Searching for an Ideal Sternal Osteosynthesis: Potential of the Novel Sternal Clips
by Stephan Raab, Evaldas Girdauskas, Sebastian Reindl*
Clinic of Cardiothoracic Surgery, University of Augsburg, Germany
*Corresponding author: Sebastian Reindl, Clinic of Cardiothoracic Surgery, University Hospital Augsburg, Faculty of Medicine, University of Augsburg, Germany.
Received Date: October 26, 2025
Accepted Date: November 06, 2025
Published Date: November 10, 2025
Citation: Raab S, Girdauskas E, Reindl S (2025) Searching for An Ideal Sternal Osteosynthesis: Potential of The Novel Sternal Clips. J Orthop Res Ther 10: 1408. DOi: 10.29011/2575-8241.001408
Glossary
DSWI Deep Sternal Wound Infection; CABG Coronary artery bypass grafting; AO/OTA Arbeitsgemeinschaft für Osteosynthesefragen/
Orthopaedic Trauma Association
Central Picture
Implantation of a two segment sternal clip: measurement, adjustment, bend around the sternum
Central Message
Sternal clips are suitable for osteosynthesis after sternal split operations, traumatic fractures and osteomyelitis oft he sternum
Perspective Statement
Sternal clips have the following advantages: The connection of the clip segments can counteract shear forces. Anchoring takes place completely around the bone and is therefore also suitable for osteomyelitis and osteoporosis. Retrosternal preparation is not necessary.
Graphical Abstract
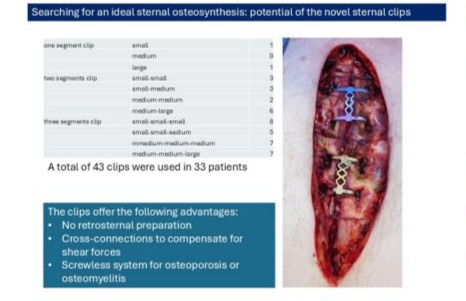
Figure 1: The sternum clips were used for the following indications: secondary closure of the sternum after DSWI, traumatic sternal fracture, sternal osteomyelitis. A total of 43 clips were used in 33 patients. There were no implant failures or serious complications.
Structured Abstract
Objective: We report on a novel clips system for sternal osteoynthesis. In contrast to previously reported sternal clips, these clips are connected to each other on up to three segments. We describe the use of this system for three different indications including primary sternal osteomyelitis, traumatic sternal fracture and secondary sternal osteosynthesis after deep sternal wound infection. Method and Results: A preliminary single-center feasibility study was conducted. The clips were used for three different indications, as described above. The clips were selected according to the sternal width and adjusted in individual length. Intraoperative variables and long-term effects were recorded. We aimed to define an appropriate clip for each specific indication. A total of 43 sternal clips were used in 33 patients between 6/2017 and 10/2024. The indications for the use of the sternal clips were secondary osteosynthesis after deep sternal wound infection (n=30), traumatic sternal fracture (n=2), osteosynthesis after syndesmosis infection (n=1). Two single clips, 14 twosegment clips and 27 three-segment clips were used. No material defects occurred during the follow-up. Osteosynthesis after traumatic horizontal sternal fractures and primary osteomyelitis of the syndesmosis were successful in all cases, without implantrelated complications. Discussion: The preliminary results of the novel clip system are promising. The potential advantage is the counteraction of the shear forces by the multi-segmental clips construct. They have advantage in patients with advanced osteoporosis and osteomyelitis. Dorsal preparation of the sternum is not necessary, which makes them easy to use for secondary osteosynthesis after deep sternal wound infection.
Keywords: Deep sternal wound infection; sternum osteomyelitis; sternum osteosynthesis; sternal clip; sternal fracture
Introduction
Sternal osteosynthesis has a wide spectrum of indications. The most common scenario is the osteosynthesis after median sternotomy. Sternal osteosynthesis after traumatic fractures is by far less common [1]. Although traumatic sternal fractures are quite common, as reported by the German hospital register of the Federal Statistical Office [2], the osteosynthetic treatment is not always necessary [3]. Osteosynthetic treatment is mostly considered in cases of secondary dislocation of the fracture or instability of the thorax [3]. A third indication might be the treatment of primary spontaneous osteomyelitis. This rare entity [4] is only mentioned in individual case reports. However, if surgical treatment is necessary, a bone defect with resulting instability should be addressed. Median sternotomy is the standard surgical access in heart surgery [5] that is usually closed using wires [6]. By using six to eight wires, the halves of the sternum are fixed together. Panduits can be used as a further development of wires [7]. These flat polymer bands are placed around the bone with a broader contact surface and without penetrating the sternum the established product line of the rib clips itself. Sternal clips are similarly placed around the bone, e.g. nitinol clips [8]. These clips are placed on the sternum and then clipped by means of thermal deformation in the intercostal areas. The novel sternal clips from MedXpert (Eschbach, Germany) presented here are the further development of sternal clipping systems. The novelty is that these clips are available in different combinations, i.e. as single, double and triple clips. This contribution comes from the established product line of the rib clips [9]. The individual clip segments can easily be fixed in the intercostal spaces around the sternum. The segment width is selected according to the width of the sternum, while the length of the clips is adapted to the distance between the intercostal spaces.
Patients
Most included patients had a deep sternal wound healing disorder after median sternotomy. The index sternal closure was performed using standard wires. Subsequently, sternal osteomyelitis was confirmed by histology and microbiology in all patients. The initial treatment was infection control by means of local negative pressure therapy and test-appropriate antibiotics. For the subsequent secondary sternal ostosynthesis we used sternal clips (Medxpert, Germany) and PDS cord (Ethicon, Johnson and Johnson, USA) in all patients. In some patients, the manubrium is too wide for the largest clip opening (Large) or forceps cannot be used at the caudal end of the corpus sterni due to the wide or vertical cartilaginous rib insertions. Titanium plates (SternaLock Blu, Zimmer Biomet, USA) were used in these cases.
Surgical Technique
The sternal clips were used according to the instructions for use and after instruction by Medxpert. First, the attachment of the pectoralis major muscle was detached from the chest wall on both sides at the sternal attachment up to 2 cm lateral to the sternum. The sternal incision surface was then freshened and straightened with the oscillating saw. Afterwards the two halves of the sternum were brought together. In preparation, the width of the sternum was first measured with the measuring instrument (Figure 2) and the respective clip width small, medium or large was selected for the segment. The 2- and 3-segment clips are available in different combinations of these 3 sizes:
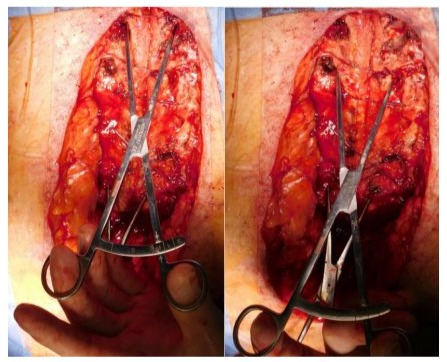
Figure 2: Measuring the width of the sternum to select the appropriate clip width.
Single clip
- Small
- Medium
- Large
- Small-Small
- Small-Medium
- Medium-Medium
- Medium-Large
- Small-Small-Small
- Small-Small-Medium
- Medium-Medium-Medium
- Medium-Medium-Large
Double clip
Triple clip
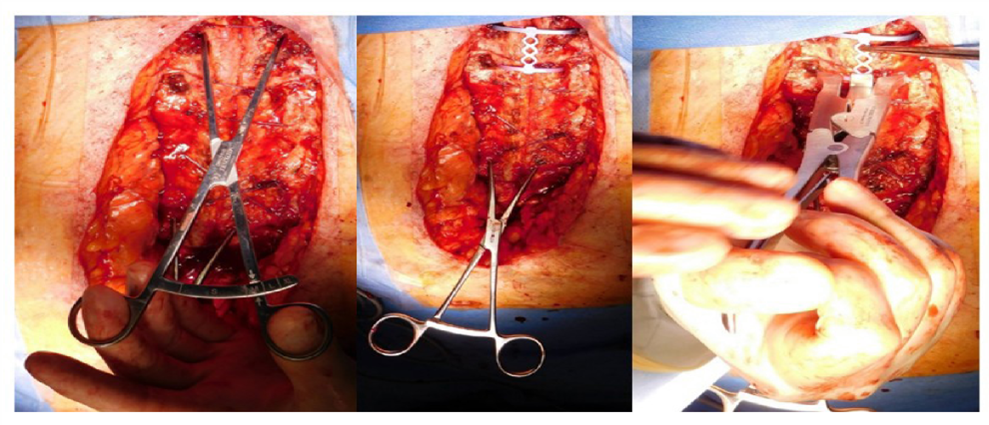
The combination of 2- and 3-segment clips was selected according to the measured sternal width. The clips were then adjusted in length according to the distances between the intercostal spaces (Figure 3). Bending of the clips was hardly necessary due to the anatomical characteristics of the sternum as a flat bone, but was carried out to a small extent for adjustment. For implantation, the sternal halves were brought into contact using reduction forceps. To hold the sternal halves in this position, PDS cords were inserted at the manubrium and costal arch. As sternal osteomyelitis was present, the PDS cords were not inserted through the sternum, but either into the cartilaginous part of the ribs or around the sternum. The intercostal spaces were then identified where a sternal clip could be inserted. The intercostal space was then incised directly on the periosteum of the sternum using the electrocautery.
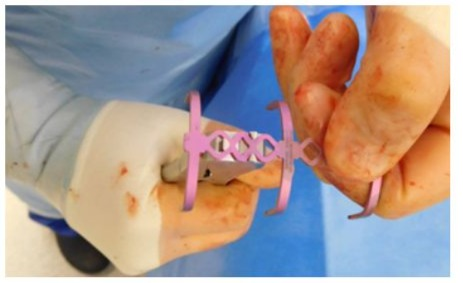
Figure 3: Adjusting the length of the three-segment clip to the individual intercostal distances.
The respective sternal clips were inserted after the adjustment described above and then the clip was pressed onto the sternum using the plier provided for this purpose and the segment bars were bent around the sternum. The individual bars were then fully bent around the sternum using the sternal clip final shaping forceps (Figure 4). The aim of sternal stabilization was to create at least 6 cross-connections between the two halves of the sternum. If this was not possible with the sternal clips alone, additional PDS cords were inserted. Titanium plates with locking screws were also available and used in 17 patients. When treating a sternal fracture with a sternal clip, the entire fracture gap was bridged with the clip.
The same applied to the treatment of a defect in the syndesmosis between the manubrium and corpus. If a bone defect had to be bridged, the procedure for adjusting the length of the sternal clips was modified. In this case, the clip was first inserted as described and clipped around the sternum. The length of the sternal clip was then adjusted using the corresponding shaping forceps. The resulting shortening leads to a shortening of the defect. Ideally, the respective bone ends should then stand on top of each other again.
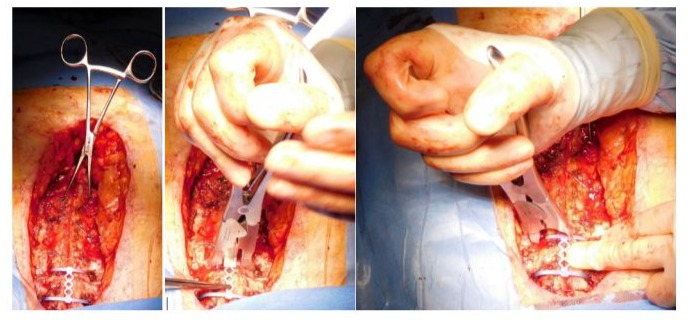
Figure 4: Inserting the clips with the two pliers.
Results
A total of 33 patients (30 after sternotomy with deep sternal wound healing disorder, 2 after sternal fracture, 1 after syndesmosis infection) were treated with 43 sternal clips between 6/2017 and 10/2024. Two patients had a traumatic sternal fracture (16.3.2.A AO/OTA classification of sternal fractures). One patient had a primary spontaneous infection of the syndesmosis between the manubrium and corpus sterni. In 30 patients, sternal clips were used for osteosynthesis after sternotomy. All patients had previously undergone heart surgery using the extracorporeal circulation, including CABG surgery (n=19), ascending aorta replacement (n=5), aortic valve replacement (n=3), combined CABG surgery and aortic valve replacement (n=3). The aim was always to insert at least 1 sternal clip, preferably a three-segment clip. This was achieved in all 30 patients (Figure 5). In 8 patients, an additional clip had to be inserted. In one patient, 3 double clips were used. As described previuosly, all patients received at least 2 PDS cords. In addition, a titanium plate was inserted in 17 patients (all patients with deep sternal wound infection). These were always positioned at the manubrium or the costal arch. The reason for such a titanium plate was: 1. the width of the manubrium that did not allow the clip implantation, 2. an insufficiently large intercostal gap at the level of the costal arch. The mean age of our study cohort was 63 ± 11 years, the gender distribution was 26 men and 7 women. The only inclusion criterion for the use of the sternal clip was an adequate bone quality allowing implantation of a sternal clip. All sternal clips were implanted at the University Hospital Augsburg, Clinic for Cardiac and Thoracic Surgery by 3 experienced surgeons.
The following one-segment, two-segment or three-segment clips combinations were used (Table 1):
|
One segment clip |
Small |
1 |
|
Medium |
0 |
|
|
Large |
1 |
|
|
Two segments clip |
Small-small |
3 |
|
Small-medium |
3 |
|
|
Medium-medium |
2 |
|
|
Medium-large |
6 |
|
|
Three segments clip |
Small-small-small |
8 |
|
Small-small-sedium |
5 |
|
|
Medium-medium-medium |
7 |
|
|
Medium-medium-large |
7 |
Table 1: Number and type of clips used
The implantation was uneventful for all patients. The two single clips were inserted in combination with a multi-segment clip. No clips had to be removed or repositioned. Of note, the clips enabled good bridging and stabilization of transverse sternal fractures and smaller bone defects, which typically may occur after disruption of the sternal wires. Clinically, all secondary osteosyntheses using the sternal clips were stable both intraoperatively and at the functional examination postoperatively. There were no serious complications. There were three minor intraoperative complications, such as bleeding from an intercostal vessel, which was stopped by electrocoagulation. One sternal clip became dislocated after the patient fell out of bed. At the same time, the PDS cords and a titanium plate, which was fixed by screws, tore out simultaneously. No fracture of the sternal clip was observed. In a total of five patients, the sternal clips were removed again due to persistent osteomyelitis. The causes for the removal were a persistent sternal infection in all cases, induced by the same microbiological pathogen. The interval between implantation and the removal was at least 6 weeks in all patients, so that the former osteotomy had become osseous in the meantime and the thorax was functionally stable. The explantation was possible without any problems in all five patients. The sternal clips were all still in their original position without any recognizable deformation or fracture.
Discussion
The use of wires for sternal osteosynthesis is considered a standard of care. It is quick to perform, has few complications and is costeffective. By using wires, the lateral forces on the rib cage can be sufficiently compensated. However, the shear forces are not sufficiently addressed by wires that are not connected to each other in most cases. The use of the figure of eight wire osteosynthesis could be a possible solution to address this drawback. Another disadvantage of the wire osteosynthesis is the fact that the bone is penetrated by the wire and the contact surface for the force distribution is very limited. This has a particularly negative effect in older female people with advanced osteporosis. There is a risk that the wire will tear through the bone tissue and lose its hold. To avoid this, Robbiczek has developed a special wiring method. However, this surgical technique may impair the blood supply to the sternum. There are several osteosynthesis systems available to overcome the limitation of wires. Sternal bands have a larger contact surface and, therefore, a superior force distribution. In addition, they are usually placed around the bone so that the bone does not have to be pierced and there is broad contact with the stable compacta. However, individual ligaments can also only cope poorly with shear forces along the osteosynthesis [10]. Alternatively, there are plates that are anchored in the bone with locking screws. These systems can absorb shear forces well as they have several anchor points on each half of the sternum. However, sufficiently firm bone tissue is required to fix the plates. A combination of both systems (ligament and plate) was also available. An ideal osteosynthesis system should fulfill the following requirements: a) the sternum should not be additionally injured during the osteosynthesis, b) there is a wide contact surface of the osteosynthesis to the bone that distributes the forces well; c) the system has several holding points that absorb shear forces; d) the osteosynthesis system can be customized; e) when implanting the osteosynthesis system, there is no necessity to dissect the dorsal side of the sternum which can be risky due to dence adhesions between the sternum and the heart or vascular structures (e.g., bypass graft).
All abovementioned requirements are addressed by the sternal clips. The main advantage of this system is the anchoring around the bone without perforating it with screws or wires. Furthermore, the system is suitable for bridging transverse fractures and smaller bone defects. Based on our preliminary experience in a limited consecutive patient’s series, the sternal clips are safe to use. An anatomical study has shown that the clips accomomodate well to the sternum in terms of length and available widths [11]. The fact that the clips can be adapted to the individual patient in terms of both the size of the opening (Small, Medium and Large) and their length has proven to be advantageous. The titanium can also be adapted to the shape of the sternum. When treating a sternal fracture with a sternal clip, the entire fracture gap must be bridged with the clip. This is only possible for 2-segment clips in the case of a horizontal fracture of the corpus sterni (AO/OTA 16.3.2.A) exactly between the intercostal spaces. For all other fractures, i.e. a horizontal fracture (AO/OTA 16.3.2.A) at the intercostal space or an oblique fracture (AO/OTA 16.3.2.B), a 3-segment clip must be inserted. Therefore, it is common sense that a 3-segment clip should always be used when treating fractures. The advantage of the sternal clip in the treatment of sternal fractures is also that the length of the clip can be adjusted again after implantation of the clip. By subsequently shortening the clip, further pressure can be applied to the fracture halves in the fracture gap. This procedure has proven to be very helpful for bridging bone defects.
However, the shortening option is limited to a few millimeters. Thus, this is sufficient for treating the defect after a Sydesmos defect or smaller bone defects after DSWI. The limitation of the sternal clip is that it can be very well implanted only on the corpus immediately caudal to the Angle of Lewis. It can be often successfully used on the manubrium in the first intercostal space, although the manubrium might be too wide for the largest opening (Large) of the clip to encompass it. Caudal to the corpus directly at the costal arch, implantation is often not possible due to the anatomical conditions. This is only possible if the ribs are still horizontal in this region. If the ribs and the associated intercostal clefts are already very steep, there is not enough space to insert the necessary bending pliers. This is also reflected by our findings; in sternal closure after median sternotomy, only 4 patients had 2 clips inserted at the same time. This is of course sufficient to counteract shear forces, but in order to achieve sufficient stability of the osteosynthesis, further osteosynthesis procedures must be used for the required 6 bridges between the two halves of the sternum. PDS cords have proven to be the optimal combination here.
To the best of our knowledge, our case series represent the largest experience published with the sternal clips. In this regard, no complications such as material breakage or surgery-associated complications occurred. As far as this retrospective analysis allows, the sternal clips described can be used safely and reproducibly within the described framework. In some indications such as osteomyelitis, osteoporosis or if retrosternal preparation is to be avoided, they may even be the first choice as an osteosynthesis procedure. The limitation is, however, the cost factor. In comparison with the wires, osteosynthesis plates or clips are more expensive. However, given the advantages and indications described above, individualized and patient-centered decision-making process is strongly appreciated.
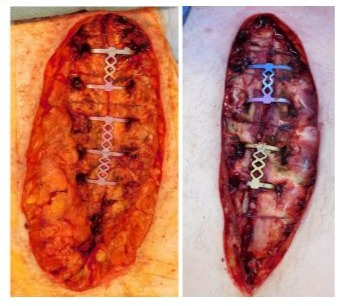
Figure 5: 2 examples of complete osteosynthesis with sternal clips after deep sternal wound infection.
References
- Brookes JG, Dunn RJ, Rogers IR (1993) Sternal fractures: a retrospective analysis of 272 cases. J Trauma 35(1): 46-54.
- Khoriati AA, Rajakulasingam R, Shah R (2013) Sternal fractures and their management. J Emerg Trauma Shock 6(2):113-116.
- Schulz-Drost S, Krinner S, Langenbach A, Oppel P, Lefering R, et al. (2017) Concomitant Sternal Fracture in Flail Chest: An Analysis of 21,741 Polytrauma Patients from the Trauma Register DGU®. Thorac Cardiovasc Surg 65(7): 551-559.
- Rodríguez Lorenzo P, Fernández Martínez B, Pérez Alba M, Ramírez Jaén C, Meana Morís AR, et al. (2023) Primary sternal osteomyelitis. Arch Argent Pediatr 121(5): e202201449.
- Gerbode F, Braimbridge MV, Melrose DG (1958) Median sternotomy for open cardiac surgery during total heart-lung by-pass. AMA Arch Surg 76(5): 821-824.
- Çiçek S (2018) Sternal closure: Wires are still the king. J Thorac Cardiovasc Surg 156(4): 1596-1597.
- Omer SJ (2018) Polymer cable tie closure of the sternum: Is it an acceptable fix? Thorac Cardiovasc Surg 156(4): 1611-1612.
- Reiss N, Schuett U, Kemper M, Bairaktaris A, Koerfer R (2007) New method for sternal closure after vacuum-assisted therapy in deep sternal infections after cardiac surgery. Ann Thorac Surg 83(6): 22467.
- Wiese MN, Kawel Boehm N, Moreno de la Santa P, Al Shahrabani F, Toffel M, et al. (2015) Functional results after chest wall stabilization with a new screwless fixation device. Eur J Cardiothorac Surg 47(5): 868-875.
- Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, et al. (2018) Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg 156(4):1589-1595.
- Reindl S, Schuller P, Meller M, Beyer M, Decker J, et al. (2022) Morphometry of The Sternum in Osteosynthetic Reconstruction. J Orthop Res Ther 7: 1242.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.