Teaching Individuals with Developmental Disabilities Basic Cooking Skills: A Single Case Research
Christina S Lappa1*,Constantinos N Mantzikos2
1 University of Thessaly, Volos, and Hellenic Open University, Patra, Greece. ORCID ID: https://orcid.org/0000-0002-3960-2450
2 Special Education Teacher, 57th Kindergarten of Piraeus, Attica, Greece. ORCID ID: https://orcid.org/0000-0003-1698-5767
*Corresponding author: Christina S Lappa, University of Thessaly, Volos and Hellenic Open University, Patra, Greece. Email: xlap@uth.gr
Received Date: 12 February 2023
Accepted Date: 01 March 2023
Published Date: 13 March 2023
Citation: Lappa CS, Mantzikos CN (2023) Teaching Individuals with Developmental Disabilities Basic Cooking Skills: A Single Case Research. Int J Autism & Relat Disabil 5: 164. DOI: https://doi.org/10.29011/2642-3227.100064
Abstract
Seven adults between the ages 27 and 65 with Developmental Disabilities (DD) (Intellectual Disability-ID, Down syndrome- DS, Autism Spectrum Disorder-ASD-with ID) were selected to be taught basic cooking skills, such as material identification, measuring, mixing, and sequencing when making bread. The purpose of this qualitative study is to investigate the efficacy of an intervention program that combined a natural pattern, a visual recipe, a task analysis, modeling, indication, feedback and reinforcement as well as the ability of individuals with DD to preserve and retrieve the recipe details when visual and verbal assistance is withdrawn. A quasi-experimental baseline design was implemented to show the acquisition of cooking skills through conditions of baseline, training and probe/evaluation. The results indicated that each participant acquired the targeted skills, and was able to complete the task independently. A social validity measure affirmed these improvements in their cooking skills. Aside from the obvious benefits of being able to cook, these skills can be an important aspect of self-sufficiency.
Keywords : Cooking skills; Developmental Disabilities; Examples of DD include ID, ASD, DS, cerebral palsy, behavioral Efficiency; Intervention program; Retrieving recipe details.
Introduction
Functional living skills are crucial for people with DD and their engagement in the community and encompass a variety of skills including social, vocational, behavior management, and academic skills [1]. Cronin [2] defined functional life skills as ‘those skills that contribute to the successful, independent functioning of an individual in adulthood’ (p. 54). These skills are broadly classified into five categories: self-care and domestic living, recreation and leisure, communication and social skills, vocational skills, and other skills necessary for community participation (e.g., postsecondary education) [3, 4]. The term “Developmental Disabilities” is a broader category of often-lifelong disability that can be intellectual, physical, or both. Examples of DD include ID, ASD, DS, cerebral palsy, behavioral difficulties, brain injury and spina bifida [5]. In this study, we focus on ID, DS, and ASD. ID is a developmental condition characterized by a decreased level of intellectual functioning and a reduced ability to adapt to daily life and social environments [6]. It is widely acknowledged that students with ID are a distinct group and that each student with ID has unique educational needs [7]. Supports, such as visual images [8, 9], innovative augmented- reality games [10], and strategies, such as video modeling and video prompting, can have positive effects on individuals with ID [11] as far as the teaching skills (e.g., daily living, employment, leisure, and academic skills) are concerned.
One of the most common genetic disorders that causes ID is DS [12, 13]. Infants with DS are the most well-studied population with ID [14], Individuals with DS have varying levels of ID, ranging from severe to limited mental function [13], with the majority having moderate to severe ID [15]. Individuals with DS learn in a different way throughout their lives. Usually, their performance improves when they receive feedback [16], choose individualized teaching [17] or when visual information is provided [18, 19]. Strategies, such as project analysis, routine practice, and learning motivation, provide the individual with many opportunities to generalize learning concepts and behaviors [20]. When the teacher’s instructions are clear and understandable, the behavior to be demonstrated during the course of learning becomes clearer [21]. Good approaches include play, systematic instruction, repetition of concepts and abilities, automation [22], and the use of visuals [23].
ASD is a group of lifelong neurodevelopmental conditions that affect one out of every 100 children worldwide [24]. Individuals with ASD have various difficulties in social functioning, such as stereotypical gestures, difficulty with eye contact, limited emotional and social reciprocity, and inability to comprehend facial expressions and body language; additionally, aggressive behavior is not uncommon [5]. Co-occurring conditions in children on the autism spectrum include anxiety disorders, ID, and attention deficit hyperactivity disorder (ADHD) [25]. Learners with ASD and ID require considerable instructional support and adaptations. Technology may assist in the learning process for persons with ASD and ID [26]. Students with ASD and ID benefit from task analysis and graphs [27] as well as Applied Behavior Analysis interventions [28].
Many people with DD have difficulties in functional living skills, such as self-care, cooking, cleaning, and managing personal finances, which limit their ability to live independently. These limitations have an impact on outcomes throughout the individual’s life span, necessitating additional support from family and agencies as they progress through their lives. Moreover, any failure to teach such skills can result in negative outcomes, such as low self-esteem, learned helplessness, and lower quality of life [29].
Meal preparation or cooking has been identified as an especially important skill for independent daily living [30, 31, 32]. According to some researchers, there is no clear and consistent definition of cooking skills [33, 34]. However, Hartmann et al. [35] argue that cooking skills are ‘the ability to prepare different foods’ (p. 129), whereas Stead et al. [36] argue that cooking includes other aspects, such as meal planning and budgeting, in addition to the meal preparation. Fordyce-Voorham [37] even uses the term ‘cooking skills’ not only for meal preparation but also for meal planning. Cooking can give individuals valuable exposure to a range of academic and functional skills, including choice-making, self-determination, and other abilities necessary for independent living. These skills include reading, budgeting, shopping and food purchasing, item identification, measurement, and sequencing [31, 38]. Aside from the obvious advantages of being able to prepare one’s own meals, this skill can be an important aspect of selfsufficiency, because food service jobs were the most common work-study jobs for secondary students with disabilities [39]. Thus, the emphasis of the curriculum for students with DD should be on functional and practical skills, resulting in the greatest possible levels of independence and self-reliance.
Researchers, educators, and healthcare professionals continue to face a crucial challenge in identifying effective educational programs designed to help people with DD acquire functional living skills. Society has been investigating efficient and effective training programs for individuals with DD. With regard to teaching autonomous completion of multistep tasks to individuals with disabilities, video modeling has been proven to be particularly effective [31, 40-43], especially in regard to food preparation skills [44-47]. Video prompting, on the other hand, is an instructional method that involves showing each step in a skill sequence on video, followed by task engagement with that specific step [48], and leads to the acquisition and maintenance of various independent living skills [49, 50]. Video-based instruction is an effective instructional technology that has been linked to improvements in a variety of skills, including cognitive ability, social skills and communication, and academic, daily living, and vocational skills [29]. Furthermore, it provides participants with an appropriate model as well as a set of behaviors or skills and enables them to observe and concentrate on the desired behaviors/ skills.
Photographs and line drawings are two of the most commonly used visual supports [51, 52]. Photographs or illustrated pictures are relatively simple to make and are frequently used to teach or prompt people with ASD or other DD to complete complex or multistep skill sequences. Photographed and/or illustrated task analyses, for example, have been used successfully to teach food preparation skills [53, 54], vocational skills [55], daily living skills [56], and community skills [57, 58]. Several strategies (prompting, modeling, reinforcement, shaping, and chaining) and interventions (video modeling, behavioral in vivo procedures, visual cues and audio cueing) have been shown to be effective in teaching daily living skills to people with ASD [59].
Therefore, comprehensive, extensive, and effective programs are needed to develop all the skills required in adult life [60, 61]. The purpose of this study was to investigate, whether an individual with DD could learn essential cooking skills like item identification, measuring, mixing, and sequencing when making bread in the context of an intervention program, and whether it was possible to preserve and retrieve the recipe details when visual and verbal assistance was withdrawn. In an effort to determine the efficacy of the intervention for achieving this purpose, we propose the following research questions:
1. Does an intervention cooking program improve essential skills, such as item identification, measuring, mixing and sequencing, in individuals with DD?
2. Is an intervention cooking program an effective strategy of cooking skill acquisition for individuals with DD?
Research Methodology
Participants
Seven adults aged 27 to 65 years with ID and ADS with ID from a residential facility in the Thessaly region of Greece participated in this study. Prior to intervention, the participants’ mental capacity and functionality was assessed by the residential facility’s psychologist using the Wechsler Intelligence Scales (WISC-III). All participants had ID. Three of them had also DS, and one of them ASD. All participants were selected because they could understand what they listen to and see, follow instructions, and ask and answer short questions, in order to complete the task. Participants’ vision and hearing were within the typical range. None of them could read. There were no fine or gross motor issues among the participants.
|
NAMES |
AGES |
DIAGNOSIS |
WISC-III |
|
GEORGE |
45 |
Moderate ID |
53 |
|
ANTONIS |
33 |
Down Syndrome and Severe ID |
34 |
|
BARBARA |
41 |
Down Syndrome and Moderate ID |
53 |
|
IOULIA |
38 |
Down Syndrome and Severe ID |
35 |
|
MARINA |
61 |
Severe ID |
34 |
|
SOTIRIS |
65 |
Severe ID |
30 |
|
VICTORIA |
36 |
ASD with severe ID |
37 |
Table 1: The age and mental score of each adult.
Ethical considerations
The first author requested the permission of the director/ president of the residential facility to conduct this study. Furthermore, the names of the participants have been changed to conceal their identities.
Functional definitions
The steps were defined as:
Correct step/response to the execution of a step with indication: When a participant did not complete a step, despite having followed the natural pattern or the visual recipe, the researcher gave verbal instructions and modeled the step by showing the participant what to do.
Correct step/response to the execution of a step without indication: When a participant completed a step correctly, the researcher did not provide guidance.
Wrong step/response to the execution of a step: A step of the task analysis was not completed correctly by the participant.
Procedure
Each training session was held in a quiet room with a table. A video camera was set up on a tripod in one corner of the room. The participants entered the room and were standing around the table. They are required to wear aprons and wash their hands. On the table were the materials, which were seven bowls, a pot of water, flour, yeast, salt, seven cups, seven spoons, seven pans. The camera began to record and the researcher gave the prompt ‘Let’s cook bread’. Sessions during the training stage were approximately 45 minutes. During the training a researcher demonstrated how to cook bread. A task analysis procedure was used. During the first two phases, the researcher used modeling to perform a complete chain of steps by showing each material, the quantities to be used, and the way they should be used, while the participants imitated each step. When a participant did not make the step correctly, the main researcher provided guidance (indication) by giving verbal instructions and modeling the step, thus showing the participant what to do. A visual recipe with pictures of thirteen steps instead of a natural pattern was provided during the last two phases. As the participants could not read, the visual recipe with pictures was preferred. Again, when a participant did not make the step correctly, the main researcher provided guidance (indication) by giving verbal instructions and modeling the step, and showing the participant what to do. Each participant was required to complete all thirteen steps of the task analysis in the right order. The session concluded when the participants completed all thirteen steps of task analysis. The data were collected over a five-week period.
Experimental sessions
In an applied behavior analysis program, the researcher must clearly specify the behaviors to be observed so that they can be observed, assessed, and agreed upon by those evaluating the program’s performance and execution. The baseline condition refers to the rate at which the researcher evaluates the desired behavior prior to training. In other words, the measurement of the dependent variable before the start of the intervention is saved in the database. The most important goal of this type of program is to alter behavior. Behavior during the subsequent probe should be compared with the behavior in the baseline condition [62]. Such programs are frequently implemented, especially when the aim of a study is to change a behavior though training [8, 9].
In the three baseline conditions (lasting one week) the materials were on the table. The participants were informed that they would be taught to make bread. The participants were given the instruction to make bread. At this point, no aid or supportive effect was provided regarding the desired behavior. The researcher waited to see if any of the participants could cook bread. The intervention began when it became apparent that the participants’ performance was constantly zero.
The three-week training was divided into four phases (Phase 1, 2, 3 and 4). The recipe was divided into thirteen steps. Cooking was designed using the constructivism learning theory, which advocated for skill acquisition through a step-by-step process [63, 64]. During the first two phases of training (Phase 1 and 2) the researcher modeled all the steps one by one by showing each material, the quantities to be used, and the way they should be used. With modeling the researcher provided a visual example of what the participants would be expected to do [65]. The breakdown of complex or multi-step skills into smaller, easier-to-learn subtasks is known as task analysis. The steps are then sequenced in the order in which they occur naturally [66]. Tan, Hughes, and Toogood [67] demonstrated that task analysis increases children’s with DD engagement in learning processes. During the last two phases of training (Phase 3 and 4) a visual recipe (instead of a natural pattern) with thirteen steps was provided. Prompt feedback was given (verbal instructions and modeling the step in order to show the participant the exact steps that he/she should follow) in the case of an incorrect step and reinforcement offered when a correct step was supplied. Finally, a probe-evaluation took place. Table 2 indicates the thirteen steps of the recipe which the participants were taught.
|
1 |
Cup of flour is poured into the basin |
|
2 |
Add another cup of flour to the basin |
|
3 |
Measure out 0.5 teaspoon of salt and place it in the bowl |
|
4 |
In the center of the flour make a well |
|
5 |
Take one cup of lukewarm water |
|
6 |
Take 0.5 teaspoon of yeast and mix it thoroughly in a mug of water |
|
7 |
Pour carefully the yeast-infused water into the well |
|
8 |
Mix the flour with the water and knead it thoroughly |
|
9 |
If the dough is too stiff, add some water |
|
10 |
If the dough is too thin, add some flour |
|
11 |
Make a ball out of my dough |
|
12 |
Dust the pan with flour and place the ball in it |
|
13 |
Put the pan with the bread in the oven |
Table 2: The thirteen steps of the recipe that the participants were taught.
More specifically, during the first phase of training which took place during the second week (Phase 1-Natural Pattern with indication: 3 sessions), one researcher physically demonstrated the steps one by one, while the main researcher provided indication (verbal instructions and modeling the step in order to show the participant what to do) whenever the participant did not respond to the execution of a step.
In a second phase (during the third week), (Phase 2 - Natural Pattern without indication: 3 sessions) the researcher again showed the steps in order, but the main researcher did not provide indication, when the participant did not respond to the execution of a step.
In a third phase (during the fourth week), (Phase 3 - Visual recipe with indication: 1 session), the researcher illustrated the steps of the recipe so as the participants could follow them, and the main researcher provided indication (verbal instructions and modeling the step in order to show the participant what to do) whenever a participant did not respond to the execution of a step.
In the fourth phase (during the fourth week), (Phase 4 - Visual recipe without indication: 2 sessions), participants saw the recipe and followed the steps without the researcher’s indication.
Throughout the whole duration of the training, verbal praise for the steps taken correctly as well as a final reward for each participant’s good practice was awarded.
Finally, there was the probe-evaluation (during the fifth week), (Back to Base), in which the participants completed the entire process on their own without natural pattern, indication or visual recipe.
Independent and dependent variables
The independent variables in the present study were the natural pattern of the researcher, the indications, the visual recipe with pictures of the thirteen steps. The dependent variable was the number of steps/responses to the execution of a step (steps without indication, steps with indication, wrong steps) from each participant per session. The data were recorded on a video-camera, collected and ranked separately for each participant by the two researchers.
Inter-observer agreement
All of the sessions were video-recorded and scored by two researchers (the main researcher and an observer). The agreement score was calculated point by point. The number of agreements was divided by the total number of agreements and disagreements and multiplied by 100 to give a percentage. All sessions were rated, and the average agreement rate was 94%.
Results and Analysis
The intervention data are presented per participant. The X-axis shows the consecutive sessions and the Y-axis shows the independent steps for each participant. The vertical lines represent changes in conditions in the order of baseline, training (Phase 1, 2, 3 and 4) and probe.
A white circle represents a correct step/response to the execution of a step with indication. A black circle represents a wrong step/ response to the execution of a step. A black triangle represents a correct step/response to the execution of a step without indication.
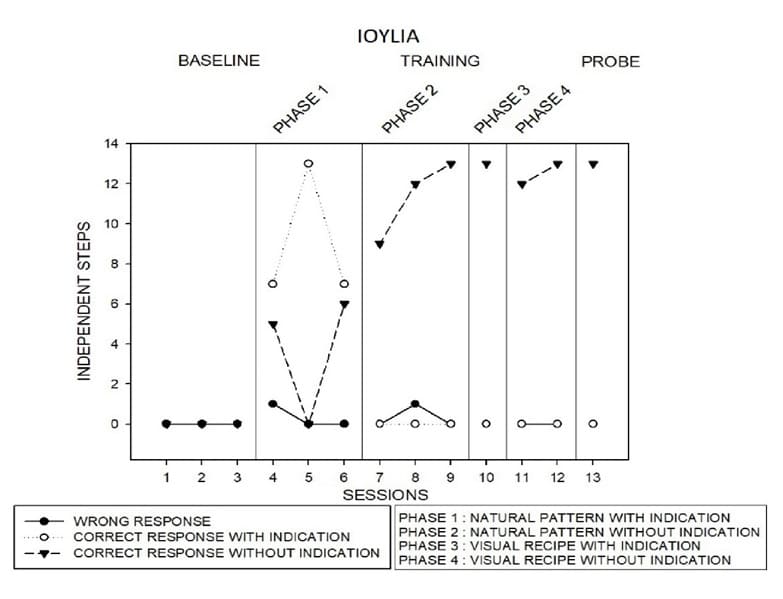
Figure 1: The number of steps/responses per session from Ioulia.
Figure 1 presents Ioulia’s independent steps. Ioulia did not make any steps during the three baselines. During training (Phase 1) Ioulia made 0 to 6 correct steps with the indication by the researcher. During Phase 2 Ioulia made 9 to 13 correct steps without indication. During Phase 3 and 4, in which was given the visual recipe, Ioulia made 12 to 13 correct steps. Finally, during the probe, Ioulia made 13 correct steps without indication and without visual recipe.
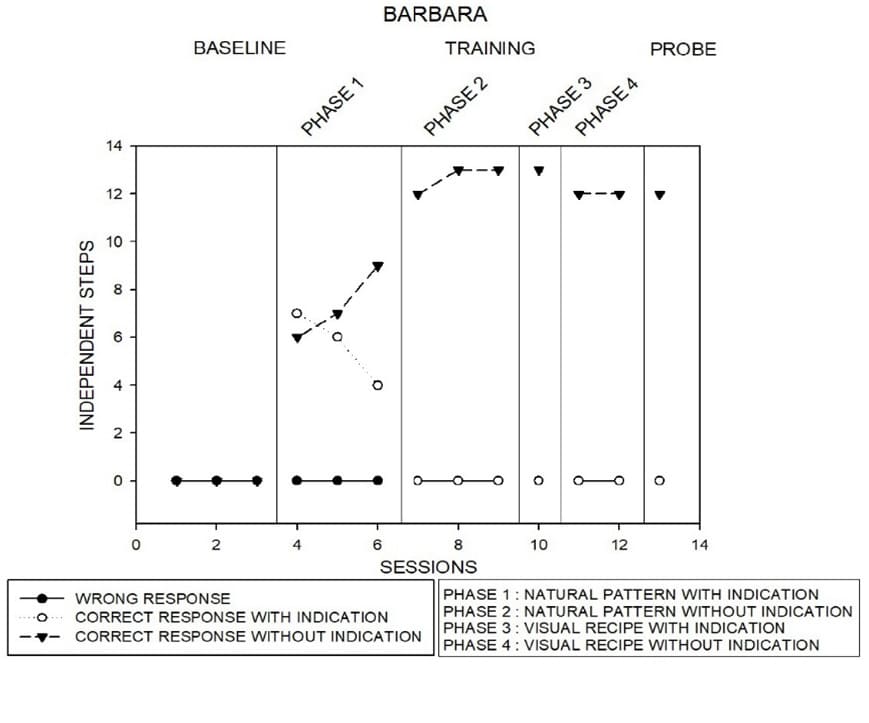
Figure 2 : The number of steps/responses per session from Barbara.
Figure 2 presents Barbara’s independent steps. Barbara did not make any steps during the three baselines. During training (Phase 1) in which was provided natural pattern Barbara made 6 to 9 correct steps without indication. During Phase 2 Barbara increased proper steps to 13. This situation was maintained during Phase 3. During Phase 4 and probe/evaluation Barbara reached 12 correct steps without indication and without visual recipe.
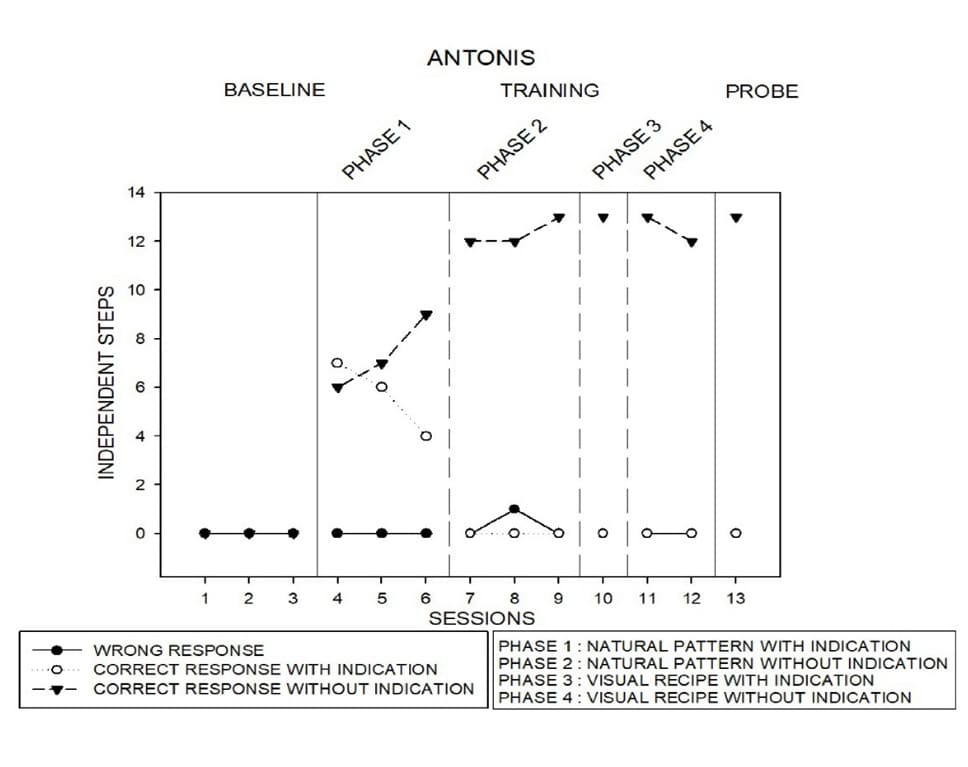
Figure 3: The number of steps/responses per session from Antonis.
Figure 3 presents Antonis’ independent steps. Antonis did not make any steps during the three baselines. During training (Phase 1) in which was provided natural pattern Antonis made 6 to 9 correct steps without indication. During Phase 3 Antonis increased correct steps without indication and maintained the same situation during Phase 4 and evaluation.
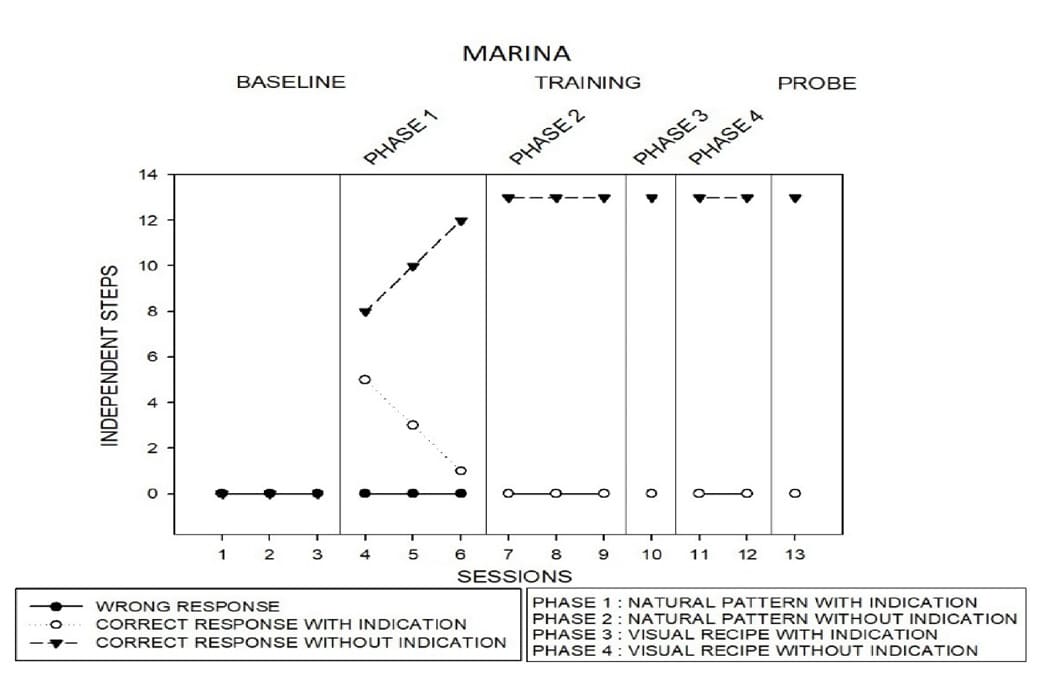
Figure 4: The number of steps/responses per session from Marina.
Figure 4 presents Marina’s independent steps. Marina did not make any steps during the three baselines. During training (Phase 1) in which was provided natural pattern Marina increased the correct steps without indication to 12. During the other Phases and evaluation Marina made all the steps correctly without indication.
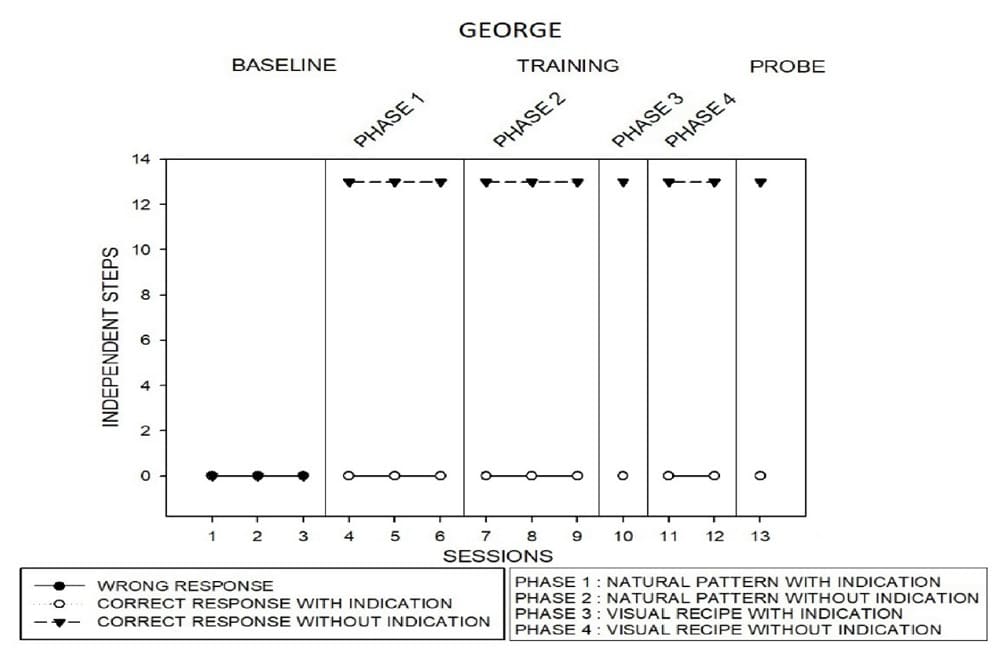
Figure 5 : The number of steps/responses per session from George.
Figure 5 presents George’s independent steps. George did not make any steps during the three baselines. During training (Phase 1, 2, 3, and 4) in which was provided natural patterns and then a visual recipe George made all the steps without indication. He maintained the same level during the evaluation
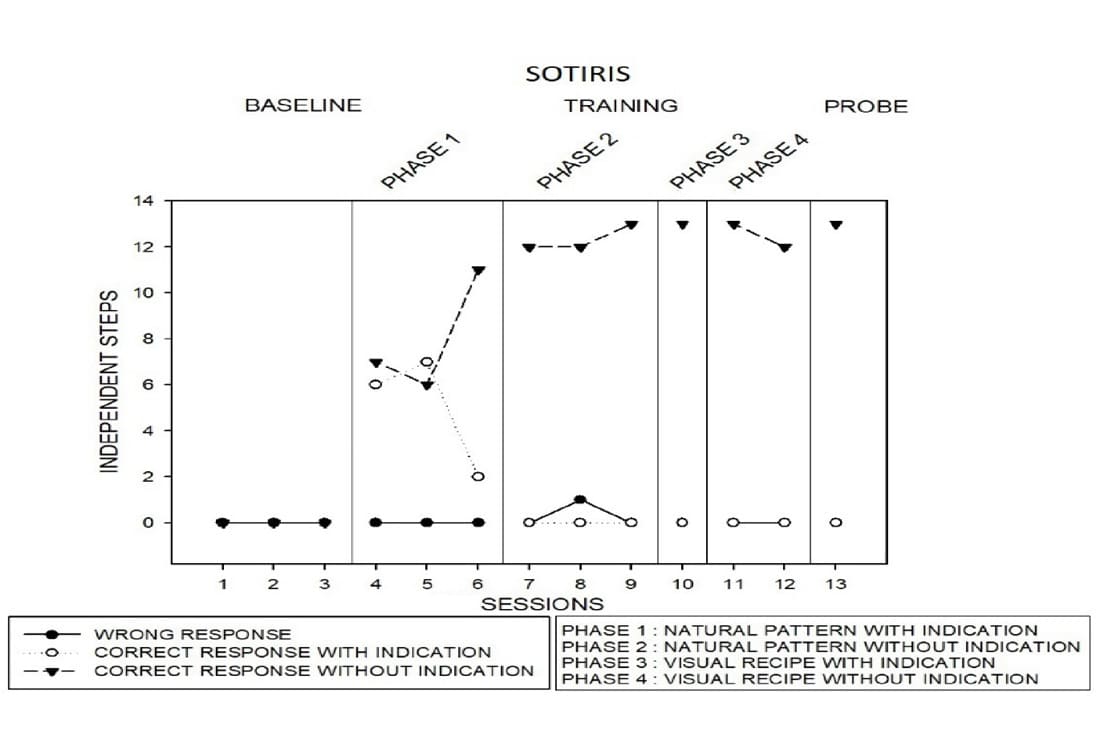
Figure 6: The number of steps/responses per session from Sotiris.
Figure 6 presents Sotiris’ independent steps. Sotiris did not make any steps during the three baselines. During training (Phase 1) in which was provided natural pattern Sotiris made 7 steps with indication. During Phase 2 and 3 Sotiris made 12 to 13 steps without indication. The same level was maintained during Phase 3 and 4, in which was provided visual recipe. During evaluation he made all steps on his own.
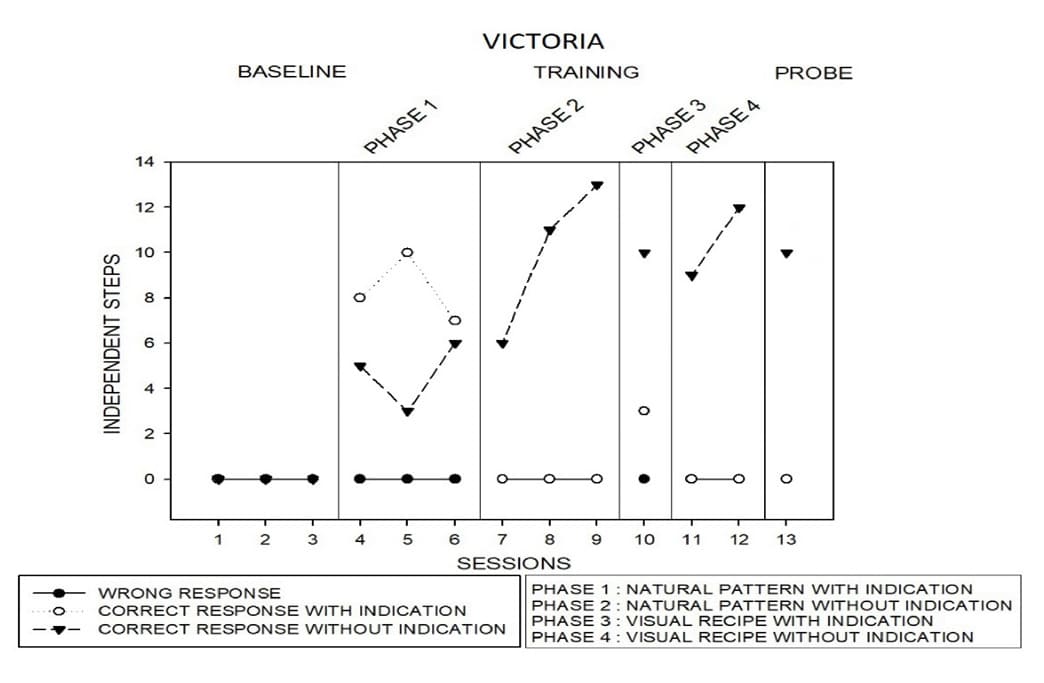
Figure 7: The number of steps/responses per session from Victoria.
Figure 7 presents Victoria’s independent steps. Victoria, as well, did not make any steps during the three baselines. During training (Phase 1) which was provided natural pattern she made 8 and 10 steps with indication, but during Phase 2 she increased the steps from 6 to 13 without indication. During Phase 3 she made 10 steps with visual recipe and indication, while during Phase 4 she made 12 steps without indication. Finally, during evaluation Victoria made 10 steps without indication, natural pattern, or visual recipe.
Social validity
In general, social validity refers to an examination of the social criteria with the goal of evaluating the intervention, procedures used, and the impact they had on the performance of the research participants. Social validity can be assessed in two ways: through social comparison or through subjective appraisal. Through subjective evaluation, target performance is used to validate the intervention’s results. Specialists with decision-making abilities evaluate the target performance that has changed as a result of the intervention. The evaluation is carried out to provide an overall assessment of the research participants’ performance following the intervention. The person asked to judge the participants’ performance should be able to determine whether there has been a significant change in performance against the goal [62].
As a result, a group of teachers was asked to evaluate the intervention in order to determine the reliability of the results and the method’s validity. Five special education teachers responded to the call and watched video excerpts of a baseline (or first) training session and a final session. They had no idea which training session came first and which followed and they couldn’t guess. The instructions were to attend two training sessions of the intervention in random order and to complete a short questionnaire to assess a) which situation (before or after the training) the participants performed better in, and b) the level of improvement. According to the team of teachers, the participants’ overall performance ranged from moderate to high.
Discussion
The goal of this study was to investigate whether people with DD could learn cooking skills like material identification, measurement, mixing and sequencing through an intervention program as well as whether they could recall the recipe when visual and verbal assistance was withdrawn. It is known, that cooking proficiency development is a complex topic in any population because it involves multiple skill sets and serves multiple purposes. Cooking, after all, is not a solitary activity but requires a wide range of skills that address both physical and social aspects, as well as fine and gross motor demands. Cooking necessitates cognitive processing, executive functioning, memory, and cultural participation and is influenced by a variety of factors such as income, social class, gender, and age [68]. In the present study, all seven participants who had DD were able to follow the thirteen steps of the recipe, recognize each material, use the correct quantity and, eventually, to make bread. It is obvious that in the probe-evaluation participants exhibited a greater degree of independence in task completion by recalling from memory all thirteen steps. While the experimental design requires only limited conclusions, the data are encouraging.
A literature review identified various effective teaching practices that assist individuals with DD in learning functional living skills and mainly cooking skills. Examples include video modeling [44-47, 69, 70], video prompting [48], photographs and line drawings [51, 52], illustrated pictures, photographed and/or illustrated task analysis [53, 54], virtual apps installed on tablets [71]. Individuals with DD learn a variety of skills through what they see. It is common knowledge that where the information gained through the sense of sight are registered and explained, then processed and integrated in order to get a complete picture of what it is attempted to be learned. Several strategies (prompting, modeling, reinforcement, shaping, and chaining) and interventions (video modeling, behavioral in vivo procedures, visual cues, and audio cueing) have been shown to be effective in teaching daily living skills to people with ASD [59].
The TEACCH approach also in teaching functional skills like vocational skills, communication skills, social skills, and life skills to young adults with ASD and ID is effective [72]. It is also known that intervention programs for people with DD must be based on a detailed description of each skill to be taught, a precise definition of objectives, the formulation of instructions based on the stage of the process, continuous reinforcement and feedback, strict control of each intervention, the use of supervisory means and charts to track progress, role-playing, and more general behavior modification [73]. People with ID tend to be visual learners and may not be able to read text. As such, incorporating picture recipes into any lessons about cooking will go a long way towards helping them learn the necessary skills. Individuals with DS can remember and comprehend new information better when it is presented in the form of images [74]. This intervention program took into consideration all the above information and by using task analysis, modeling, systematic feedback, reinforcement and visual supporter managed to train adults with DD basic cooking skills. It is worth noting that during the probe/evaluation, the participants retained the recipe despite of the removal of the original components (natural pattern and visual recipe) which were used during the training. The participants were able to recall all or part of the recipe. It is understandable that when individuals with DD have opportunities and use appropriate learning strategies, they can acquire information and develop and improve their skills.
It turns out that intervention programs such as the one described above are very important. Another dimension that must be reported is that there is a therapeutic value in involving people in food preparation as a form of nutritional intervention or health promotion [35, 75, 76]. Cooking ability can improve nutritional status, dietary variety, socialization, and overall health [77, 78]. For individuals with DD the ability to cook and to take care of their nutritional needs is an important aspect of independent living [79]. At the same time, increased cognitive function [80], improved opportunities for social interaction, peer relationship development, quality of life improvement [81] and reduction of anxiety and depression are observed [81]. That’s why training people with disabilities in basic skills is critical if the goal is to create adults who can survive independently in society, form relationships, and participate actively in the societies in which they live [82]. Studies showed that individuals with ID who participated in programs for living and vocational skills regained their autonomy and social inclusion [45].
The transition to independent living should be concentrated mainly during a person’s post-school adolescence and adult years [83, 84]. Facilitating the individuals’ transition to adulthood and working life is dependent on them acquiring the independent living skills they require. Teaching daily living skills to people with DD is critical so that they can deal with the current and future demands of everyday life, such as personal hygiene skills, dressing and taking them off, food preparation, cooking and eating, money, transportation, work skills, time management, and entertainment [85].
Teaching skills to young adults are aimed at teaching specific skills (generally daily life skills) rather than comprehensive and multi-dimensional independent life education programs [86]. Learning to cook can provide individuals with valuable exposure to a variety of academic and functional skills, including decisionmaking, self-determination, reading, budgeting, shopping and food purchasing, item identification, measurement, and sequencing [38]. It is worth mentioning that these skills can be generalized to new situations and stimuli. Though cognitive and social skills are important, developing a life skills training system for individuals with ID to regain independence and relieve social burdens is a practical challenge [87]. Learning to perform functional living skills on their own may enable individuals with DD to care for them, improve their quality of life, and reduce their reliance on others [88]. Achieving independence is one of the cornerstones of our existence and teaching life skills that promote this individuality should be an integral part of the special education system, not an afterthought.
The present study aligns with the new ways of thinking about learning and training, where many naturalistic elements (use of natural pattern, visual recipe, everyday life situations) are drawn into the intervention in order to facilitate a broad generalization of the taught skill in everyday life. The fact that these gains in basic cooking skills were achieved by individuals with DD substantiates the possibility that this intervention will produce similar or better results in populations with milder disabilities, perhaps faster and with less effort devoted to teaching. For better results, such intervention programs can be implemented using multimedia systems that are personalized based on each individual’s needs and preferences.
Future directions-implications
Life skills instruction should be provided in classrooms and community settings, so that students can learn to apply what they have learned in the classroom to their daily lives [89]. Life skills instruction should be the responsibility of both general and special teachers. The special education teacher, in collaboration with the general education teacher, may encourage the inclusion of individuals with DD, and may choose a skill to emphasize each month. In addition, individuals in general education would serve as role models for students with DD. Another long-term goal could be to pair up high school special day class students as mentors or ‘big buddies’ to work with elementary special day class students on a practical life skill [90]. Specific interventions taught in a systematic and explicit manner can improve students’ overall functioning in life and social skills [91]. Last but not least, teachers participating in such programs may benefit from having a basic understanding of behavior analytic services and extensive experience working with these students. This level of behavior analytic support is not always available in typical clinical or educational settings. That is why teacher in Greece must me trained in Applied Behavior Analysis or similar behavioral methods.
Limitations
It is worth noting that only seven people with DD (ID, DS, or ASD with ID) took part in this study. In order for the results to be more representative, future studies may use a more representative sample, investigate additional factors (for example, gender, intellectual age/intelligence quotient, previous “experience,” and environment) and may aim to achieve generalization. Because the goal of the study was simply to show the participants’ performance before and after the intervention, no comparative study was conducted between performance in the baseline and probe. Future research may focus on this topic.
Acknowledgment
The authors would like to thank all participants and the staff members of the residential facility center.
References
- Bennett KD, Dukes C (2013) A systematic review of Teaching Daily Living Skills to adolescents and adults with autism spectrum disorder. Review Journal of Autism and Developmental Disorders 1: 2-10.
- Cronin ME (1996) Life Skills Curricula for Students with Learning Journal of Learning Disabilities 29: 53-68.
- Chiang HM, Ni X, Lee YS (2017) Life Skills Training for Middle and High School Students with Autism. Journal of Autism and Developmental Disorders 47: 1113-1121.
- Nietupski J, Hamre-Nietupski S, Curtin S, Shrikanth K (1995) A Review of Curricular Research in Severe Disabilities from 1976 to 1995 in Six Selected Journals. The Journal of Special Education 31: 36-55.
- American Psychiatric Association (2013) Diagnostic and statistical manual of mental disorders. Diagnostic and Statistical Manual of Mental Disorders.
- American Association on Intellectual and Developmental Disabilities (2019) Defining Criteria for Intellectual Disability.
- Rhodes KT, Branum-Martin L, Morris RD, Romski M, Sevcik RA(2015) Testing Math or Testing Language? The Construct Validity of the KeyMath-Revised for Children with Intellectual Disability and Language Difficulties. American Journal on Intellectual and Developmental Disabilities 120: 542-568.
- Lappa CS, Mantzikos CN (2019) Teaching social skills in small groups of children with multiple disabilities: motor and intellectual disabilities. An intervention program. European Journal of Special Education Research 4: 57-77.
- Lappa CS, Mantzikos CN (2021) Teaching Individuals with Down Syndrome and Moderate or Severe Intellectual Disability with The Aim of Their Acquiring, Retaining and Recalling Knowledge: An Intervention Programme for Discovering and Understanding The Environment. International Journal of Pedagogy and Teacher Education 5: 66-81.
- Papadaki E, Ntoa S, Adami I, & Stephanidis C (2018) Let’s cook: An Augmented Reality System, Towards Developing Cooking Skills for Children with Cognitive Impairments. In B. Guidi, L. Ricci, C. Calafate, Gaggi, & J. Marquez-Barja (Eds.), Smart Objects and Technologies for Social Good, Springer Pp: 237-247.
- Park J, Bouck E, Duenas A (2018) The Effect of Video Modeling and Video Prompting Interventions on Individuals With Intellectual Disability: A Systematic Literature Review. Journal of Special Education Technology 34: 3-16.
- Anderson JS, Nielsen JA, Ferguson MA, Burback MC, Cox ET, et al.(2013) Abnormal brain synchrony in Down Syndrome. NeuroImage: Clinical 2: 703-715.
- Contestabile A, Benfenati F, Gasparini L (2010) Communication breaks-Down: From neurodevelopment defects to cognitive disabilities in Down syndrome. Progress in Neurobiology 91: 1-22.
- Macchini F, Leva E, Torricelli M, Valadè A (2011) Treating acid reflux disease in patients with Down syndrome: pharmacological and physiological approaches. Clinical and Experimental Gastroenterology 4: 19-22.
- Lott IT, Dierssen M (2010) Cognitive deficits and associated neurological complications in individuals with Down’s syndrome. TheLancet Neurology 9: 623-633.
- Baroody AJ (1995) Self-invented addition strategies by children with mental retardation. American journal of mental retardation: AJMR 101: 72-89.
- Bashash L, Outhred L, Bochner S (2003) Counting Skills and Number Concepts of Students with Moderate Intellectual International Journal of Disability, Development and Education 50: 325-345.
- Abbeduto L, Pavetto M, Kesin E, et al. (2001) The linguistic and cognitive profile of Down syndrome: Evidence from a comparison with fragile X syndrome. Down Syndrome Research and Practice 7 : 9-15.
- Lappa C, Kyparissos N, Paraskevopoulos S (2011) Teaching Conversation in Small Groups of Children and Adults With Moderate and Severe Mental Retardation. European Journal of Behavior Analysis 12: 249-262.
- Iacob I, Musuroi C (2013) Aspects of Adapting the Intervention Program to the Particular Learning Profile of Children’s with Down Procedia - Social and Behavioral Sciences 84: 846-849.
- Salvaras I (2013) Teaching Children with Special Needs in Ordinary School. Grigoris Publications.
- Mara D, Mara EL. (2011) Characteristics of Learning Process atChildren with Down Syndrom. Procedia - Social and Behavioral Sciences 30: 73-78.
- de la Iglesia CJF, Buceta JM, Campos A (2005) Prose learning in children and adults with Down syndrome: The use of visual and mental image strategies to improve recall. Journal of Intellectual & Developmental Disability 30: 199-206.
- Zeidan J, Fombonne E, Scorah J, Ibrahim A, Durkin MS, et al. (2022) Global prevalence of autism: A systematic review update. AutismResearch 15: 778-790.
- Mannion A, Brahm M, Leader G (2014) Comorbid Psychopathology in Autism Spectrum Disorder. Review Journal of Autism and Developmental Disorders 1: 124-134.
- den Brok WLJE, Sterkenburg PS (2014) Self-controlled technologies to support skill attainment in persons with an autism spectrum disorder and/or an intellectual disability: a systematic literature review. Disability and Rehabilitation: Assistive Technology 10: 1-10.
- Browder DM, Jimenez BA, Trela K (2012) Grade-Aligned Math Instruction for Secondary Students with Moderate Intellectual Education and Training in Autism and Developmental Disabilities 47: 373-388.
- Dillenburger K (2012) Why reinvent the wheel? A behaviour analyst’s reflections on pedagogy for inclusion for students with intellectual and developmental disability. Journal of Intellectual & Developmental Disability 37: 169-180.
- Cannella-Malone HI, Miller O, Schaefer JM, Jimenez ED, Page EJ, et (2015) Using Video Prompting to Teach Leisure Skills to Students With Significant Disabilities. Exceptional Children 82: 463-478.
- Graves TB, Collins BC, Schuster JW, Kleinert H (2005) Using Video Prompting to Teach Cooking Skills to Secondary Students with Moderate Disabilities. Education and Training in Developmental Disabilities 40: 34-46.
- Mechling LC, Gast DL, Fields EA (2008) Evaluation of a Portable DVD Player and System of Least Prompts to Self-Prompt Cooking Task Completion by Young Adults With Moderate Intellectual The Journal of Special Education 42: 179-190.
- Sigafoos J, O’Reilly M, Cannella H, Edrisinha C, de la cruz B, et (2007) Evaluation of a Video Prompting and Fading Procedure for Teaching Dish Washing Skills to Adults with Developmental Disabilities. Journal of Behavioral Education 16: 93-109.
- Begley A, Gallegos D (2010) What’s cooking for dietetics? A review ofthe literature. Nutrition & Dietetics 67: 26-30.
- McGowan L, Caraher M, Raats M, Lavelle F, Hollywood L, et al. (2017)Domestic cooking and food skills: A review. Critical reviews in food science and nutrition 57: 2412-2431.
- Hartmann C, Dohle S, Siegrist M (2013) Importance of cooking skills for balanced food choices. Appetite 65: 125-131.
- Stead M, Caraher M, Wrieden W, Longbottom P, Valentine K, et al. (2004) Confident, fearful and hopeless cooks. British Food Journal 106: 274-287.
- Fordyce-Voorham S (2011) Identification of Essential Food Skills forSkill-based Healthful Eating Programs in Secondary Schools. Journal of Nutrition Education and Behavior 43: 116-122.
- Madaus JW, Pivarnik L, Patnoad M, Scarpati S, Richard N, et al. (2010) Teaching Food Safety Skills to Students with Disabilities. Teaching Exceptional Children 42: 44-51.
- Cameto R, Marder C, Wagner M, Cardoso D (2003) Youth Employment. A report from the national longitudinal transitional study-2.
- Delano ME (2007) Video Modeling Interventions for Individuals with Remedial and Special Education 28: 33-42.
- McCoy K, Hermansen E (2007) Video Modeling for Individuals with Autism: A Review of Model Types and Effects. Education and Treatment of Children 30: 183-213.
- Mechling LC, Gast DL, Seid NH (2009) Using a Personal Digital Assistant to Increase Independent Task Completion by Students with Autism Spectrum Disorder. Journal of Autism and Developmental 39: 1420-1434.
- Mechling LC, Gustafson MR (2008) Comparison of Static Picture and Video Prompting on the Performance of Cooking-Related Tasks byStudents with Autism. Journal of Special Education Technology 23: 31-45.
- Ayres K, Cihak D (2010) Computer- and Video-Based Instruction of Food-Preparation Skills: Acquisition, Generalization, and Intellectual and Developmental Disabilities 48: 195-208.
- Cheung JCW, Tam EWC, Mak AHY, Chan TTC, Zheng YP (2022) A Night-Time Monitoring System (eNightLog) to Prevent Elderly Wandering in Hostels: A Three-Month Field Study. International Journal of Environmental Research and Public Health 19: 2103.
- Domire SC, Wolfe P (2014) Effects of Video Prompting Techniques on Teaching Daily Living Skills to Children With Autism Spectrum Research and Practice for Persons with Severe Disabilities 39: 211-226.
- Mousa Al-Salahat M (2016) Using of Video Modeling in Teaching a Simple Meal Preparation Skill for Pupils of down Syndrome. Journal of education and practice 7: 82-90.
- Gardner SJ, Wolfe PS (2014) Teaching Students With Developmental Disabilities Daily Living Skills Using Point-of-View Modeling Plus Video Prompting With Error Correction. Focus on Autism and Other Developmental Disabilities 30: 195-207.
- Aljehany MS, Bennett K (2018) Meta-Analysis of Video Prompting to Teach Daily Living Skills to Individuals With Autism Spectrum Journal of Special Education Technology 34: 17-26.
- Aljehany MS, Bennett KD (2020) A Comparison of Video Prompting toLeast-to-Most Prompting among Children with Autism and Intellectual Journal of Autism and Developmental Disorders 50: 17141724.
- Lancioni GE, O’Reilly MF (2001) Self-management of instruction cues for occupation: review of studies with people with severe and profound developmental disabilities. Research in Developmental Disabilities 22: 41-65.
- Lancioni GE, O’Reilly MF (2002) Teaching Food Preparation Skills to People with Intellectual Disabilities: a Literature Overview. Journal ofApplied Research in Intellectual Disabilities 15: 236-253.
- Bergstrom T, Patttavina S, Martella RC, Marchand-Martella NE (1995) Microwave Fun User-Friendly Recipe Cards. Teaching Exceptional Children 28: 61-63.
- Singh NN, Oswald DP, Ellis CR, Singh SD (1995) Community-based instruction for independent meal preparation by adults with profound mental retardation. Journal of Behavioral Education 5: 77-91.
- Martin JE, Mithaug DE, Frazier ES (1992) Effects of picture referencing on PVC chair, love seat, and sette assemblies by students with mental Research in Developmental Disabilities 13: 267-286.
- Pierce KL, Schreibman L (1994) Teaching daily living skills to children with autism in unsupervised settings through pictorial self Journal of Applied Behavior Analysis 27: 471-481.
- Alberto PA, Cihak DF, Gama RI (2005) Use of static picture promptsversus video modeling during simulation instruction. Research inDevelopmental Disabilities. 26: 327-339.
- Cihak D, Alberto PA, Taber-Doughty T, Gama RI (2006) A Comparison of Static Picture Prompting and Video Prompting Simulation Strategies Using Group Instructional Procedures. Focus on Autism and Other Developmental Disabilities 21: 89-99.
- Ninci J, Neely LC, Hong ER, Boles MB, Gilliland WD, et al. (2015) Meta-analysis of Single-Case Research on Teaching Functional Living Skills to Individuals with ASD. Review Journal of Autism and Developmental Disorders 2: 184-198.
- Alwell M, Cobb B (2009) Functional Life Skills Curricular Interventions for Youth With Disabilities. Career Development for Exceptional Individuals 32: 82-93.
- Bouck EC (2010) Reports of life skills training for students with intellectual disabilities in and out of school. Journal of Intellectual Disability Research 54: 1093-1103.
- Kazdin AE (2011) Single-Case Research Designs: Methods for Clinical and Applied Settings. Oxford University Press.
- Chen C (2023) Theoretical Bases for Using Virtual Reality in Education. Themes in science and technology education Pp: 71-90.
- Nabors L, Monnin J, Jimenez S (2020) A Scoping Review of Studies on Virtual Reality for Individuals with Intellectual Disabilities. Advances in Neurodevelopmental Disorders 4: 344-356.
- Burden PR, Byrd DM (2019) Methods for Effective Teaching: Meeting the Needs of All Students. Pearson.
- Heward WL (2018) Exceptional Children: An Introduction to Special Education. Pearson.
- Tan HC, Hughes MR, Toogood S (2016) Using task analysis to promote engagement in special educational settings. European Journal of Behavior Analysis 17: 116-130.
- Adams J, White M (2015) Prevalence and socio-demographic correlates of time spent cooking by adults in the 2005 UK Time Use Cross-sectional analysis. Appetite 92: 185-191.
- Palechka G, MacDonald R (2010) A Comparison of the Acquisition of Play Skills Using Instructor-Created Video Models and Commercially Available Videos. Education and Treatment of Children 33: 457-474.
- Sancho K, Sidener TM, Reeve SA, Sidener DW (2010) Two Variations of Video Modeling Interventions for Teaching Play Skills to Children with Autism. Education and Treatment of Children 33: 421-442.
- Panerai S, Catania V, Rundo F, Ferri R (2018) Remote HomeBased Virtual Training of Functional Living Skills for Adolescents and Young Adults with Intellectual Disability: Feasibility and Preliminary Frontiers in Psychology.
- Siu AMH, Lin Z, Chung J (2019) An evaluation of the TEACCHapproach for teaching functional skills to adults with autism spectrumdisorders and intellectual disabilities. Research in Developmental Disabilities 90: 14-21.
- Hauritz M, Riches V, Parmenter TR, Ward J. (1980) Program Development for the Acquisition of Work and Social Skills. Australian Journal of Developmental Disabilities 6: 11-16.
- Yussof RL, Paris TN (2011) Reading activities using scaffolding in MEL-SindD for Down Syndrome children. Procedia- Social Behavioral Sciences 35: 121-128.
- Chu YL, Farmer A, Fung C, Kuhle S, Storey KE, et al. (2012)Involvement in home meal preparation is associated with food preference and self-efficacy among Canadian children. Public Health Nutrition 16: 108-112.
- Condrasky MD, Baruth M, Wilcox S, Carter C, Jordan JF (2013) Cooks training for Faith, Activity, and Nutrition project with AME churches in Evaluation and Program Planning 37: 43-49.
- Chen RCY, Lee MS, Chang YH, Wahlqvist ML (2012) Cooking frequency may enhance survival in Taiwanese elderly. Public Health Nutrition 15: 1142-1149.
- Erlich R, Yngve A, Wahlqvist ML (2012) Cooking as a healthy Public Health Nutrition 15: 1139-1140.
- Humphries K, Traci MA, Seekins T (2008) Nutrition Education and Support Program for Community-Dwelling Adults with Intellectual Taylor SJ, ed. Intellectual and Developmental Disabilities 46: 335-345.
- García-Villamisar D, Hughes C (2007) Supported employment improves cognitive performance in adults with Autism. Journal ofIntellectual Disability Research 51: 142-150.
- Hillier AJ, Fish T, Siegel JH, Beversdorf DQ (2011) Social and Vocational Skills Training Reduces Self-reported Anxiety and Depression Among Young Adults on the Autism Spectrum. Journal of Developmental and Physical Disabilities 23: 267-276.
- Dellasoudas L (2005) Teaching Students with Special Educational Needs. From Theory to Practice. Atrapos Publications. [In Greek]
- Hanley-Maxwell C, Collet-Klingenberg L (2011) Education. Sage
- Strnadová I, Cumming TM, Danker J (2016) Transitions for Students with Intellectual Disability and/or Autism Spectrum Disorder: Carer and Teacher Perspectives. Australasian Journal of Special Education 40: 141-156.
- Friend M (2013) Special Education. Pearson Higher Ed.
- Belva BC, Matson JL (2013) An examination of specific daily living skills deficits in adults with profound intellectual disabilities. Research in Developmental Disabilities 34: 596-604.
- Simmons D, Chapman GE (2012) The significance of home cooking within families. British Food Journal 114: 1184-1195.
- Hong ER, Ganz JB, Mason R, Morin K, Davis JL, et al. (2016) Theeffects of video modeling in teaching functional living skills to persons with ASD: A meta-analysis of single-case studies. Research in Developmental Disabilities 57: 158-169.
- Clark GM, Field S, Patton JR, Brolin DE, Sitlington PL (1994) Life Skills Instruction: A Necessary Component for All Students with Disabilities A Position Statement of the Division on Career Development and Career Development for Exceptional Individuals 17: 125133.
- deRecat E (2019) Dominican Scholar Dominican Scholar Life Skills for Life-Long Learners: Teaching Functional Skills to Life Skills for LifeLong Learners: Teaching Functional Skills to Elementary Students with Special Needs Elementary Students with Special Needs. Unpublished Master’s Thesis.
- Storey K, Miner CA (2017) Systematic Instruction of Functional Skills for Students and Adults with Disabilities. Charles C. Thomas Publisher Ltd.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.