The Carotid Web as a Cause of Cryptogenic Stroke in a Young Patient: Diagnosis and Treatment
by Rim Moufakkir*, Hajar Naciri Darai, Dahab Ouhabi, Houyam Tibar, Wafa Regragui
Neurology B and Neurogenetics Department, Specialties Hospital, Ibn Sina Teaching Hospital, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University in Rabat, Rabat, Morocco.
*Corresponding author: Rim Moufakkir, Neurology B and Neurogenetics Department, Specialties Hospital, Ibn Sina Teaching Hospital, Faculty of Medicine and Pharmacy of Rabat, Mohammed V University in Rabat, Rabat, Morocco.
Received Date: 13 May, 2025
Accepted Date: 20 May, 2025
Published Date: 23 May, 2025
Citation: Moufakkir R, Darai NH, Ouhabi D, Tibar H, Regragui W (2025) The Carotid Web as a Cause of Cryptogenic Stroke in a Young Patient: Diagnosis and Treatment. Int J Cerebrovasc Dis Stroke 08: 198. https://doi.org/10.29011/2688-8734.100198.
Abstract
Carotid Webs (CWs) are rare, non-atherosclerotic intraluminal abnormalities increasingly recognized as a potential cause of ischemic stroke, particularly in young adults without traditional vascular risk factors. We report the case of a 48-year-old man with no significant medical history, who presented with sudden-onset left hemiplegia and dysarthria. Brain imaging revealed a complete right middle cerebral artery infarction. Extensive etiological workup was unremarkable. Vascular imaging identified a thin, linear defect in the posterior wall of the right carotid bulb, consistent with a carotid web. The patient partially recovered with supportive care, was started on oral anticoagulation, and referred for vascular surgery. CWs are often asymptomatic until they cause embolic strokes. They are underdiagnosed and may be responsible for a significant proportion of cryptogenic strokes. Diagnosis is primarily based on cervical CT angiography, while MRI and Doppler ultrasound may lack sensitivity. Given the high risk of recurrence, particularly in the same vascular territory, more definitive treatment options such as surgical endarterectomy or carotid artery stenting should be considered. Carotid webs should be included in the differential diagnosis of cryptogenic stroke, especially in younger patients. Timely recognition through appropriate imaging and multidisciplinary management is essential to prevent recurrence.
Introduction
Ischemic stroke can result from a wide range of etiologies, most commonly atherosclerosis or cardioembolism [1].
However, carotid or vertebral artery webs represent a rare, nonatherosclerotic vascular cause of ischemic stroke, particularly in young adults. First described in the 1970s, this condition remains underrecognized in clinical practice [2]. In this report, we describe the case of a young patient with ischemic stroke secondary to a carotid web and review its frequency, characteristic imaging features, and therapeutic management.
Case Presentation
We report here the case of a 48-year-old right-handed man with a history of active smoking estimated at 20 pack-years. He had no known history of diabetes, hypertension, consanguinity, or similar familial cases. He was admitted for sudden-onset leftsided weakness, accompanied by right-sided facial deviation and dysarthria. The patient presented outside the window for recanalization therapy. Neurological examination revealed left hemiplegia, a right central facial palsy, and dysarthria. Cardiovascular and general physical examinations were unremarkable. A non-contrast head CT revealed a complete right Middle Cerebral Artery (MCA) territory infarction.
A comprehensive etiological workup for ischemic stroke in a young adult—including ECG, transthoracic and transesophageal echocardiography, cervical-transcranial ultrasound, serologic tests, and inflammatory markers—was entirely negative. Cerebral MRI with arterial angiography revealed a thin, linear filling defect along the posterior-lateral wall of the right carotid bulb, consistent with a right carotid web, which was identified as the likely cause of the infarct (Figure 1).
The patient showed partial motor recovery over time. He was initiated on oral anticoagulation and referred to a vascular surgery unit for further management.
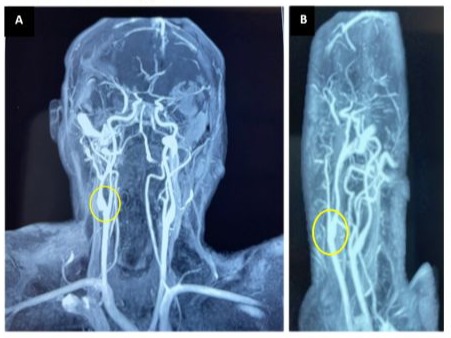
Figure 1: Cerebral MR angiography: Sagittal view (A) and coronal view (B) showing a right carotid web, appearing as a linear filling defect along the posterior-lateral wall of the right carotid bulb.
Discussion
Our patient experienced an ischemic stroke attributed to a carotid web (CW), diagnosed based on characteristic imaging findings and after exclusion of other potential causes, particularly given the patient’s young age. Carotid webs are considered a rare, nonatherosclerotic arteriopathy and are currently classified as a focal variant of fibromuscular dysplasia (FMD). Histologically, CWs are composed of a loose myxoid matrix containing few spindleshaped cells, gradually replaced by fibrous tissue and lacking elastic fibers. This proliferation primarily involves the intimal layer, to a lesser extent the media, and shows no evidence of inflammation, calcification, or lipid accumulation [2]. Carotid webs are a potential source of artery-to-artery embolism, especially in cryptogenic strokes in young adults.
The pathophysiological mechanism most commonly proposed is the formation of mural thrombus due to flow stagnation just distal to the web, which can subsequently embolize to intracranial arteries [3]. These lesions are typically located at the posterior wall of the carotid bulb, a region prone to flow disturbances.
Carotid webs are often asymptomatic until they cause a cerebral infarction, typically categorized as cryptogenic in origin. Studies estimate that CWs may account for 9.5% to 37% of cryptogenic ischemic strokes in young adults [4]. Stroke related to a CW is always ipsilateral to the lesion and classically involves the posterior segment of the carotid bulb [5].
The condition appears to be more prevalent in young women under 55 years old and disproportionately affects individuals of African descent, often in the absence of traditional vascular risk factors [6]. As a non-invasive diagnostic tool, Doppler ultrasound has limited diagnostic value, especially in cases of cervical artery dissection, as the blood flow may appear normal due to the absence of significant stenosis. In our patient, the Doppler study was normal. At best, it may show indirect signs suggestive of dissection. The diagnosis was established by MRI angiography, although it showed only minimal stenosis and no clear signs of arterial rupture.
The cervical CT angiogram is considered the imaging modality of choice, where the web is visualized as an endoluminal defect, typically broader than it is tall, located opposite the external carotid artery. Variants may appear as thin or thick membranes. However, the classic appearance can be temporarily obscured by superimposed thrombus. When non-invasive techniques fail to identify the web, catheter angiography may be warranted, particularly in cases of recurrent strokes within the same vascular territory [6,7].
By contrast, MRI angiography (MRA) has shown lower sensitivity in detecting carotid webs. When visible, the lesion appears as a homogeneous structure, showing mild T1 hyperintensity, isointensity on T2, and a linear pattern of contrast enhancement— without signs of intraplaque hemorrhage, necrotic lipid core, or fibrous cap rupture but in our case it make the diagnostic [8,9].
Although typically non-stenotic, symptomatic carotid webs are associated with a high risk of recurrent ischemic events, with recurrence rates ranging from 24% to 71% depending on the series, most often within the same vascular territory. Recurrence may occur as early as within the first 30 months following the initial event [7]. For our patient, this was the first vascular event related to cervical artery dissection, as there was no other focal neurological deficit and no subclinical lesions on brain MRI.
Because of this substantial recurrence risk, secondary prevention requires more aggressive strategies than standard antiplatelet therapy, which has shown limited efficacy. Both surgical endarterectomy and endovascular stenting are considered firstline treatment options. Stenting is often preferred in younger patients with favorable vascular anatomy, offering a minimally invasive and effective solution when arterial tortuosity does not compromise catheter navigation [10].
Conclusions
Carotid webs represent a rare and underrecognized cause of ischemic stroke, particularly in young adults. Non-invasive imaging—such as Doppler ultrasound, CT angiography, and MR angiography—facilitates diagnosis, though sensitivity varies among modalities. The limited effectiveness of anticoagulants or antiplatelet agents alone in preventing recurrence highlights the importance of considering surgical or endovascular interventions for long-term management in selected patients.
References
- Yahyaoui A, Chatou N, Bouchal S (2020) Accident vasculaire cérébral ischémique sur diaphragme artériel. Rev Neurol (Paris) 176(Suppl): S110.
- Houdart E (2018) Le diaphragme du bulbe carotidien : Une cause souvent méconnue d’AVC du sujet jeune. JMV-Journal de Médecine Vasculaire 43: 108–109.
- Gee W, Burton R, Stoney RJ (1974) Atypical fibromuscular hyperplasia involving the carotid artery. Ann Surg 180: 136–138.
- Coutinho JM, Derkatch S, Potvin AR, Tomlinson G, Casaubon LK, et al. (2017) Carotid artery web and ischemic stroke: a case-control study. Neurology 88: 65–69.
- Gopal N, Puc MM, Grossman AW, Treiman GS (2020) Vessel wall imaging of carotid web. Neurology 94: e620–e624.
- Joux J, Chausson N, Jeannin S, Saint-Vil M, Mejdoubi M, et al. (2014) Carotid-bulb atypical fibromuscular dysplasia in young Afro-Caribbean patients with stroke. Stroke 45: 3711–3713.
- Choi PMC, Singh D, Trivedi A, Qazi E, George D, et al. (2015) Carotid webs and recurrent ischemic strokes in the era of CT angiography. AJNR Am J Neuroradiol 36: 2134–2139.
- Joux J, Mejdoubi M, Quere J-B, Colombani S, Hennequin J-L, et al. (2016) MRI characteristics of carotid bulb atypical fibromuscular dysplasia in Black stroke patients. J Neuroradiol 43: 214–217.
- Fu W, Crockett A, Low G, Patel V (2015) Internal carotid artery web: Doppler ultrasound with CT angiography correlation. J Radiol Case Rep 9: 1–6.
- Lenck S, Labeyrie MA, Saint-Maurice JP, Tarlov N, Houdart E (2014) Diaphragms of the carotid and vertebral arteries: an under-diagnosed cause of ischaemic stroke. Eur J Neurol 21: 586–593.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.