The Association Between Vitamin D and Lung Cancer Risk and Survival: A Systematic Review
by Andrej Roj1*, Jörg Lindenmann1, Paul Swatek1, Iurii Mykoliuk1, Anton Busau1, Edin Ahmic1, Gudrun Pregartner2, Andrea Berghold2
1Division of Thoracic Surgery, Department of Surgery, Medical University of Graz, Austria.
2Institute for Medical Informatics, Statistics and Documentation, Medical University of Graz, Austria.
*Corresponding author: Roj A, Division of Thoracic Surgery, Department of Surgery, Medical University of Graz, Austria.
Received Date: 11 February, 2026
Accepted Date: 23 February, 2026
Published Date: 27 February, 2026
Citation: Roj A, Lindenmann J, Swatek P, Mykoliuk I, Busau A, et al. (2026) The Association between Vitamin D and Lung Cancer Risk and Survival: A Systematic Review. J Oncol Res Ther 11: 10331. DOI: https://doi.org/10.29011/2574-710X.10331
Abstract
Background: Lung cancer represents a significant challenge for public health worldwide. Multiple genetic and metabolic elements contribute critically to the pathogenesis of this disease, with vitamin D being among these influential factors; however, the relationship between vitamin D and lung cancer has yet to be definitively established. Methods: An extensive literature search was conducted using the following databases: PubMed, Medline, Embase, Cochrane Library and Web of Science. After application of the inclusion (studies of human populations, RCTs, cohort or case–control studies) and exclusion criteria (non-original articles, articles with insufficient data on vitamin D supplementation or survival, studies conducted on animals, studies of benign diseases), seven suitable studies were included in this review. The risk of bias was evaluated using the Newcastle–Ottawa Scale (NOS) for observational studies and the Cochrane Collaboration´s Risk of Bias (RoB2) tool for randomized controlled trials (RCTs). Results: Four studies assessed the impact of vitamin D on the survival of patients with lung cancer, and three evaluated its impact on the incidence of lung cancer. The included studies were narratively summarized, and their results were compared with one another. Conclusions: This systematic review analyzed the available literature regarding the association between vitamin D and the prognosis and incidence of lung cancer. The association between vitamin D and lung cancer risk and survival still needs to be investigated.
Keywords: Vitamin D; Lung Cancer; Survival; Incidence; Review
Introduction
Lung cancer represents a major global public health concern and is responsible for substantial mortality worldwide. According to the GLOBOCAN 2020 estimates of cancer incidence and mortality from the International Agency for Research on Cancer (IARC), lung cancer continues to be the primary cause of cancer-related deaths, accounting for approximately 1.8 million fatalities in 2020. Therefore, early diagnosis and prevention are essential for decreasing the incidence and mortality of this disease [1].
Vitamin D exerts its biological actions via vitamin D receptors (VDRs), and the widespread presence of VDRs throughout various bodily tissues and cells indicates that vitamin D has diverse functions extending beyond its role in bone metabolism [2].
However, vitamin D is biologically inactive and requires sequential hepatic and renal hydroxylation to produce its active metabolite, 1,25-dihydroxycholecalciferol [1,25(OH)2D3]. Ultraviolet radiation catalyzes cutaneous synthesis of vitamin D3, which undergoes hepatic hydroxylation to 25-hydroxycholecalciferol. Renal 1α-hydroxylase then converts this intermediate to 1,25(OH)2D3, the most biologically potent form of vitamin D [3].
Vitamin D Vitamin D is acquired from three sources: dietary intake, supplements, and UVB radiation. UVB-induced synthesis provides approximately 80% of vitamin D supply, while dietary sources play a secondary role. In Europe and North America, common foods contain minimal vitamin D, with only select items (fatty fish, mushrooms, fortified products) providing substantial amounts. Supplements deliver significantly higher doses than dietary sources [4]. Given frequent deficiencies in both dietary intake and endogenous synthesis, particularly during winter and with reduced sun exposure, supplementation is strongly recommended for all age groups [5].
As a steroid hormone, vitamin D is essential for regulating calcium and bone homeostasis in the body. It enhances intestinal absorption of this mineral and critically influences both bone formation and bone resorption processes [6]. However, it also possesses a much broader spectrum of biological activities, and, consequently, vitamin D deficiency enhances the incidence and severity of a huge variety of common age-related diseases, such as type 2 diabetes, hypertension, obesity, pregnancy complications, memory disorders, osteoporosis, certain cancers, autoimmune diseases and systemic inflammatory diseases [7].
Most significantly for this review, emerging evidence indicates vitamin D possesses anti-neoplastic properties through multiple mechanisms, including G1 phase cell cycle arrest, cellular differentiation, apoptosis induction, signaling pathway modulation, and angiogenesis suppression. Vitamin D modulates apoptotic regulators by downregulating anti-apoptotic proteins (BCL2, BCL-X) and upregulating pro-apoptotic proteins (BAX, BAK, BAD) [8].
In cancer, vitamin D inhibits angiogenesis, a critical step in tumor growth, with reduced neovascularization observed in prostate and lung murine models. Additionally, vitamin D suppresses metastatic progression of lung cancer cells, with murine studies demonstrating an inverse correlation between circulating 1,25(OH)2D concentrations and tumor proliferation [9]. In Lewis lung carcinoma models, vitamin D treatment enhanced intratumoral T-cell immune responses while reducing both metastasis and locoregional tumor recurrence [10].
In humans, 1,25(OH)2D exerts antiproliferative effects by upregulating adhesion proteins including E-cadherin and catenins, which strengthen intercellular connections and reduce malignant cell migration into lymphatic and vascular systems. Decreased expression of these adhesion molecules correlates with local invasion, metastasis, and poor survival in NSCLC [11].
Vitamin D induces G1 cell-cycle arrest by activating cyclindependent kinase inhibitors p21 and p27, which interact with the ras-oncogene family; K-ras mutations are common in adenocarcinoma [12].
The effects of vitamin D on various cancer types are extremely heterogenous and sometimes contradictory. Initially, An inverse relationship between serum 25(OH)D levels and colorectal cancer risk was demonstrated in a 2016 meta-analysis by Ekmekcioglu [13]. Consistent with these findings, McCullough et al. (2019) reported in over 5000 patients that elevated 25(OH)D levels correlated with significant risk reduction in women and non-significant reduction in men [14]. Yet a large randomized controlled trial by WatcawskiWende et al. found no effect of vitamin D supplementation on the incidence of this neoplasm [15].
In prostate cancer, a meta-analysis by Xu et al. demonstrated a significant 17% increase in disease risk among patients with elevated 25(OH)D serum levels [16]. Conversely, a study by Attila et al. found no significant difference in overall survival between placebo and intervention groups [17].
In breast cancer, a 2019 meta-analysis by Hossain et al. identified a link between vitamin D deficiency and disease occurrence, with an inverse relationship also noted for supplementation [18]. Additionally, a meta-analysis by Kim et al. suggested that elevated blood 25(OH)D levels are weakly associated with reduced risk of this malignancy [19].
On the other hand, there is no statistically significant association between vitamin D and several other cancers, including gastric, esophageal, pancreatic and skin cancer [20, 21]. Regarding the association between vitamin D and lung cancer, the data remains inconclusive. Consequently, the aim of this systematic review is to analyze the literature regarding the association between vitamin D and the incidence and survival rates of lung cancer.
Methods
Literature Search
A comprehensive literature review was performed in March 2025 using the following databases: PubMed, Medline, Embase, Cochrane Library and Web of Science. This investigation was conducted by a thoracic surgeon in collaboration with a scientific librarian experienced in retrieving scientific publications. The query strategy consisted of free-text terms as well as medical subject headings, as follows: (((lung OR pulmonary OR bronchial OR bronchogenic) AND (cancer OR carcinoma OR neoplasms OR adenocarcinoma OR squamous carcinoma)) OR (non-small cell lung cancer OR small cell lung cancer OR NSCLC OR SCLC)) AND (vitamin D OR vitamin D supplementation OR dietary vitamin D intake). Additionally, a manual examination of references cited in the selected articles was performed (Figure 1).
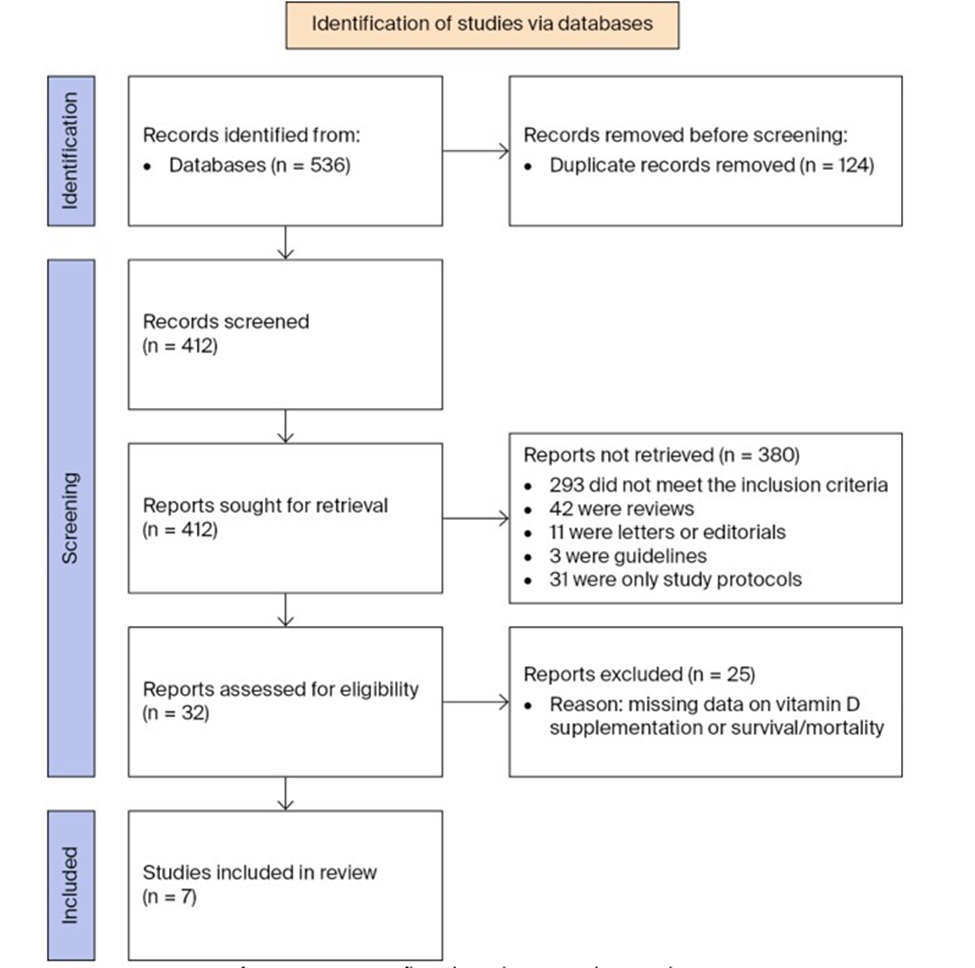
Figure 1: PRISMA flowchart depicting the search strategy.
Study Selection
The inclusion criteria were as follows: (1) studies on human populations, (2) randomized controlled trials (RCTs), and cohort or case-control studies. The exclusion criteria comprised: (1) non-original articles, (2) studies with inadequate reporting of vitamin D supplementation data or survival/mortality outcomes, (3) studies conducted on animals, (4) benign diseases. The search was conducted in March 2025. Three studies addressed the association between vitamin D and lung cancer survival (Table 1), and four studies covered the association between vitamin D and lung cancer risk (Table 2).
|
Author |
Year |
Country |
Study Design |
Number of Patients |
Vitamin D |
Outcome |
|
Supplementation |
||||||
|
Zhou |
2005 |
USA |
Observational |
456 |
No |
Improved RFS in patients with higher vitamin D intake who had surgery during summer |
|
Akiba |
2018 |
Japan |
RCT |
155 |
Yes |
Improved OS and RFS in subgroup with early-stage adenocarcinoma with low 25 (OH)D |
|
Weinstein |
2022 |
USA |
Observational |
450 |
No |
Improved OS of patients with higher serum vitamin D levels |
Table 1: Characteristics of the studies evaluating the association between vitamin D and lung cancer survival.
|
Author |
Year |
Country |
Study Type |
Number of Patients |
Vitamin D |
Outcome |
|
Supplementation |
||||||
|
Takata |
2009 |
China |
Observational |
79,941 |
Yes |
No association |
|
Cheng |
2013 |
USA |
Observational |
1,28,779 |
Yes |
Lower incidence of lung cancer in non-smoking postmenopausal women with a total vitamin D intake > 400 IU/d |
|
Redaniel |
2014 |
UK |
Observational |
484 |
Yes |
No association |
|
Zhu |
2018 |
Australia |
Observational |
3818 |
No |
No association |
Table 2: Characteristics of the studies evaluating the association between vitamin D and lung cancer incidence.
Data extraction and assessment of the articles
All articles identified by the initial search were screened for eligibility by two authors based on title and abstract. Disagreements were resolved by consensus after discussion. The final step was assessment of the full publication.
Risk-of-bias evaluation
The quality of the observational studies and randomized controlled trials (RCTs) was assessed using the Newcastle–Ottawa Scale (NOS) and Cochrane Collaboration´s Risk of Bias (RoB2) tool, respectively. The NOS has separate versions for cohort studies and case–control studies, as shown in Tables 3 and 4, respectively [22]. The RoB2 tool assesses the following domains (Table 5): 1) potential bias from the randomization process, 2) deviations from intended interventions (including effects of assignment and adherence), 3) incomplete outcome data, 4) measurement error in outcomes, 5) selective reporting of results. For observational studies, quality was evaluated across three dimensions: 1) selection criteria (0-4 stars), 2) comparability measures (0-2 stars), and 3) outcome/exposure assessment (0-3 stars). We categorized the results as “good” (studies with at least seven stars), “acceptable” (studies with four to six stars) or “substandard” (studies with three stars or fewer) quality (Figure 2).
|
NOS-Cohort Studies |
|||||
|
Components |
Zhou (2005) |
Weinstein (2022) |
Takata (2009) |
Cheng (2013) |
Zhu (2018) |
|
Selection |
|||||
|
Representativeness of the exposed cohort |
* |
* |
* |
* |
* |
|
Selection of the non-exposed cohort |
* |
* |
* |
* |
* |
|
Ascertainment of exposure |
* |
* |
* |
* |
* |
|
Demonstration that outcome of interest was not present at start of the study |
* |
* |
* |
* |
* |
|
Comparability |
|||||
|
Comparability of cohorts on the basis of design or analysis |
** |
** |
** |
** |
** |
|
Outcome |
|||||
|
Assessment of outcome |
* |
* |
* |
* |
* |
|
Enough follow-up time length for outcome to occur |
* |
* |
* |
* |
* |
|
Adequacy of follow-up of cohorts |
* |
||||
|
Study Quality |
|||||
|
Total Score |
8 |
8 |
9 |
8 |
8 |
|
Evaluation |
Good |
Good |
Good |
Good |
Good |
Table 3: Evaluation of the quality of the cohort studies using the Newcastle–Ottawa Scale.
|
NOS—Case–Control Study |
|
|
Components |
Redaniel (2014) |
|
Selection |
|
|
Is the case definition adequate? |
* |
|
Representativeness of the cases |
* |
|
Selection of controls |
* |
|
Definition of controls |
* |
|
Comparability |
|
|
Comparability of cases and controls on the basis of the design or analysis |
** |
|
Exposure |
|
|
Ascertainment of exposure |
* |
|
Same method of ascertainment for cases and controls |
* |
|
Non-response rate |
|
|
Study Quality |
|
|
Total Score |
8 |
|
Evaluation |
Good |
Table 4: Evaluation of the quality of the single case–control study using the Newcastle–Ottawa Scale.
|
RoB2 tool-RCT |
|
|
Domains |
Akiba (2018) |
|
Randomization process |
Low risk |
|
Deviation from the intended interventions |
|
|
Effect of assignment to intervention |
Low risk |
|
Effect of adherence to intervention |
Low risk |
|
Missing outcome data |
Low risk |
|
Measurement of the outcome |
Low risk |
|
Selection of the reported result |
Low risk |
|
Overall risk of bias |
Low risk |
Table 5: Evaluation of the single RCT using the RoB2 tool.

Figure 2: Evaluation of the quality of the cohort studies using the Newcastle–Ottawa Scale.
The included studies were narratively summarized and their results contrasted with each other. There was insufficient data available to perform a meta-analysis. This review was written in compliance with the PRISMA guidelines.
Results
After searching the abovementioned databases, a total of 536 studies were identified. Figure 1 depicts the flowchart of the selection process. After deleting the duplicates and assessing the eligibility based on titles and abstracts, the full-text articles of 32 studies were screened, and an additional 25 studies were eliminated due to a lack of relevant data. Finally, seven studies were included in this review: six observational studies and one RCT.
The principal characteristics of the four studies examining the relationship between vitamin D and lung cancer prognosis are outlined in Table 1 and the key features of the three studies assessing the link between vitamin D and lung cancer incidence in Table 2.
Vitamin D and Lung Cancer Survival
Two of the three studies on the association between vitamin D and lung cancer survival were performed in the USA, and the third in Japan. The sample size ranged from 450 to 456 in the observational studies, while the RCT included two arms with 77 and 78 patients, respectively. The median follow-up period ranged from 3.3 to 15.6 years. Serum vitamin D levels were measured in two studies, and one study assessed the vitamin D levels based on food questionnaires. Only one study actively supplemented vitamin D.
Zhou et al. conducted an initial investigation in 2005 on the relationship between vitamin D and lung cancer survival outcomes. They analyzed how surgical timing (by season) and vitamin D consumption correlated with recurrence-free survival (RFS) and overall survival (OS) in 456 patients with early-stage non-small-cell lung cancer. Surgical procedures were evenly distributed across seasons: 140 patients (31%) in winter, 165 (36%) during spring/fall and 151 (33%) in summer. The cohort was predominantly Caucasian (96%), and the median follow-up period was 5.9 years. Vitamin D consumption ranged from less than 239 IU/d in the lowest quartile to 596 IU/d in the highest, and no significant statistical correlation emerged between vitamin D consumption alone and RFS (HR of highest versus lowest quartile = 0.85, 95% CI = 0.56–1.28, p = 0.66). Nevertheless, both seasonal variation and dietary intake influenced vitamin D status. Individuals who underwent surgery in summer and had maximum vitamin D consumption demonstrated a superior RFS rate (HR = 0.33, 95% CI = 0.15–0.74) compared to those whose surgeries were during winter and had minimal vitamin D intake: 5-year RFS rates of 56% and 23%, respectively. Consequently, Zhou et al. concluded that the interaction between dietary vitamin D and surgical season was linked to survival in early-stage NSCLC patients. Notably, actual serum vitamin D concentrations were not directly measured; instead, consumption was assessed using a quantitative food frequency questionnaire (Harvard–Willett) and calculated via the Harvard database, an adapted version of the U.S. Department of Agriculture Nutrition Composition Laboratory’s food composition database. Participants were stratified into four intake categories (596 IU), with 35% reporting supplementation use [23].
In 2018, Akiba et al. conducted the inaugural randomized, double-blind, placebo-controlled trial investigating vitamin D supplementation in postoperative NSCLC patients. A total of 155 individuals were randomly allocated to either the vitamin D group (n=77) or the placebo arm (n=78), and the median follow-up duration was 3.3 years. Daily supplementation consisted of 1200 IU vitamin D in capsule form, and participants were prohibited from using additional vitamin D products. Serum 25(OH)D concentrations were determined via radioimmunoassay. Within the entire cohort, no statistically significant differences emerged for either RFS or OS; five-year RFS rates were 65% for the supplementation group versus 57% for the placebo (HR = 1.15, 95% CI = 0.64-2.05, p = 0.64), while 5-year OS rates were 76% and 78%, respectively (HR = 1.22, 95% CI = 0.54-2.79, p = 0.63). Conversely, a subgroup analysis restricted to early-stage adenocarcinoma patients with insufficient baseline vitamin D revealed significantly improved RFS (86% vs. 50%, P=0.04) and OS (91% vs. 48%, P=0.02) in the treatment arm. Thus, while supplementation failed to enhance survival across the entire population, the limited sample size may have been inadequate for detecting meaningful effects. Furthermore, the intervention period was restricted to 12 months at a daily dose of 1200 IU; extended treatment durations or higher dosages might have produced different outcomes. Despite the relatively modest enrollment numbers, this investigation’s primary strength lies in being the first randomized, double-blind, placebocontrolled trial examining whether vitamin D supplementation influences NSCLC patient survival [24].
Weinstein et al. (2022) investigated the relationship between vitamin D status and cancer survival among 4038 patients with various malignancies over a median follow-up period of 15.6 years as part of the Prostate, Lung, Colorectal and Ovarian Cancer Screening Trial, which included 450 lung cancer cases. Comparisons between the highest (34.8 ng/ml) and lowest (13.1 ng/ml) quintiles of circulating vitamin D revealed that elevated serum vitamin D levels correlated with improved overall cancer survival (HR = 0.83, 95% CI = 0.70–0.98; P = 0.05) and specifically enhanced lung cancer survival (HR = 0.63, 95% CI = 0.44–0.90; P = 0.03). Baseline 25(OH)D measurements were obtained through radioimmunoassay, chemiluminescence immunoassay or liquid chromatography–mass spectrometry. While the investigation demonstrated a statistically significant link between vitamin D and lung cancer survival, it is important to note that the cohort was predominantly white (87.9% of participants). This demographic characteristic is noteworthy given the well-documented disparities in 25(OH)D concentrations observed between black and white populations [25].
Vitamin D and Lung Cancer Risk
Concerning the relationship between vitamin D and lung cancer development, investigations were performed in four countries: the United States, China, the United Kingdom and Australia. The number of participants ranged from 484 to 128,779, and the median follow-up duration spanned from 5 to 20 years. Two studies relied on food questionnaires to determine the basic vitamin D levels, one measured the serum vitamin D levels and one was a case– control study that focused only on supplementation.
No association was observed between vitamin D and lung cancer risk in the study performed by Takata et al. in 2009. The study included 71,267 female Chinese non-smokers, and vitamin D intake was calculated using an interviewer-administered food frequency questionnaire during home visits. However, serum vitamin D levels were not measured. According to the cancer registry databases, a total of 428 lung cancer cases occurred during a median follow-up duration of 11.2 years. Among these 428 cases, 45 cases had missing information for vitamin D-containing supplements. For this reason, the analysis included a total of 383 cases, among which one group (93 cases) consumed vitamin D supplements and the other (290 cases) did not. The consumption of vitamin D supplements was not significantly associated with the risk of lung cancer (HR = 1.11, 95% CI = 0,87 – 1,41, p = 0.40). However, it is worth mentioning that, in this study, patients were merely separated into two groups regarding the use of vitamin D-containing supplements (yes/no); information about the dosage of the vitamin D supplements consumed was not gathered, information on sunlight exposure was not collected and serum vitamin D levels were not measured [26].
Cheng et al. (2013) examined the relationship between vitamin D consumption and lung cancer development in 128,779 postmenopausal women enrolled in the Women’s Health Initiative trial. Baseline total consumption encompassed both dietary sources (assessed via food frequency questionnaires) and supplementation. No significant correlation emerged across the entire cohort. However, among those who had never smoked, reduced lung cancer occurrence was noted in those consuming more than 400 IU/d of total vitamin D. Relative to an intake below 100 IU/d, consumption exceeding 400 IU/d demonstrated significantly decreased lung cancer occurrence across multiple intake levels: 400 to 800 IU/d (HR = 0.37, 95% CI = 0.18-0.77; P = 0.01). Additionally, in a vitamin D intervention trial involving 36,282 women and 400 IU/d supplementation over eight years with rigorous monitoring, the supplemented group exhibited a non-significant 13% reduction in lung cancer occurrence compared with controls (HR = 0.87, 95% CI = 0.70-1.07) [27].
In their investigation utilizing the UK Clinical Practice Research Database, Redaniel et al. (2013) found no correlation between vitamin D and lung cancer development. Their case–control design included women aged 55 years and older with initial diagnoses of lung, breast, colorectal, ovarian or uterine malignancies as cases, while the controls consisted of cancer-free women frequencymatched by birth year, study entry date, follow-up duration and general practice, resulting in 484 lung cancer cases with a minimum 5-year follow-up period matched with 4553 common controls. Multivariable logistic regression analysis evaluated the relationship between vitamin D supplementation and cancer development odds for each malignancy type, and no association emerged between vitamin D supplementation and lung cancer occurrence [28].
A study performed by Zhu et al. in 2018 also failed to show an association between serum vitamin D and lung cancer risk. A total of 3818 participants with no history of cancer at baseline were included in the analysis, and over 90% of the population were of Anglo-Celtic ancestry. Blood samples were collected at baseline and serum vitamin D levels were determined using an assay methodology. Over the 20-year observation period, 212 participants succumbed to malignancies (36 lung, 22 colorectal, 15 breast, 17 prostate, 122 other), as documented in the cancer registry and mortality databases. No statistically significant correlation was identified between circulating vitamin D concentrations and either overall cancer development or lung cancer specifically. UV exposure was not taken into account in this study [29].
Discussion
Vitamin D is well known for its crucial role in calcium metabolism in the body. In addition to its metabolic activities, it also contributes to other processes of great importance, particularly carcinogenesis. While some studies have proven an association between vitamin D and a decreased risk of prostate and breast cancers, its role in lung cancer remains unclear.
The strengths of this review include the thorough literature search methodology, the independent screening procedures, the autonomous study selection and the rigorous quality assessment of the included studies. As shown in Table 3 and Figure 2, all of the studies were assigned at least eight stars or more and were graded as “good” quality. On the other hand, our review also has some limitations that must be acknowledged: First and foremost, we were unable to conduct a meta-analysis due to the substantial heterogeneity observed across the included studies. Thus, the implementation of meta-analytic techniques in a research context characterized by a greater number of methodologically comparable investigations might enable a more precise and accurate evaluation of the relationship between vitamin D levels and lung cancer outcomes. Secondly, our literature search methodology was specifically designed for and exclusively targeted lung cancer research. This focused approach meant we may have inadvertently overlooked certain studies that examine the association between vitamin D and multiple cancer types, where lung cancer is included as one among several malignancies investigated within the same research framework.
According to the recent RCT performed by Akiba et al., earlystage NSCLC adenocarcinoma patients appear to benefit from vitamin D supplementation in terms of recurrence-free survival and overall survival. However, these findings were limited to the subgroup with early-stage lung adenocarcinoma. This reflects a key aspect of oncological diseases, namely, that different cancer stages respond diversely to various treatments. Therefore, an RCT with a similar design but a larger sample size might show this association with higher precision.
Moreover, the current literature reveals a shortage of randomized controlled trials evaluating vitamin D’s impact on survival in NSCLC patients. The majority of research investigating this association employs an observational design; however, observational investigations are vulnerable to confounding variables and multiple sources of bias. In addition, establishing a causal link between vitamin D and lung cancer development/ survival through observational studies alone is exceptionally challenging. To address this, larger-scale randomized controlled trials with substantially increased sample sizes conducted within multicenter collaborative frameworks are necessary.
Furthermore, the assessment of vitamin D levels in different studies is extremely inconsistent. Namely, serum concentration of vitamin D is the main indicator of vitamin D status, but, in this review, only three studies determined serum vitamin D levels (Akiba, Weinstein, Zhu). Other studies estimated the vitamin D intake with the assistance of food questionnaires, which is a considerably less objective method for assessing the baseline amount of vitamin D in the body, and, although most questionnaires were filled out under the guidance of an interviewer, there is still a relatively high possibility of bias in this area. Consequently, future studies should rely more on the measurement of vitamin D in the blood.
It should be noted that, initially, assessing vitamin D status by measuring serum vitamin D concentrations was complex due to the substantial variability of the available assays used by different laboratories. This could result in falsely high or falsely low findings, depending on the type of assay [30]. Thus, procedures for standardizing the laboratory measurement of vitamin D have been determined through the International Vitamin D Standardization Program [31].
In addition, the heterogeneity in vitamin D supplementation protocols across different trials represents a critical consideration. For instance, the investigations included in this review employed varied supplementation approaches, with daily doses ranging from 400 to 1200 IU. In 2011, the National Academy of Medicine (NAM) released guidelines on the dietary requirements for calcium and vitamin D stating the Recommended Dietary Allowance (RDA) for vitamin D to be 600 international units (15 mcg) daily for adults up to age 70 years, increasing to 800 international units (20 mcg) daily for individuals aged 71 years and older, but these dietary intake recommendations were established based on vitamin D’s positive effects on bone health rather than its potential role in cancer prevention [32].
Consequently, standardized guidelines establishing optimal vitamin D supplementation dosages and protocols for oncological disease prevention and treatment are necessary. Additional investigation in this area is clearly essential.
Importantly, while several studies incorporated patients with different cancer types simultaneously into their analyses, few focused on addressing lung cancer patients separately. Since different cancer types possess different tumor biologies, addressing this gap in future research might yield more conclusive results.
Conclusion
In conclusion, while a considerable body of research has documented the potential role of vitamin D in enhancing survival outcomes and decreasing the risk of developing lung cancer, the existing literature presents conflicting and inconsistent results. The accumulated evidence base remains inadequate and does not provide sufficient justification for recommending routine vitamin D supplementation as a preventive measure against lung cancer development or as a therapeutic intervention to improve survival rates among patients diagnosed with non-small-cell lung cancer (NSCLC). Moving forward, there is a critical need for additional high-quality research, particularly large-scale randomized controlled trials with substantially larger sample sizes and rigorous methodological designs. Such studies are essential to comprehensively assess and definitively establish the nature and extent of the relationship between vitamin D status and various aspects of lung cancer, including both incidence and prognosis.
Conflicts of Interest: All authors have nothing to disclose.
Author’s Contributions: Conceptualization, A.R. and J.L.; methodology, A.R., G. P. and A. B.; software, A.R. and I.M.; formal analysis, A.R., G. P. and A. B.; investigation, A.R.; data curation, A.R., P.S. and I.M.; writing—original draft preparation, A.R., G. P. and A. B.; writing—review and editing, A.R., G. P. and A. B.; visualization, A.R.; supervision, J.L. and A. B.; project administration, E.A. All authors have read and agreed to the published version of the manuscript.
Funding: This research received no external funding.
Artificial Intelligence (AI) Disclosure: No artificial intelligence (AI) tools, including large language models or machine learning software, were used in the preparation, analysis, or presentation of this manuscript.
SUPPLEMENTARY MATERIAL
|
Author(s) and Year |
Study Title |
Reason for Exclusion |
|
Nakagawa et al., 2005 |
1 alpha,25-Dihydroxyvitamin D(3) is a preventive factor in the metastasis of lung cancer |
animal model study |
|
Liu et al., 2020 |
Inhibition of lung cancer by vitamin D depends on downregulation of histidine-rich calcium-binding protein |
animal model study |
|
Schömann et al., 2024 |
Umbrella Review on the Relationship between Vitamin D Levels and Cancer |
non-original article, narrative review |
|
Peterlik et al., 2009 |
Calcium, vitamin D and cancer |
non-original article, narrative review |
|
Jolliffe et al., 2019 |
Vitamin D to prevent exacerbations of COPD: systematic review and meta-analysis of individual participant data from randomised controlled trials |
benign lung disease only, no malignancy, review |
|
Kokturk et al., 2018 |
Vitamin D deficiency: What does it mean for chronic obstructive pulmonary disease (COPD)? a compherensive review for pulmonologists |
benign lung disease only, no malignancy, review |
|
Gold et al., 2025 |
Vitamin D Supplementation, Chronic Obstructive Lung Disease and Asthma Exacerbations, and Lung Function Decline |
benign lung disease only, no malignancy |
|
Henn et al., 2022 |
Vitamin D in Cancer Prevention: Gaps in Current Knowledge and Room for Hope |
general data on vitamin D and cancer |
|
Thomson et al., 2024 |
Long-Term Effect of Randomization to Calcium and Vitamin D Supplementation on Health in Older Women |
not related to lung cancer |
|
Fu et al., 2014 |
Polymorphisms in the vitamin D receptor gene and the lung cancer risk |
mechanistic study, no survival or incidence data |
|
Gheliji et al., 2022 |
Evaluation of expression of vitamin D receptor related lncRNAs in lung cancer |
mechanistic study, no clinical outcomes |
|
Wannamethee et al., 2021 |
Vitamin D deficiency, impaired lung function and total and respiratory mortality in a cohort of older men: cross-sectional and prospective findings from The British Regional Heart Study |
no cancer diagnosis or outcomes |
|
Virtanen et al., 2022 |
Vitamin D supplementation and prevention of cardiovascular disease and cancer in the Finnish Vitamin D Trial: a randomized controlled trial |
mixed data for cardiovascular disesases and cancer |
|
Harvie et al., 2014 |
Nutritional supplements and cancer: potential benefits and proven harms |
Vitamin D data not separately analyzed |
|
Kratzer et al., 2020 |
Vitamin D binding protein and risk of renal cell carcinoma in the prostate, lung, colorectal and ovarian cancer screening trial |
focused on bidning protein, not 25(OH)D levels |
|
Prakash et al., 2023 |
Calcitriol induced hypercalcemia - a rare phenomenon in lung cancer: A case report |
case report, insufficient sample size |
|
Stolzenberg et al., 2009 |
Serum vitamin D and risk of pancreatic cancer in the prostate, lung, colorectal, and ovarian screening trial |
focus on pancreatic cancer, unclear data regarding lung cancer: |
|
Zhang et al., 2013 |
Differential response to 1α,25-dihydroxyvitamin D3 (1α,25(OH)2D3) in non-small cell lung cancer cells with distinct oncogene mutations |
in vitro study, no human objects |
|
Cusato et al., 2019 |
Influence of Vitamin D in Advanced Non-Small Cell Lung Cancer Patients Treated with Nivolumab |
focus on nivolumab concentrations, no survival outcomes |
|
Polański et al., 2021 |
Relationship between Nutritional Status and Clinical Outcome in Patients Treated for Lung Cancer |
general consideration on nutritional status, vitamin D not isolated |
|
Cai et al., 2022 |
The Progress of the Prevention and Treatment of Vitamin D to Tuberculosis |
tuberculosis, no malignancy |
|
Sun et al., 2018 |
Serum 25-hydroxyvitamin D levels and risk of lung cancer and histologic types: a Mendelian randomisation analysis of the HUNT study |
genetic study, no direct vitamin D measurement |
|
Segal et al., 2012 |
Vitamin D deficiency in oncology patients--an ignored condition: impact on hypocalcemia and quality of life |
included patients with advanced stages of oncological diseases who already had bone metastasis |
|
Hu et al., 2017 |
Vitamin D3-vitamin D receptor axis suppresses pulmonary emphysema by maintaining alveolar macrophage homeostasis and function |
benign disease, imunological endpoints, no survival data |
|
Torres et al., 2024 |
Dietary Interventions for Cancer Pre vention: An Update to ACS International Guidelines. Nutrients |
clinical guidelines, not original research |
|
Note: The inclusion criteria were as follows: (1) studies on human populations, (2) randomized controlled trials (RCTs), and cohort or casecontrol studies. The exclusion criteria comprised: (1) non-original articles, (2) studies with inadequate reporting of vitamin D supplementation data or survival/mortality outcomes, (3) studies conducted on animals, (4) benign diseases. The search strategy (Prisma flowchart) and full eligibility criteria are detailed in the Methods section of the main manuscript. Total studies screened: 526 Studies included in final analysis: 7 |
||
Supplementary Table 1: Excluded Studies and Reasons for Exclusion
Purpose: This table documents studies identified during the systematic literature search that were subsequently excluded (n=25) from the final analysis. Studies were excluded based on pre-defined eligibility criteria established in the methodology section of the main manuscript.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, et al. (2021) Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71: 209-249.
- Wimalawansa SJ (2024) Physiology of Vitamin D-Focusing on Disease Prevention. Nutrients 16.
- Delrue C, Speeckaert MM (2023) Vitamin D and Vitamin D Binding Protein in Health and Disease 2.0. Int J Mol Sci 24.
- Benedik E (2022) Sources of vitamin D for humans. Int J Vitam Nutr Res 92: 118-125.
- Tran V, Janda M, Lucas RM, McLeod DSA, Thompson BS, et al. (2023) Vitamin D and Sun Exposure: A Community Survey in Australia. Curr Oncol 30: 2465-2481.
- Saponaro F, Saba A, Zucchi R (2020) An Update on Vitamin D Metabolism. Int J Mol Sci 21.
- Alonso N, Zelzer S, Eibinger G, Herrmann M (2023) Vitamin D Metabolites: Analytical Challenges and Clinical Relevance. Calcif Tissue Int 112: 158-177.
- Deeb KK, Trump DL, Johnson CS (2007) Vitamin D signalling pathways in cancer: potential for anticancer therapeutics. Nat Rev Cancer 7: 684-700.
- Krishnan AV, Feldman D (2011) Mechanisms of the anti-cancer and anti-inflammatory actions of vitamin D. Annu Rev Pharmacol Toxicol 51: 311-36.
- Nakagawa K, Kawaura A, Kato S, Takeda E, Okano T (2005)1 alpha,25Dihydroxyvitamin D (3) is a preventive factor in the metastasis of lung cancer. Carcinogenesis 26: 429-40.
- Choi YS, Shim YM, Kim SH, Son DS, Lee HS, et al. (2003) Prognostic significance of E-cadherin and beta-catenin in resected stage I nonsmall cell lung cancer. Eur J Cardiothorac Surg 24: 441-449.
- Serres MP, Zlotek-Zlotkiewicz E, Concha C, Gurian-West M, Daburon V, et al. (2011) Cytoplasmic p27 is oncogenic and cooperates with Ras both in vivo and in vitro. Oncogene 30: 2846-2858.
- Ekmekcioglu C, Haluza D, Kundi M (2017) 25-Hydroxyvitamin D Status and Risk for Colorectal Cancer and Type 2 Diabetes Mellitus: A Systematic Review and Meta-Analysis of Epidemiological Studies. Int J Environ Res Public Health 14:127.
- McCullough ML, Zoltick ES, Weinstein SJ, Fedirko V, Wang M, et al. (2019) Circulating Vitamin D and Colorectal Cancer Risk: An International Pooling Project of 17 Cohorts. J Natl Cancer Inst 111: 158-169.
- Wactawski-Wende J, Kotchen JM, Anderson GL, Assaf AR, Brunner RL, et al. (2006) Calcium plus vitamin D supplementation and the risk of colorectal cancer. N Engl J Med 354: 684-696.
- Xu Y, Shao X, Yao Y, Xu L, Chang L, et al. (2014) Positive association between circulating 25-hydroxyvitamin D levels and prostate cancer risk: new findings from an updated meta-analysis. J Cancer Res Clin Oncol 140: 1465-1477.
- Petrou S, Mamais I, Lavranos G, I PT, Chrysostomou S (2018) Effect of Vitamin D Supplementation in Prostate Cancer: A Systematic Review of Randomized Control Trials. Int J Vitam Nutr Res 88: 100-112.
- Hossain S, Beydoun MA, Beydoun HA, Chen X, Zonderman AB, et al. (2019) Vitamin D and breast cancer: A systematic review and metaanalysis of observational studies. Clin Nutr ESPEN 30: 170-184.
- Kim Y, Je Y (2014) Vitamin D intake, blood 25(OH)D levels, and breast cancer risk or mortality: a meta-analysis. Br J Cancer 110: 2772-2784.
- Zgaga L, O’Sullivan F, Cantwell MM, Murray LJ, Thota PN, et al. (2016) Markers of Vitamin D Exposure and Esophageal Cancer Risk: A Systematic Review and Meta-analysis. Cancer Epidemiol Biomarkers Prev 25: 877-886.
- Barreto SG, Neale RE (2015) Vitamin D and pancreatic cancer. Cancer Lett 368: 1-6.
- Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, et al. (2019) RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ 366: l4898.
- Zhou W, Suk R, Liu G, Park S, Neuberg DS, et al. (2005) Vitamin D is associated with improved survival in early-stage non-small cell lung cancer patients. Cancer Epidemiol Biomarkers Prev 14: 2303-2309.
- Akiba T, Morikawa T, Odaka M, Nakada T, Kamiya N, et al. (2018) Vitamin D Supplementation and Survival of Patients with Non-small Cell Lung Cancer: A Randomized, Double-Blind, Placebo-Controlled Trial. Clin Cancer Res 24: 4089-4097.
- Weinstein SJ, Mondul AM, Layne TM, Yu K, Huang J, et al. (2022) Prediagnostic Serum Vitamin D, Vitamin D Binding Protein Isoforms, and Cancer Survival. JNCI Cancer Spectr 6: pkac019.
- Takata Y, Shu XO, Yang G, Li H, Dai Q, et al. (2013) Calcium intake and lung cancer risk among female nonsmokers: a report from the Shanghai Women’s Health Study. Cancer Epidemiol Biomarkers Prev 22: 50-57.
- Cheng TY, Lacroix AZ, Beresford SA, Goodman GE, Thornquist MD, et al. (2013) Vitamin D intake and lung cancer risk in the Women’s Health Initiative. Am J Clin Nutr 98: 1002-1011.
- Redaniel MT, Gardner MP, Martin RM, Jeffreys M (2014) The association of vitamin D supplementation with the risk of cancer in postmenopausal women. Cancer Causes Control 25: 267-271.
- Zhu K, Knuiman M, Divitini M, Hung J, Lim EM, et al. (2019) Lower serum 25-hydroxyvitamin D is associated with colorectal and breast cancer, but not overall cancer risk: a 20-year cohort study. Nutr Res 67: 100-107.
- Brooks SPJ, Sempos CT (2017) The Importance of 25-Hydroxyvitamin D Assay Standardization and the Vitamin D Standardization Program. J AOAC Int 100: 1223-1224.
- Sempos CT, Binkley N (2020) 25-Hydroxyvitamin D assay standardisation and vitamin D guidelines paralysis. Public Health Nutr 23: 1153-1164.
- Ross AC, Manson JE, Abrams SA, Aloia JF, Brannon PM, et al. (2011) The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: what clinicians need to know. J Clin Endocrinol Metab 96: 53-58.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.