Ten-Year Outcomes Following Primary Bariatric Metabolic Surgery: Weight Loss Durability, Patient-Reported Health, and Long-Term Gastrointestinal Symptoms
by John Peacey1*, Lucimay Davey1, Christine Skinner1, George Hopkins1,2
1Metabolic GI Surgery Brisbane, QLD, Australia
2St. Vincent’s Hospital Northside, QLD, Australia
*Corresponding Author: John Peacey, Metabolic GI Surgery Brisbane, QLD, Australia
Received Date: 20 February 2026
Accepted Date: 25 February 2026
Published Date: 27 February 2026
Citation: Peacey J, Davey L, Skinner C, Hopkins G (2026) Ten-Year Outcomes Following Primary Bariatric Metabolic Surgery: Weight Loss Durability, Patient-Reported Health, and Long-Term Gastrointestinal Symptoms. J Surg 11: 11576 DOI: https://doi.org/10.29011/25759760.011576
Abstract
Background: Long-term outcomes following bariatric metabolic surgery remain incompletely characterised in Australian populations, particularly patient-reported health and chronic gastrointestinal symptoms beyond 10 years.
Methods: Patients approximately 10 years following primary Sleeve Gastrectomy (SG) or Gastric Bypass (GB) were contacted for structured long-term follow-up including questionnaire completion, blood testing, and clinic review. Outcomes included Body Mass Index (BMI), percentage Total Body Weight Loss (%TBWL), patient-reported health improvement, regret, long-term gastrointestinal symptoms, and revisional surgery.
Results: Sixty-six patients participated (SG n = 44; GB n = 22); 48 were female (72%). Mean pre-operative BMI was 45.6 kg/m² (SG) and 47.8 kg/m² (GB). At 10 years, mean BMI was 34.8 kg/m² and 31.0 kg/m², respectively. Mean nadir %TBWL was 37% at 20 months following SG and 42% at 33.6 months following GB. At 10 years, mean %TBWL was 24% (SG) and 32% (GB). Overall, 80% reported improved health and 94% reported no regret. Gastrointestinal symptoms were common, and 26% underwent revisional surgery.
Conclusion: In this Australian cohort, both SG and GB provided durable long-term weight loss and high patient satisfaction at 10 years. Gastric bypass demonstrated greater weight loss durability, while chronic gastrointestinal symptoms and revisional surgery were prevalent following both procedures, emphasising the need for lifelong follow-up within the Australian healthcare system.
Keywords: Long-Term Bariatric Outcomes; Metabolic Bariatric Surgery; Roux-En-Y Gastric Bypass; Sleeve Gastrectomy
Introduction
Obesity represents one of the most significant public health challenges facing Australia. Current national data indicate that over two-thirds of Australian adults are overweight or obese, with approximately one-third meeting criteria for obesity. The prevalence of obesity-related comorbidities including type 2 diabetes mellitus, cardiovascular disease, obstructive sleep apnoea, non-alcoholic fatty liver disease, and musculoskeletal disease continues to rise, contributing substantially to healthcare expenditure and reduced quality of life. The chronic and relapsing nature of obesity necessitates durable, long-term treatment strategies. Bariatric metabolic surgery remains the most effective intervention for achieving substantial and sustained weight loss in individuals with severe obesity. Large observational studies and randomised trials have demonstrated durable weight loss, improvement or remission of metabolic disease, and reductions in long-term mortality following bariatric surgery when compared with non-surgical management [1-3]. Consequently, bariatric surgery is increasingly recognised as a key component of chronic disease management rather than a purely elective intervention. While short- and medium-term outcomes are well established, long-term data beyond 10 years remain limited, particularly from Australian centres. This is clinically important, as weight regain, gastrointestinal sequelae, nutritional deficiencies, and the need for revisional surgery often emerge several years after the index procedure. Long-term outcomes also directly influence healthcare utilisation, particularly in a publicly funded system such as Australia’s, where access to specialist follow-up may vary by geography. Sleeve Gastrectomy (SG) and Gastric Bypass (GB) are the most commonly performed bariatric procedures in Australia. Over the past decade, SG has become the dominant primary procedure due to technical simplicity, shorter operative time, and perceived lower peri-operative risk. However, accumulating international evidence suggests that SG and GB may diverge in long-term outcomes, particularly with respect to weight loss durability and Gastro-Oesophageal Reflux Disease (GORD) [4-8]. Australian-specific long-term data are required given differences in population demographics, healthcare access, follow-up models, and geographic distribution, particularly for patients living in regional and remote areas. Patient-reported outcomes such as perceived health improvement and regret are also increasingly recognised as critical measures of success but remain under-reported in long-term bariatric literature. This study aimed to evaluate 10-year outcomes following primary SG and GB in an Australian cohort, focusing on weight loss durability, patient-reported health improvement and regret, long-term gastrointestinal symptoms, and revisional surgery rates.
Methods
Study Design and Setting
This was a retrospective cohort study with prospective long-term follow-up conducted at an Australian tertiary bariatric surgery centre. Institutional ethics approval was obtained prior to commencement.
Participants
Patients who underwent primary laparoscopic sleeve gastrectomy or gastric bypass were identified from institutional bariatric databases. Eligible patients were contacted at approximately 10 years following their index procedure and invited to participate in structured long-term follow-up. Patients were included irrespective of whether they had required revisional surgery, reflecting real-world long-term outcomes.
Follow-Up Assessment
Participants completed a structured questionnaire assessing selfreported health status, gastrointestinal symptoms, and regret related to surgery. Clinical review and blood testing were performed in accordance with routine long-term bariatric follow-up protocols. Follow-up was conducted through a combination of in-person review and telehealth, reflecting contemporary Australian practice.
Data Collection
Collected variables included sex, procedure type, pre-operative
BMI, nadir BMI, time to nadir weight, BMI at 10 years, nadir %TBWL, %TBWL at 10 years, patient-reported improvement in health, regret regarding surgery, long-term gastrointestinal symptoms (reflux, bowel dysfunction, abdominal pain), and revisional surgery following the index procedure.
Outcomes
Primary outcomes were BMI and %TBWL at 10 years. Secondary outcomes included nadir %TBWL, patient-reported health improvement, regret, long-term gastrointestinal symptoms, and revisional surgery.
Statistical Analysis
Given the exploratory nature of long-term follow-up and modest sample size, analyses were descriptive. Continuous variables are presented as means, and categorical variables as frequencies and percentages.
Results
Patient Characteristics
Sixty-six patients participated, including 44 who underwent SG and 22 who underwent GB. The cohort comprised 48 females (72%) and 18 males (27%), reflecting the female predominance commonly observed in bariatric surgery populations.
Weight Loss Outcomes
Mean pre-operative BMI was 45.6 kg/m² in the SG group and 47.8 kg/m² in the GB group. At 10 years, mean BMI was 34.8 kg/m² for SG and 31.0 kg/m² for GB. Mean nadir %TBWL was 37% at a mean of 48 months following SG and 42% at 33.6 months following GB. At 10 years, mean %TBWL was 24% in the SG group and 32% in the GB group, indicating greater long-term weight loss durability following GB. The weight-loss outcomes are displayed in Figure 1.
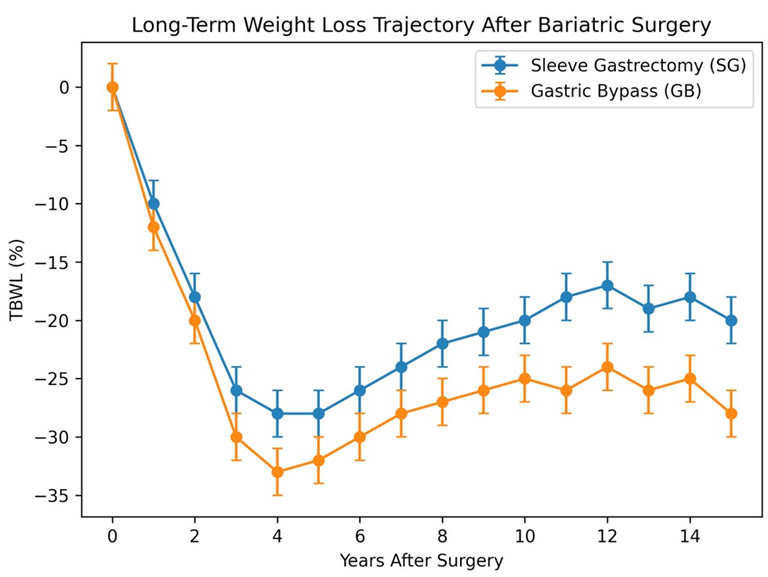
Figure 1: Long-Term Weight Loss Trajectory Following Sleeve Gastrectomy and Gastric Bypass Mean percentage Total Body Weight Loss (TBWL) over time following primary Sleeve Gastrectomy (SG) and Gastric Bypass (GB). Gastric bypass demonstrates greater nadir weight loss and superior long-term durability compared with sleeve gastrectomy. Error bars represent variability within each surgi- cal group.
Patient-Reported Outcomes
At 10 years, 80% of participants reported improved health compared with their pre-operative state. Regret was uncommon, with 94% reporting no regret regarding their bariatric procedure.
Long-Term Gastrointestinal Symptoms
Chronic gastrointestinal symptoms were prevalent in both groups. In the SG group, 52% reported bowel dysfunction, 58% reported reflux, and 26% reported abdominal pain. Among those reporting reflux following SG, 96% required ongoing proton pump inhibitor therapy. In the GB group, 62% reported bowel dysfunction, 24% reported reflux, and 23% reported abdominal pain.
Revisional Surgery
The rate of revisional surgery was 26% (n=17). In the SG group, 7 patients were converted to GB for reflux and 1 patient underwent re-sleeve for weight regain. In the GB group, 6 underwent endoscopic dilatation of the gastrojejunostomy. Other operations in the GB group included fixed ring placement (n=1), division of adhesions (n=3), internal hernia repair (n=1) and bypass reversal (n=1). The weight long-term weight outcomes and symptoms of the cohort are displayed in Figure 2.
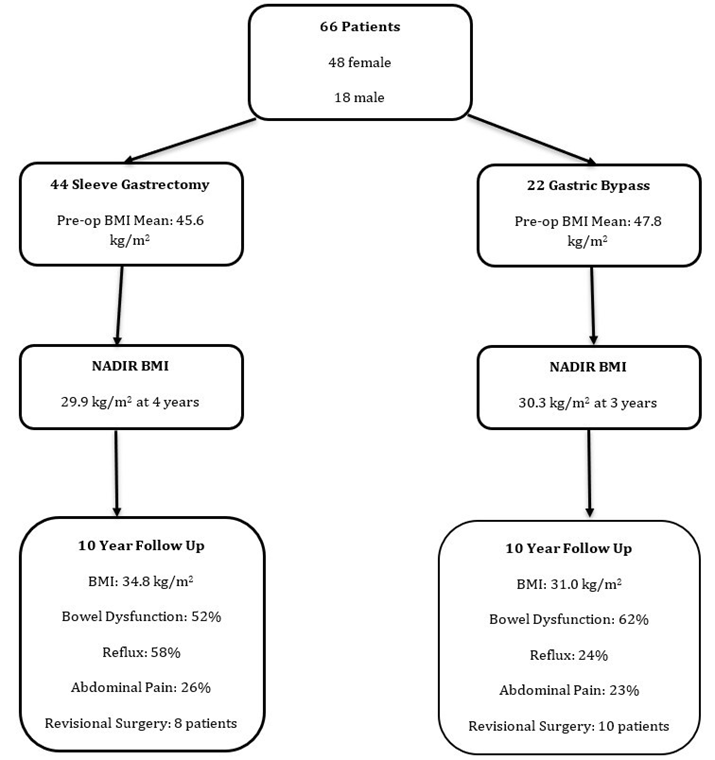
Figure 2: Overall flowchart of long-term weight outcomes and symptoms of cohort of patients with 10 years follow up post metabolic bariatric surgery.
Discussion
This study provides long-term Australian data at 10 years following primary bariatric metabolic surgery, demonstrating durable weight loss and high patient satisfaction after both Sleeve Gastrectomy (SG) and Gastric Bypass (GB). Importantly, gastric bypass was associated with greater long-term weight loss durability, while chronic gastrointestinal symptoms and revisional surgery were common following both procedures. These findings reinforce the concept of bariatric surgery as a lifelong intervention requiring sustained follow-up within the Australian healthcare system.
Long-Term Weight Loss Durability
Weight loss durability remains one of the most critical determinants of success following bariatric surgery. In the present cohort, both SG and GB achieved substantial early weight loss, with clinically meaningful reductions in BMI and %TBWL maintained at 10 years. However, greater attenuation of weight loss over time was observed following SG compared with GB, consistent with international long-term data [6,9,10]. Multiple long-term cohort studies and randomised trials have demonstrated superior weight loss maintenance following gastric bypass beyond five to ten years [6,11,10]. While SG often achieves comparable early outcomes, progressive weight regain has been reported during the latter half of the postoperative decade [9,12]. The divergence in long-term trajectories observed in this Australian cohort aligns with these findings and highlights the importance of long-term follow-up when evaluating procedural efficacy. Several physiological mechanisms may underpin the superior durability observed following GB. Gastric bypass induces sustained alterations in gut hormone secretion, including glucagon-like peptide-1 and peptide YY, which enhance satiety and improve glycaemic control [13]. In addition, changes in bile acid metabolism and intestinal nutrient sensing may exert prolonged metabolic effects that attenuate weight regain [13,14]. In contrast, SG relies predominantly on restrictive mechanisms and early hormonal changes, which may diminish over time as gastric compliance increases and behavioural adaptation occurs. From an Australian perspective, weight loss durability is particularly relevant given variability in access to multidisciplinary bariatric follow-up. Patients living in regional and remote areas may have limited access to dietetic, psychological, and exercise physiology services. Procedures with greater inherent metabolic durability may therefore offer advantages in settings where long-term support is inconsistent.
Patient-Reported Health and Regret
A notable finding of this study is the high level of patient-reported health improvement and low regret at 10 years, despite weight regain, chronic symptoms, and revisional surgery. Eighty per cent of participants reported improved health compared with their preoperative state, and regret was uncommon. These findings are consistent with previous studies demonstrating that patient-perceived benefit extends beyond absolute weight loss and includes improvements in functional capacity, mobility, self-esteem, and social participation [15,16]. Patients may also value the prevention or mitigation of obesity-related comorbidities, which were not directly quantified in this study but are known to significantly influence quality of life. Low regret rates suggest that patients contextualise long-term outcomes holistically rather than focusing solely on complications or weight regain. This has important implications for pre-operative counselling in Australia, supporting transparent discussions regarding long-term risks while reinforcing that overall satisfaction remains high for most patients. Incorporating patient-reported outcomes into routine long-term follow-up may therefore provide a more comprehensive assessment of surgical success than weight metrics alone.
Gastro-Oesophageal Reflux Disease
Gastro-Oesophageal Reflux Disease (GORD) emerged as a major long-term issue following SG in this cohort, with more than half of SG patients reporting reflux symptoms and the majority requiring ongoing proton pump inhibitor therapy. In contrast, reflux prevalence was substantially lower following GB. These findings are consistent with a growing body of international literature linking SG to de novo or worsened GORD [17-19]. Proposed mechanisms include altered gastric anatomy, increased intragastric pressure, disruption of the angle of His, and impaired lower oesophageal sphincter function. Over time, progressive dilation of the gastric sleeve may further exacerbate reflux symptoms. From an Australian healthcare perspective, chronic GORD has important implications for quality of life and healthcare utilisation. Access to endoscopy and specialist gastroenterology services may be limited in regional and remote settings, potentially delaying diagnosis and management of complications such as oesophagitis or Barrett’s oesophagus. These findings support careful patient selection and counselling, particularly in individuals with pre-existing reflux, oesophageal dysmotility, or hiatus hernia, where gastric bypass may offer superior long-term symptom control [20].
Bowel Dysfunction and Chronic Abdominal Pain
Bowel dysfunction was prevalent in both procedure groups, affecting more than half of patients at 10 years. Symptoms included altered bowel habit, urgency, and diarrhoea. The aetiology of bowel dysfunction following bariatric surgery is multifactorial and may include altered gut motility, bile acid malabsorption, dietary intolerance, and changes in the gut microbiome [13,14,21]. Chronic abdominal pain was reported by approximately one-quarter of patients in both groups. Potential causes include functional gastrointestinal disorders, adhesions, marginal ulcers, internal hernias, and altered visceral sensitivity [22,23]. Chronic pain can significantly impair quality of life and often leads to repeated investigations and healthcare encounters, underscoring the importance of a multidisciplinary approach to long-term bariatric care. These findings highlight the need for structured symptom assessment during longterm follow-up. In Australian practice, long-term bariatric care is often fragmented, particularly for patients outside metropolitan centres. Improved integration between surgical, medical, and primary care services may facilitate earlier identification and management of chronic gastrointestinal symptoms.
Revisional Surgery and the Chronic Disease Model
The revisional surgery rate of 26% observed in this cohort reflects the chronic and progressive nature of obesity and bariatric disease. Conversion from SG to GB was the most common revisional strategy, typically undertaken for refractory reflux or inadequate weight loss. International studies report similar long-term revisional surgery rates, particularly following SG [7,12,24-26]. As SG has become the dominant primary bariatric procedure in Australia, demand for revisional bariatric surgery is likely to increase over time. Revisional surgery is technically more complex, associated with higher morbidity, and requires specialised expertise, with implications for surgical training and workforce planning. These findings support conceptualising bariatric surgery as part of a chronic disease management model rather than a one-time intervention. Lifelong follow-up, early identification of suboptimal outcomes, and timely intervention may reduce the need for late revisional surgery and improve long-term outcomes.
Strengths and Limitations
The strengths of this study include long-term follow-up at 10 years and the integration of patient-reported outcomes with objective weight metrics. Such data remain scarce in Australian bariatric literature and provide clinically relevant insights into long-term outcomes. Limitations include the modest sample size, retrospective design, and reliance on self-reported symptoms, which may be subject to recall bias. Formal comparative statistical analyses were not performed due to limited power. Additionally, detailed data on comorbidity remission and validated quality-of-life instruments were not available. Despite these limitations, the findings provide valuable real-world insights into long-term outcomes following bariatric surgery in an Australian context.
Conclusion
In an Australian cohort, both sleeve gastrectomy and gastric bypass provided durable long-term weight loss and high patient satisfaction at 10 years. Gastric bypass demonstrated superior weight loss durability, while chronic gastrointestinal symptoms and revisional surgery were common following both procedures. These findings support informed procedure selection and emphasise the importance of lifelong follow-up within the Australian healthcare system.
References
- Australian Institute of Health and Welfare (2023) Overweight and obesity among Australian adults. Canberra: AIHW.
- Sjöström L (2013) Review of the key results from the Swedish Obese Subjects (SOS) trial a prospective controlled intervention study of bariatric surgery. J Intern Med 273: 219-234.
- Adams TD, Gress RE, Smith SC, Halverson RC, Simper SC, et al. (2007) Long-term mortality after gastric bypass surgery. N Engl J Med 357: 753-761.
- Arterburn DE, Olsen MK, Smith VA, Livingston EH, Van Scoyoc L, et al. (2015) Association between bariatric surgery and long-term survival. JAMA 313: 62-70.
- Courcoulas AP, King WC, Belle SH, Berk P, Flum DR, et al. (2018) Seven-year weight trajectories and health outcomes in the Longitudinal Assessment of Bariatric Surgery (LABS) study. JAMA Surg 153: 427-434.
- Peterli R, Wölnerhanssen BK, Peters T, Vetter D, Kröll D, et al. (2018) Effect of laparoscopic sleeve gastrectomy vs Roux-en-Y gastric bypass on weight loss in patients with morbid obesity: the SM-BOSS randomized clinical trial. JAMA 319: 255-265.
- Oor JE, Roks DJ, Ünlü Ç, Hazebroek EJ (2016) Laparoscopic sleeve gastrectomy and gastroesophageal reflux disease: a systematic review and meta-analysis. Am J Surg 211: 250-267.
- Angrisani L, Santonicola A, Iovino P, Ramos A, Shikora S, et al. (2021) Bariatric surgery worldwide 2018. Obes Surg 31: 1345-1352.
- Thereaux J, Czernichow S, Corigliano N, Poitou C, Oppert JM, et al. (2019) Five-year outcomes of gastric bypass versus sleeve gastrectomy: results from a multicenter prospective cohort study. Ann Surg 269: 110-118.
- King WC, Hinerman AS, Belle SH, Wahed AS (2020) Comparison of the performance of common measures of weight regain after bariatric surgery for association with clinical outcomes. Obesity 28: 113-123.
- Peterli R, Borbély Y, Kern B, Gass M, Peters T, et al. (2024) Ten-year outcomes of sleeve gastrectomy versus Roux-en-Y gastric bypass: a multicentre randomised trial. Lancet 403: 123-134.
- Clapp B, Harper B, Dodoo C, Klingsporn W, Barrientes A, et al. (2020) Revisional bariatric surgery trends in the United States. Obes Surg 30: 420-427.
- le Roux CW, Heneghan HM (2018) Bariatric surgery for obesity. Med Clin North Am 102: 165-182.
- Aron-Wisnewsky J, Clément K (2016) The gut microbiome, diet, and links to cardiometabolic and chronic disorders. Nat Rev Nephrol 12: 169-181.
- Kolotkin RL, Davidson LE, Crosby RD, Hunt SC, Adams TD (2018) Six-year changes in health-related quality of life in gastric bypass patients versus obese comparison groups. Obes Surg 28: 1359-1367.
- van Hout GCM, Verschure SKM, van Heck GL (2009) Psychosocial predictors of success following bariatric surgery. Obes Surg 19: 701707.
- Yeung KTD, Penney N, Ashrafian H, Darzi A, Purkayastha S (2020) Does sleeve gastrectomy expose the distal esophagus to severe reflux? A systematic review and meta-analysis. Ann Surg 271: 257-265.
- Sebastianelli L, Benois M, Vanbiervliet G, Bailly L, Robert M, et al. (2019) Systematic endoscopy after sleeve gastrectomy: incidence of esophagitis, Barrett’s esophagus, and reflux symptoms. Surg Obes Relat Dis 15: 1406-1414.
- Stefanidis D, Kuwada TS, Gersin KS (2010) The effect of bariatric surgery on gastroesophageal reflux disease. Surg Obes Relat Dis 6: 474-479.
- Soricelli E, Casella G, Rizzello M, Abbatini F, Alessandri G, et al. (2006) Initial experience with sleeve gastrectomy as a stand-alone procedure for morbid obesity. Obes Surg 16: 664-670.
- Camilleri M (2015) Bile acid diarrhea: prevalence, pathogenesis, and therapy. Gut 64: 1651-1664.
- Carrodeguas L, Szomstein S, Soto F, Whipple O, Simpfendorfer C, et al. (2005) Management of abdominal pain after Roux-en-Y gastric bypass surgery. Surg Obes Relat Dis 1: 404-408.
- Higa KD, Ho T, Tercero F, Yunus T, Boone KB (2003) Internal hernias after laparoscopic Roux-en-Y gastric bypass: incidence, treatment and prevention. Obes Surg 13: 350-354.
- Gagner M, Milone L, Yung E, Broseus A, Gumbs A (2013) Causes of weight regain after sleeve gastrectomy. Surg Obes Relat Dis 9: 123128.
- Lynch J, Belgaumkar A, Cochrane L, Miras AD, Vincent RP, et al. (2020) Long-term outcomes after bariatric surgery: a systematic review. Obes Surg 30: 444-453.
- Mahawar KK, Jennings N, Brown J, Gupta A, Balupuri S (2013) “Mini” gastric bypass: systematic review of a controversial procedure. Obes Surg 23: 1890-1898.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.