Stereotactic parietal transtentorial placement of a catheter into a pontine cyst of a pilocytic astrocytoma is a safe treatment option
by Thomas Fortmann1,3*§, Samer Zawy Alsofy2,3§, Ralf Stroop3, Antonio Santacroce3, Makoto Nakamura3, Christian Ewelt2, Ralph Lehrke1
1Department of Stereotactic Neurosurgery, St. Barbara Clinic Hamm, Am Heessener Wald 1, 59073 Hamm, Germany
2Department of Neurosurgery, St. Barbara Clinic Hamm, Am Heessener Wald 1, 59073 Hamm, Germany.
3Medical Faculty, University of Witten-Herdecke, Witten Herdecke, Germany
*Corresponding author: Thomas Fortmann, Department of Stereotactic Neurosurgery, St. Barbara Clinic Hamm, Am Heessener Wald 1, 59073 Hamm, Germany.
§ These authors contributed equally to this work.
Received Date: 15 Octobeer 2025
Accepted Date: 20 October 2025
Published Date: 22 October 2025
Citation: Fortmann T, Alsofy S Z, Stroop R, Santacroce A, Nakamura M, et all (2025) Stereotactic parietal transtentorial placement of a catheter into a pontine cyst of a pilocytic astrocytoma is a safe treatment option J Surg 10: 11471 https://doi.org/10.29011/2575-9760.011471
Abstract
Pilocytic astrocytomas of the brainstem are rarely amenable to complete resection. Residual tumor tissue is commonly managed through observation or adjuvant radiotherapy. As a late complication of resection or brachytherapy, space-occupying cysts may develop in approximately 12% of patients. Symptomatic cystic lesions typically necessitate surgical intervention. In cases where patients decline open surgical procedures, stereotactic approaches offer a minimally invasive alternative.
We report on the case of a patient with a recurrent pontine cyst associated with a pilocytic astrocytoma. The lesion had previously been treated by open surgical resections and subsequently by suboccipital stereotactic aspirations. Despite these interventions, the cyst recurred, resulting in pronounced gait disturbances. Following a comprehensive review of the literature, a stereotactic parietal transtentorial approach was selected for the placement of a catheter connected to a subgaleal Rickham reservoir. The procedure was performed without complications, and the patient exhibited rapid clinical improvement postoperatively.
To the best of our knowledge, this represents the first reported case of a pontine cyst arising from a pilocytic astrocytoma treated via this approach. The described trajectory appears to be a safe and effective treatment option in carefully selected patients.
Keywords: Stereotaxy; Stereotactic parietal transtentorial trajectory; Pilocytic astrocytoma; Pontine cyst
Introduction
Pilocytic astrocytomas are benign tumors of the central nervous system. Complete surgical resection is associated with a more favorable prognosis. Bond et al. reported that 31% of patients experience tumor recurrence, with a significant difference between those who underwent gross total resection (27%) and those with subtotal resection (73%) [1]. These astrocytomas frequently occur within the brainstem, where complete resection is often challenging due to the tumor’s critical location [2]. When residual tumor tissue remains, management options include observation, radiotherapy, or brachytherapy. Brachytherapy has demonstrated a high response rate and excellent local control, achieving an overall survival rate of 86.2% at 10 years [3]. However, space-occupying cysts develop in approximately 12.8% of patients treated with either resection or brachytherapy.
We present the case of a patient diagnosed in 2004 with a brainstem
tumor following the onset of gait disturbance. After complete resection, no residual tumor was detected. In 2006, a space-occupying cyst developed and was treated with stereotactic drainage. Following recurrent symptomatic cyst formation, additional resections were performed in 2007 and 2008. In 2014, the patient presented with hemifacial pain due to cyst recurrence, which was drained and connected to a subgaleal Rickham reservoir.
In 2019, gait disturbances reappeared as the cyst enlarged; the Rickham reservoir was found to be occluded and was subsequently removed, followed by stereotactic cyst drainage. In 2023, an open surgical resection and fenestration of multiple cysts were performed. Postoperatively, the patient developed a transient hemiparesis and permanent deafness. In June 2025, the pontine cyst recurred once more, resulting in renewed gait impairment (Figure 1).
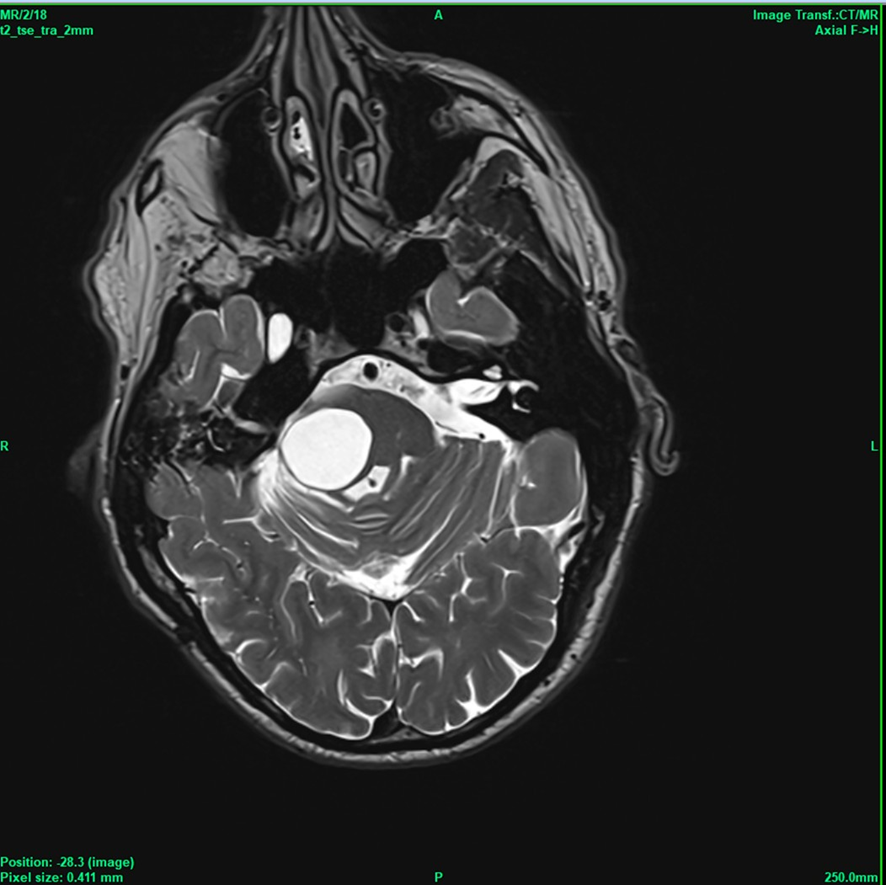
Figure 1 Space occupying cyst causing gait disturbances.
The patient declined open surgery; therefore, stereotactic aspiration of the cyst was offered as an alternative. Following aspiration, the patient’s condition improved for approximately three months before gait disturbances recurred. To facilitate future management, the placement of a Rickham reservoir was considered. Up to that point, all stereotactic cyst aspirations and the initial Rickham reservoir placement had been performed with the patient in the prone position via a right infratentorial approach. During the most recent open resection, a large infratentorial craniectomy had been performed (Figure 2).
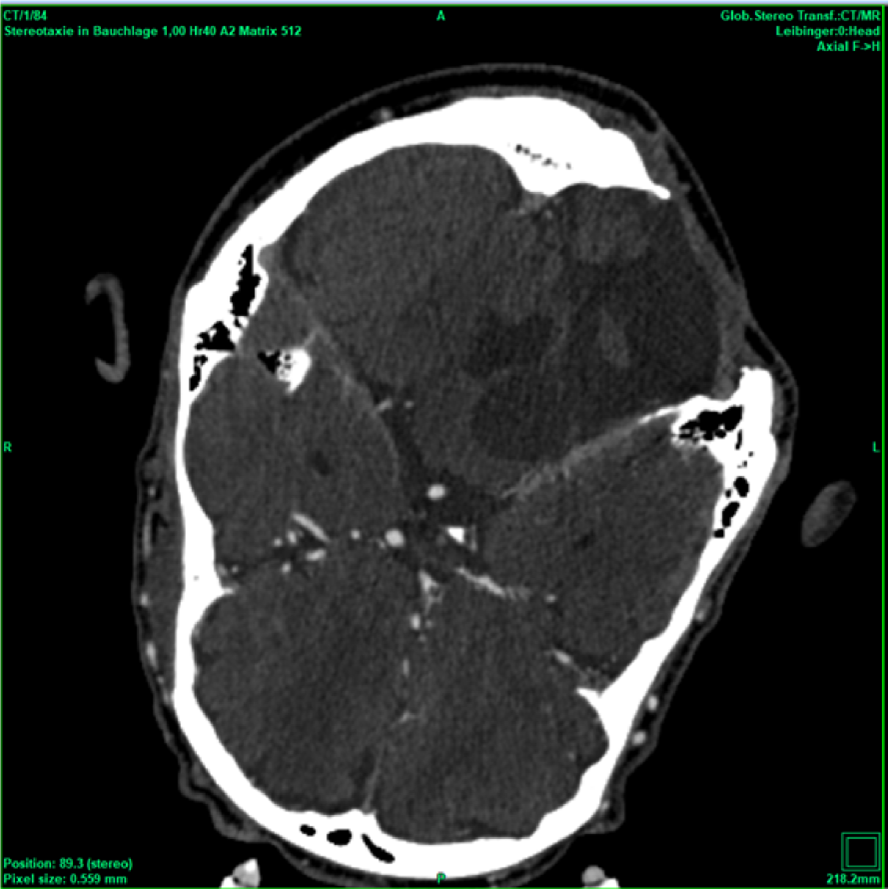
Figure 2 Large bony defect after right suboccipital craniectomy (patient in prone position!).
The most recent cyst aspiration was performed through the existing surgical scar using a stereotactic guide tube to perforate the dura, allowing for minimal dural opening. (Figure 3).

Figure 3 Suboccipital puncture and aspiration of the cyst in June 2025.
Placing the Rickham reservoir ipsilaterally in contact with bone did not provide a stable fixation option. A contralateral infratentorial placement would have traversed the ipsilateral dentate nucleus, as well as the fourth ventricle and the facial nerve nucleus. A contralateral frontal approach, as described by Amundson et al. would have intersected the ipsilateral corticospinal tract [3]. Consequently, we considered whether a transtentorial approach could represent a safe alternative for our patient and conducted a review of the literature to evaluate this option.
Materials and methods
Pubmed and medline analysis
In this study the pubmed and medline databases were analysed using the terms “stereotactic” AND “transtentorial”. All occurring papers were reviewed and included, if both terms really met our criteria.
Stereotactic procedure
The patient was offered the alternative treatment of open fenestration and was informed that there was little to no experience regarding the outcome of this new procedure. Informed consent was obtained. On the day of the procedure, the patients received total intravenous anesthesia and a single shot of 1.5 g cefuroxime. The patient’s head was fixed in a aluminum ring (Precisis AG, Heidelberg, Germany) within a prone position. MR images with 2mm slices and a stereotactic CT were uploaded into the inomed iPS 6.0 software (inomed, Emmendingen, Germany). Several potential trajectories were evaluated to determine the safest surgical approach. A parietal transtentorial route was ultimately selected (Figure 4).
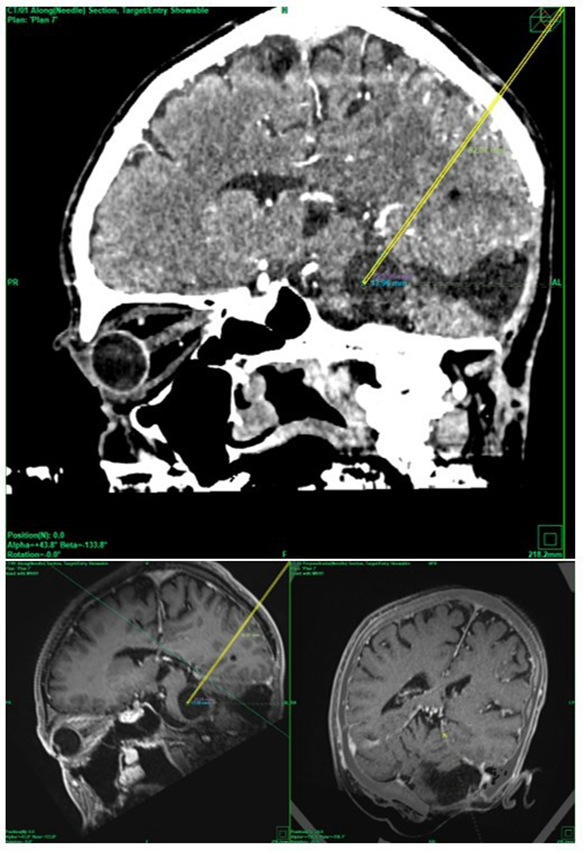
Figure 4 Stereotactic parietal transtentorial approach within the stereotactic CT scan (top) and within the MRI (bottom).
Stereotactic coordinates were established using a Riechert–Mundinger frame (Precisis AG, Heidelberg, Germany) and verified with a stereotactic phantom (Precisis AG, Heidelberg, Germany). The distance from the skull to the tentorium was measured, and a Backlund biopsy needle was advanced along this trajectory.
As the Backlund cannula was unable to perforate the tentorium, the biopsy spiral was utilized. The spiral was gently rotated through the tentorium; however, it could not be retracted to complete the perforation. Therefore, the Backlund needle was rotated around the spiral until the tentorium was successfully penetrated. The spiral was then removed, and the inner component of the Backlund needle was reinserted (Figure 5).
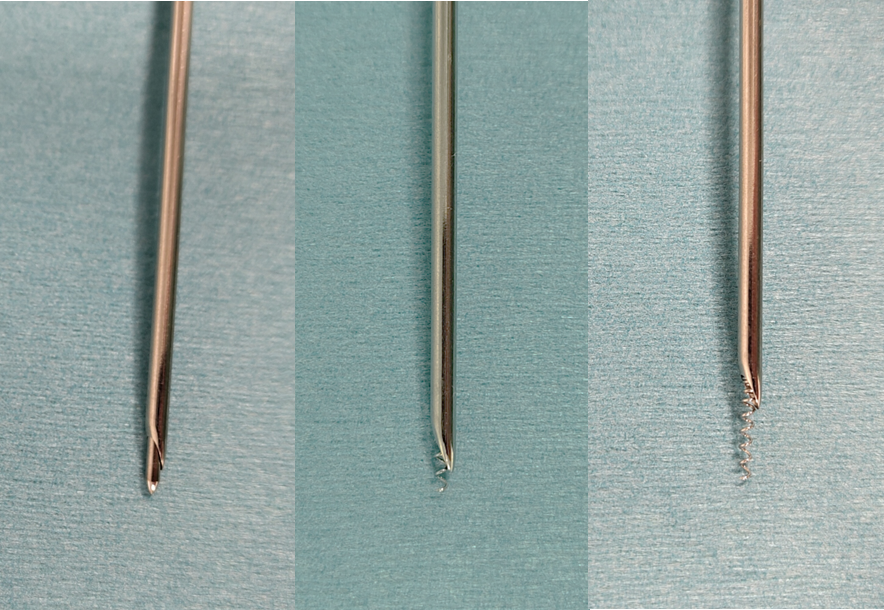
Figure 5 Backlund biopsy needle with inlay (left), with biopsy spiral beginning to exit (middle) and at end position of biopsy spiral (right).
A Rickham reservoir was connected to a 92 mm catheter, which, with its guiding wire, was introduced through a secondary guiding sleeve. The cyst was punctured using the Backlund needle, which was then withdrawn, allowing insertion of the Rickham catheter. The cyst volume was measured by 7 mL. The Rickham reservoir was accessed and aspirated slowly; approximately 7 mL of viscous, yellow, gel-like fluid was evacuated, followed by cerebrospinal fluid, at which point aspiration was discontinued.
The wound was subsequently closed, and an immediate postoperative CT scan was obtained to confirm correct catheter placement and exclude potential complications (Figure 6).
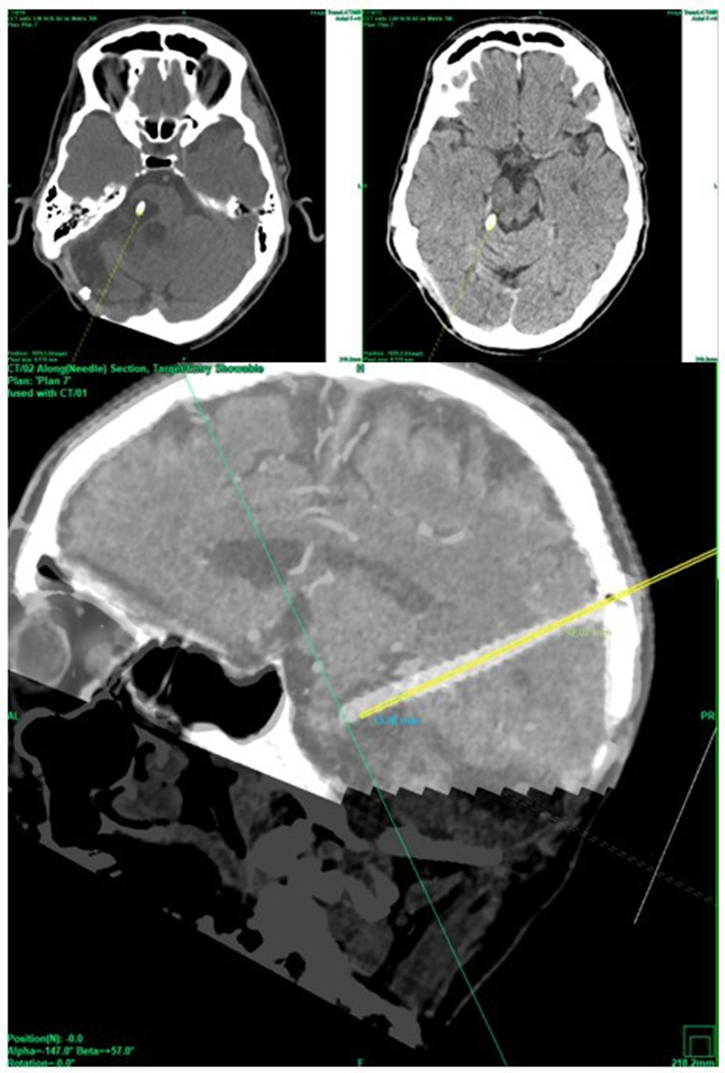
Figure 6 Immediate post-operative CT scan showing correct placement of catheter within the smaller cyst (left) and no adverse event at the breakthrough point of the tentorium, and a good alignment along the planned trajectory (bottom).
Results
Pubmed and medline analysis
The search was done using the NLM Medical subject headings MeSH terms “stereotactic” and “transtentorial” and the Boolean operator “AND”. 32 citations were listed and reviewed. 26 publications covered infratentorial procedures and were excluded. Of the remaining six publications two focused on a transtentorial but transhiatal approach [4,5] (Figure 1).
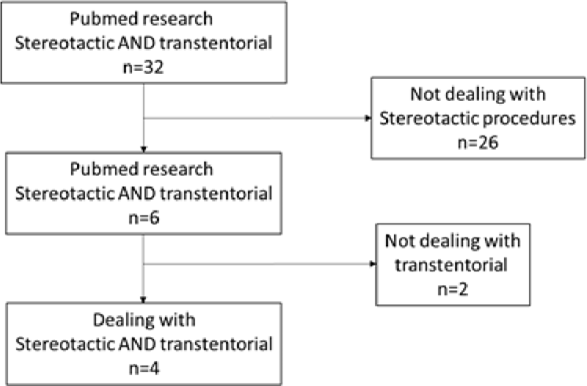
Figure 7: PRISMA flow diagram of pubmed/ medline research.
Medical subject headings “stereotactic” and “transtentorial” where combined using Boolean operator “AND”. All publications were reviewed and excluded if the topic does not match the topic. Only four publications are relevant.
The first publication is a case report of a cerebellar vermian abscess with was drained successfully. The second publication deals with trapped fourth ventricles in four patients that were treated successfully. The remaining four publications deal with different diseases.
Aung et al. show a case of a stereotactic aspiration of the cystic pontine lesion of a pulmonary adenoma via an occipital transtentorial route using a subgaleal Ommaya reservoir for follow up aspirations [6].
Galanda et al. treated nine patients with cerebral palsy with deep wire electrodes, which were placed trantentorailly directly into the anterior lobe of cerebellum [7].
Garber et al. analysed patients with trapped fourth ventricles. They report 11 patients in which a shunt was place stereotactically from parietal through the tentorium [8].
Turner et al. demonstrated three patients with cystic lesions (Dandy Walker malformation, arachnoid cyst and trapped fourth ventricle) which were treated successfully with a transtentorially placed cysto-peritoneal shunt [9]. A summary of all cases is presented in Table 1.
|
Author |
Published in |
N= |
Pathology location |
Disease |
|
Galanda et. al. |
1980 |
9 |
Anterior lobe of cerebellum |
Cerebral palsy |
|
Aung et al. |
1997 |
1 |
Pons |
Metastasis of pulmonary adenocarcinoma |
|
Turner et al. |
2011 |
3 |
Posterior fossa |
Dandy Walker malformation, arachnoid cyst and trapped fourth ventricle |
|
Garber et al. |
2013 |
11 |
Fourth ventricle |
Trapped fourth ventricle |
|
Fortmann et al. |
2025 |
1 |
Pons |
Pilocytic astrocytoma |
Table 1 Overview over published cases and our case.
Patient outcome
After the postoperative CT scan showed a correct placement of the catheter without any bleeding complication the patient was extubated. He showed no new deficit. The following day he mobilized himself without assistance and was able to walk freely without assistance.
Discussion
A review of the literature identified 24 previously published cases in which a transtentorial trajectory was utilized. The majority of these cases (n = 14) involved treatment of a trapped fourth ventricle [8,9]. An additional nine cases described the placement of electrodes within the anterior lobe of the cerebellum for the management of cerebral palsy [7]. Only one reported case involved the transtentorial placement of a catheter connected to a subgaleal Ommaya reservoir to drain a space-occupying pontine cyst secondary to a metastatic pulmonary adenocarcinoma [6]. This latter case bears notable similarity to ours.
To our knowledge, the present report represents the first documented case of a pontine cyst associated with a pilocytic astrocytoma successfully treated through transtentorial catheter placement connected to a Rickham reservoir. The patient experienced rapid symptomatic relief within 24 hours postoperatively and no procedure-related complications.
All previously published cases originated from centers with substantial experience in stereotactic procedures or in the management of tumors via transtentorial approaches. With the addition of our case, a total of 25 transtentorial stereotactic procedures have now been reported—ours being the first published in twelve years since the work of Garber et al. This limited number underscores that transtentorial trajectories are not part of routine clinical practice and should remain reserved for highly selected cases in which alternative approaches are not feasible. In the present case, the combination of an extensive prior suboccipital craniectomy and the patient’s refusal of open surgical fenestration prompted the consideration of this technique.
Conclusion
Stereotactic transtentorial procedures are rarely performed, with only 24 cases reported in the literature. We present the first case of stereotactic parietal transtentorial catheter placement into a pontine cyst of a pilocytic astrocytoma. This approach is technically feasible and represents a safe procedure in selected patients.
Author Contribution Statement
Designed research: T.F, S.Z.A. R.S., R.L.; performed research: T.F., A.S., R.L.; analyzed data: T.F., S.Z.A., R.L.; data acquisition: A.S., C.E.; Writing original draft: T.F.; review & editing: All. All authors have read and agreed to the published version of the manuscript.
Ethics Approval Statement
The patient was offered different treatment options: open fenestration, repeated puncture of the cyst through a suboccipital approach and the transtentorial placement of a catheter connected to a Rickham reservoir. He was informed that there was little to no experience regarding the outcome of this new procedure. If the tentorium would not be perforated safely, the suboccipital approach was planned as alternativ. Informed consent was obtained.
Funding
This work was not funded.
Data Availability Statement
Data generated during this study are available from the corresponding author on reasonable request.
Conflict of Interest Statement
The authors declare no conflict of interest.
References
- Bond KM, Hughes JD, Porter AL, Orina J, Fang S, Parney IF. Adult Pilocytic Astrocytoma: An Institutional Series and Systematic Literature Review for Extent of Resection and Recurrence. World Neurosurg 2018;110:276–83. https://doi.org/10.1016/j.wneu.2017.11.102.
- Salles D, Laviola G, Malinverni ACdM, Stávale JN. Pilocytic Astrocytoma: A Review of General, Clinical, and Molecular Characteristics. J Child Neurol 2020;35(12):852–8. https://doi. org/10.1177/0883073820937225.
- Amundson EW, McGirt MJ, Olivi A. A contralateral, transfrontal, extraventricular approach to stereotactic brainstem biopsy procedures. Technical note. J Neurosurg 2005;102(3):565–70. https:// doi.org/10.3171/jns.2005.102.3.0565.
- Matsuoka T, Yamada K, Matsuda Y, Kamite Y, Uozumi T. CT-guided stereotactic operation for cerebellar abscess by the transtentorial hiatus approach: a case report. No Shinkei Geka 1995;23(1):69–72.
- Montes JL, Clarke DB, Farmer JP. Stereotactic transtentorial hiatus ventriculoperitoneal shunting for the sequestered fourth ventricle. Technical note J Neurosurg 1994;80(4):759–61. https://doi. org/10.3171/jns.1994.80.4.0759.
- Aung TH, Kwok CK, Mak YF, Mak EG. Computed tomographyguided stereotactic aspiration and biopsy of a cystic metastatic adenocarcinoma of the pons. Hong Kong Med J 1997;3(2):232–5.
- Galanda M, Nádvornik P, Fodor S. Stereotactic approach to therapeutic stimulation of cerebellum for spasticity. Acta Neurochir Suppl (Wien) 1980;30:345–9. https://doi.org/10.1007/978-3-7091-8592-6_42.
- Garber ST, Riva-Cambrin J, Bishop FS, Brockmeyer DL. Comparing fourth ventricle shunt survival after placement via stereotactic transtentorial and suboccipital approaches. J Neurosurg Pediatr 2013;11(6):623–9. https://doi.org/10.3171/2013.3.PEDS12442.
- Turner MS, Nguyen HS, Payner TD, Cohen-Gadol AA. A novel method for stereotactic, endoscope-assisted transtentorial placement of a shunt catheter into symptomatic posterior fossa cysts. J Neurosurg Pediatr 2011;8(1):15–21. https://doi.org/10.3171/2011.4.PEDS10541.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.