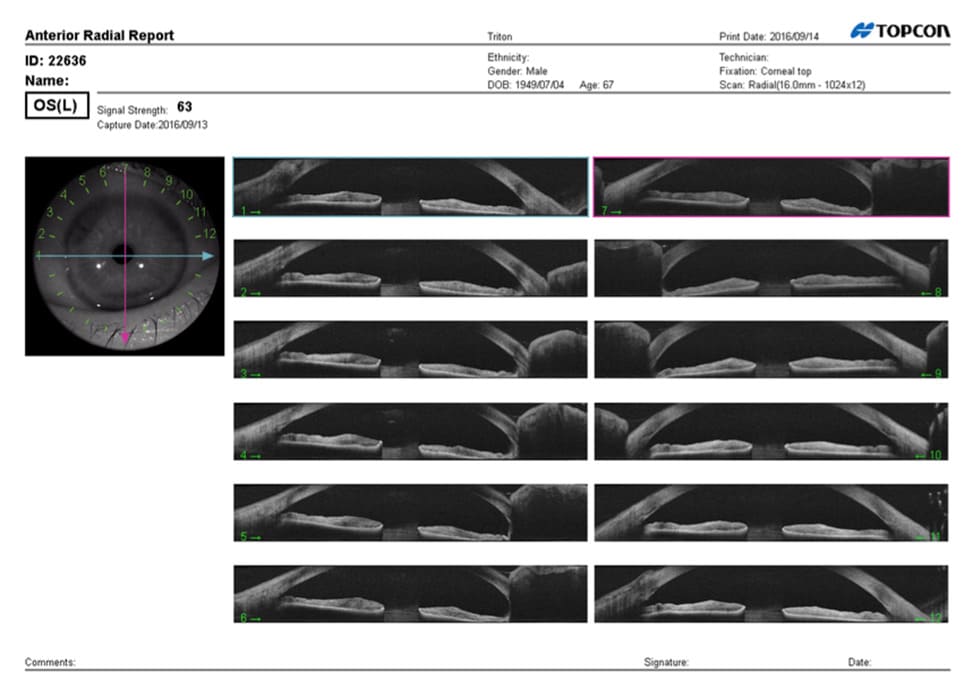
Figure 4: Radial Anterior Segment, OS.
During the same visit, OD ARGON laser peripheral iridoplasty was completed. Consent was obtained prior to the procedure. Images were captured the following day in follow-up, to determine angle 24 hours following the procedure. Figure 5 demonstrates Radial Anterior Segment of the right eye 24 hours following the procedure. Figure 6 also utilizes Radial Anterior Segment in 16mm with a scan resolution of 1024 × 12 of the cornea, in 2D modality. With use of this technology, the increase in anterior chamber angle is clearly visualized.
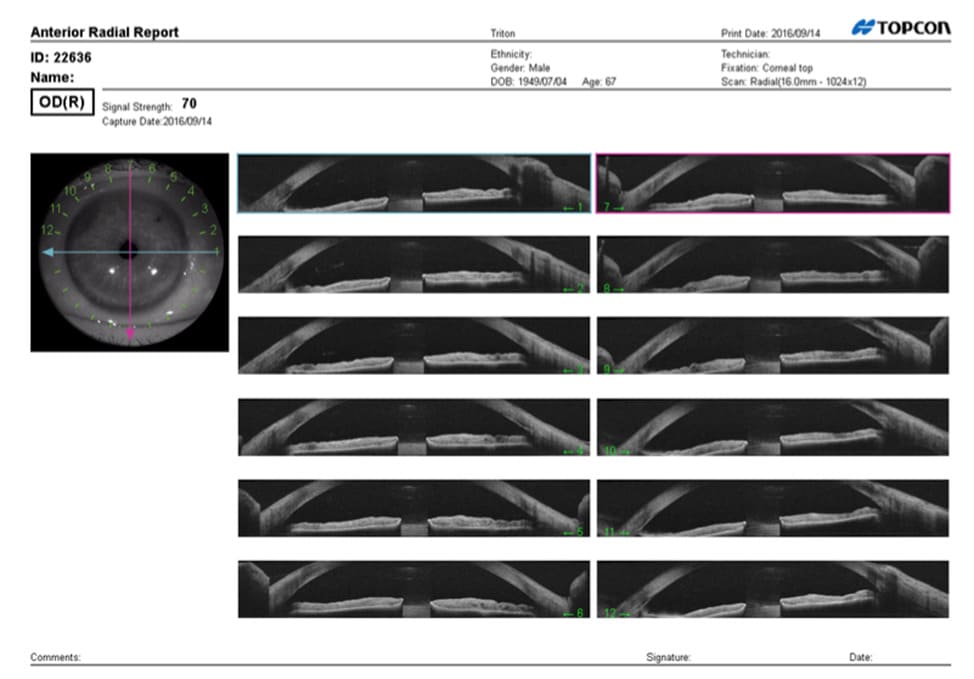
Figure 5: Radial Anterior Segment, OD, Post-Treatment.
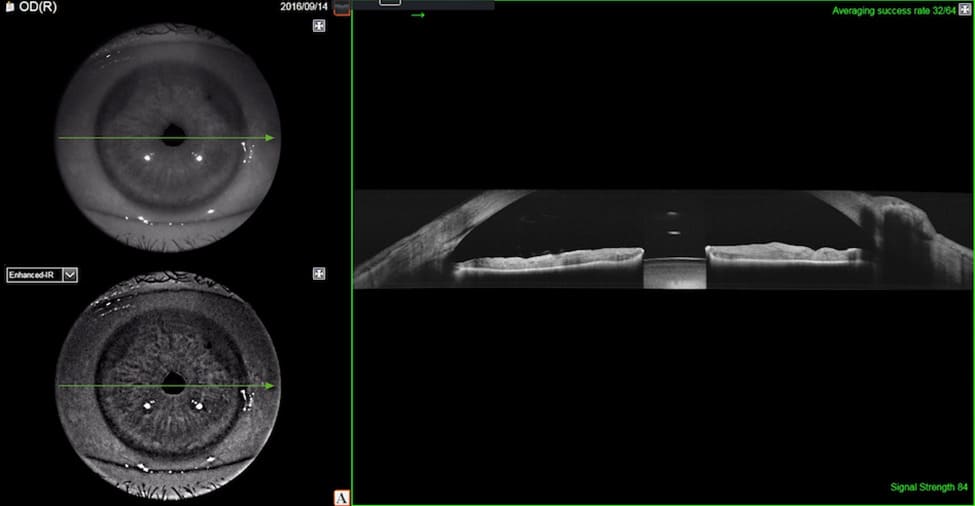
Figure 6: Radial Anterior Segment, 16mm, OD, Post-Treatment.
Figures 7-9 best demonstrate the increase in anterior chamber segment angle pre- and post-treatment with the use of ‘3D Anterior Segment’ scan protocol, a 3 × 3 mm scan with 512 × 256 cornea resolution. Figure 7 uses this technology to visualize a right anterior chamber segment prior to iridoplasty, while Figure 8 reveals a segment in the left eye. Figure 9 reveals the wide angle of the same anterior chamber segment in the right eye 24 hours following YAG laser peripheral iridoplasty. This is perhaps the most visually important image of this study. It provides clear evidence of the open anterior chamber angle of this patient following the procedure.
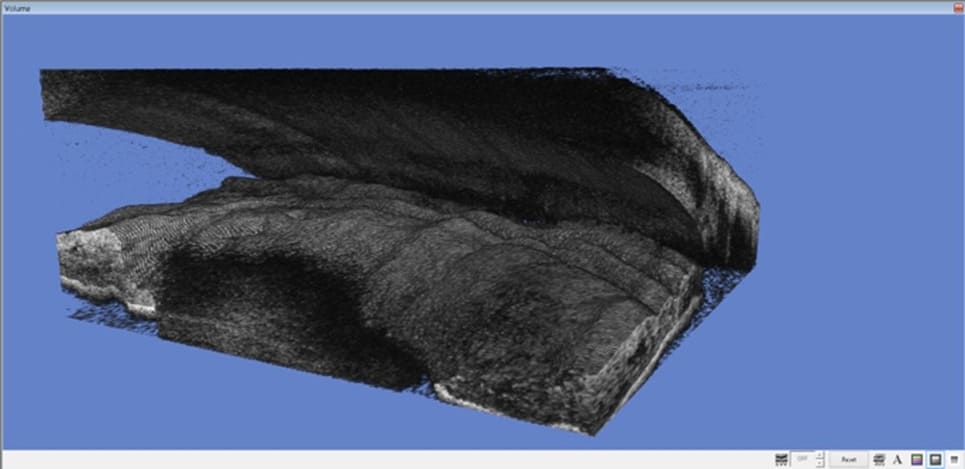
Figure 7: 3D Anterior Segment, OD, Pre-Treatment.
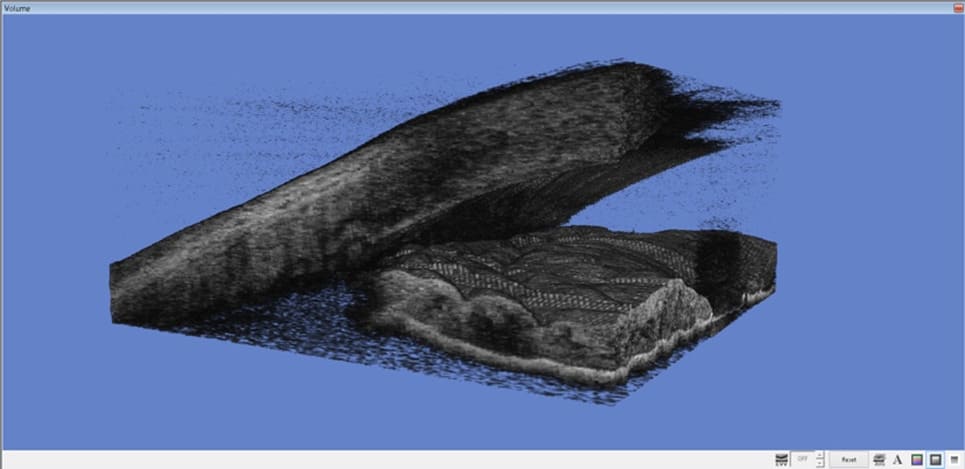
Figure 8: 3D Anterior Segment, OS.
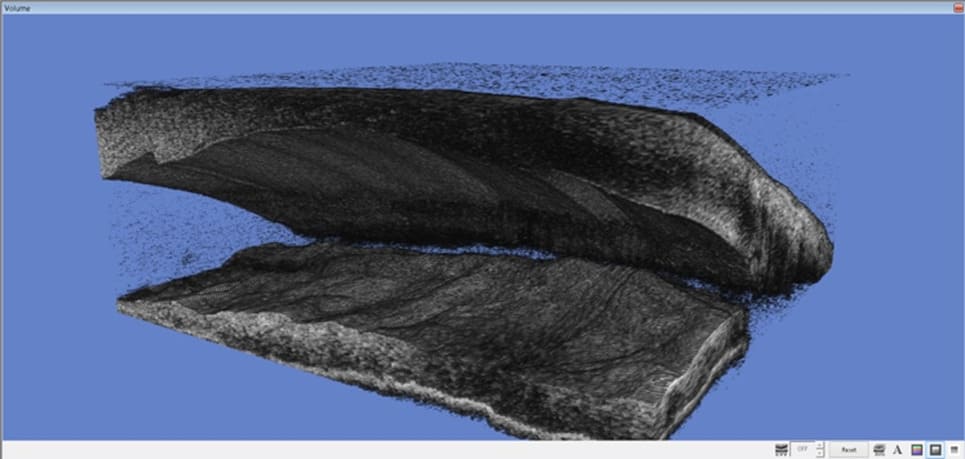
Figure 9: 3D Anterior Chamber, OD, Post-Treatment.
We propose based on our observations and the data presented above, as well as the images provided, that the form of glaucoma found in Mongolian and Inuit populations presents not an acute problem but a more chronic and indolent disease process. In contrast, glaucoma found in Caucasian populations involves a pupillary block mechanism with secondary change in pressure dynamics may cause acute or a chronic problem, or both. Further research will investigate pressure dynamic changes in these populations to further delineate etiology of PACG.
In addition, there has been significant debate in the literature as to the long-term efficacy of either goniotomy or iridoplasty, as well as the repeatability of these procedures and whether that provides benefit. However, the literature is equally unclear as to whether or not peripheral iridotomy prevents the progression of the form of glaucoma found in Asian and Inuit populations.
Finally, we propose that this classification of glaucoma in eyes of different ethnic origin should be divided into: ‘primary pupillary block with a bowed iris’, ‘plateau iris’, and finally ‘open angle’. With evidence from DNA analyses, it can be inferred that PACG in Asian and Indian populations may be secondary to a form of plateau iris to which these populations are predisposed by ancestry. Collaboration between Inuit and Chinese to make screening through refined imaging techniques, particularly newer swept source optical coherence tomography, followed by effective newer treatment paradigms can significantly reduce blindness in both populations.
References
- Quigley HA, Broman AT (2006) The number of people with glaucoma worldwide in 2010 and 2020. Br J Opthalmol 90: 262-267.
- Wong TY, Loon SC, Saw SM (2006) The epidemiology of age related eye diseases in Asia. Br J Opthalmol 90: 506-511.
- Kumar RS, Tantisevi V, Wong MH, Laohapojanart K, Chansanti O, et al. (2009) Plateau iris in Asian subjects with primary angle closure Arch Opthalmol 127: 1269-1272.
- Casson RJ (2008) Anterior chamber depth and primary angle-closure glaucoma: an evolutionary perspective. Clinical and Experimental Opthalmology 36: 70-77.
- Alsbirk PH (1976) Primary angle-closure glaucoma. Oculometry, epidemiology, and genetics in a high risk population. Acta Opthalmol Suppl 127: 5-31.
- Treude E (2004) The work of Knud Rasmussen in the Canadian Arctic as described by RCMP Inspector Stuart Wood. Etudes Inuit Studies 28: 185-201.
- Kong X, Yan M, Sun X, Xiao Z (2015) Anxiety and depression are more prevalent in primary angle closure glaucoma than in primary openangle glaucoma. J Glaucoma 24: e57-e63.
- Johnson GJ, Green JS, Paterson GD, Perkins ES (1984) Survey of ophthalmic conditions in a Labrador community: II. Ocular disease. Can J Opthalmol 19: 224-233.
- Johnson GJ, Foster PJ (2005) Can we prevent angle-closure glaucoma? Eye 19: 1119-1124.
- Statistics Canada (2006) 2006 Census: Aboriginal Peoples in Canada in 2006: Inuit, Metis and First Nations.
- Statistics Canada (2011) The 2011 National Household Survey.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.