Sacculation of the Uterus: A Case Series and Review of the Literature
by Franziska Oelrich, Kimberly Van Ravenzwaay*, Peter Kollertz, Constanze Banz-Jansen
Clinic for gynecology and obstetrics, Protestant Hospital of Bethel Foundation, University Hospital OWL of Bielefeld University, Bielefeld-Bethel Campus, Burgsteig 13, 33617 Bielefeld, Germany
*Corresponding author: Kimberly van Ravenzwaay, Clinic for gynecology and obstetrics, Protestant Hospital of Bethel Foundation, University Hospital OWL of Bielefeld University, Bielefeld-Bethel Campus, Burgsteig 13, 33617 Bielefeld, Germany
Received Date: 24 September 2025
Accepted Date: 29 September 2025
Published Date: 01 October 2025
Citation: Oelrich F, Van Ravenzwaay K, Kollertz P, Banz-Jansen C. (2025). Sacculation of the Uterus: A Case Series and Review of the Literature. Ann Case Report. 10: 2423. https://doi.org/10.29011/2574-7754.102423
Abstract
Objectives: The purpose of this case series is to provide valuable insights for the examination of a retroverted uterus and the planning of delivery.
Case Series: Within one year our obstetrics unit had three different cases of incarceration and sacculation of a retroverted uterus. The first patient was a 33 year old primigravida diagnosed with a uterine sacculation due to a retroverted uterus caused by a fundal myoma at 20 weeks of gestation. A surgical correction or myomectomy was not considered during pregnancy as the patient did not report any clinical symptoms. The delivery was performed at 37+2 weeks of gestation through a midline incision cesarean section. The second patient was a 39 year old diagnosed late into the 3rd Trimester. Due to the advanced gestational age no further interventions were considered to correct the incarceration before delivery. For both patients the delivery was performed at 37+2 weeks of gestation through a midline incision cesarean section. The third patient was 28 years old and reported a high risk constellation of a previous operation, a previous retroflexed uterus and a twin pregnancy. An emergency laparotomy was performed due to a spontaneous rupture of the uterus.
Conclusion: The descriptions of these three cases show that there were severe differences in the fetal and maternal outcomes depending on the medical history of the patient. Therefore women with risk factors such as previous operations and especially previous retroverted uterus should be closely examined even in the first trimester. This is particularly important in the case of a twin pregnancy.
Keywords: Sacculation; Retroverted Uterus; MRI; Pregnancy; Incarceration
Introduction
Incarceration and sacculation of a retroverted uterus is a very rare complication that can occur during pregnancy. It is accompanied by clinical symptoms such as bladder emptying dysfunction, abdominal pain and constipation [1]. A prenatal diagnosis is essential for caesarean section planning as well as to prevent high fetal morbidity [2]. Despite the rarity of this complication, three different cases were experienced in our obstetrics unit within one year. In this case series we present those three cases occurring in two succeeding pregnancies, while one undiagnosed case ended in an intrauterine fetal death due to a spontaneous rupture of the uterus in the second trimester.
Case Presentation
All three cases have a German ethnicity.
First case: The first patient presented to our obstetrics unit was a 33 year old primigravida at 19+4 weeks of gestation with a known history of uterus myoma. The transabdominal ultrasound examination showed a fetus in the transverse position with normal fetal growth and no abnormalities in organ development. However the uterus appeared to be distorted by 180 degrees in transverse axis due to an extensive fundus myoma (13,5 x 11,5 x 10cm) which appeared to be fixated in the pouch of Douglas. The cervix was elongated and pulled up to the umbilicus (Figure 1).

Figure 1: Fibroid (on the right side), elongated cervix marked below the bladder, low lying placenta on the posterior wall (*)
An MRI-scan was initiated due to these findings for appropriate planning of delivery. The MRI scan was performed at 20 weeks of gestation. The magnetic resonance imaging confirmed the suspected sacculation of the uterus due to a large fundal myoma of approximately 14cm in diameter. Furthermore, placenta praevia was diagnosed. Both maternal kidneys showed mild hydronephrosis. Overall, the patient was diagnosed with uterine sacculation due to a retroverted uterus caused by a fundal myoma (Figure 2).
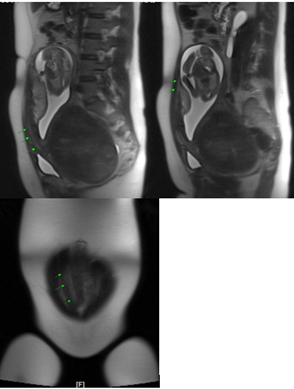
Figure 2: The arrows show the elongated cervix in the MRI scan, sagittal view (picture above), coronal view (picture below)
The patient returned to our clinic at 30+5 weeks of gestation for another examination and the appropriate planning of delivery through a caesarean section.
The patient did not report any kind of complaints throughout the pregnancy. The ultrasound presented a fetus in cephalic presentation. Fetal biometry, organ showed no abnormalities. A caesarean section was planned for 37+5 weeks of gestation. The possibility of myomectomy during the caesarean section had been discussed. It was agreed to attempt a myomectomy only if feasible of safety.
The patient was then admitted to our obstetrics unit at 37+0 weeks of gestation with circulatory dysregulation. Because of this, the caesarean section was performed at 37+2 weeks of gestation through a midline incision. After carefully identifying and delineating the bladder, a transverse uterine incision was made at the fundus underneath the myoma. A healthy male newborn (weight: 3285g; length: 54cm; APGAR 9/9/10 at 1, 5 and 10min, respectively; umbilical artery blood pH 7, 30) was delivered by breech presentation. The uterus was repositioned manually into its anatomical correct position. The previously described myoma now appeared to be larger than the remaining uterus. Thus a myomectomy was not performed. The puerperium was uneventful.
About 5 months postpartum, the patient was again presented to our clinic for laparoscopic myomectomy and adhesiolysis. The procedure was performed without any complications.
Second case: The second case was a 39 year old primigravida presented at 33 weeks of gestation with a twin pregnancy because of suspected complete placenta praevia. The pregnancy was achieved through ICSI treatment. The patient also presented with a medical history of extensive endometrioses, which had previously been treated through laparoscopy. The endometrioses had also affected the vagina and rectum.
Ultrasound examination showed normal fetal growth with normal amniotic fluid volume for both fetuses. Also the examination revealed an unusual elongation of the cervix. A previous scan at 13 weeks of gestation revealed a normal length of cervix and a suspected posterior placenta. The 22-week scan then showed an already elongated cervix with a retroflected uterus.
Now at 33 weeks of gestation the cervix appeared with a length of more than 9 cm. A cranial demarcation through ultrasound was not possible.
An MRI-scan was then performed for further diagnostic purposes due to suspected uterine sacculation due to adhesions in the lower abdomen caused by previous surgery. The MRI findings showed an elongated cervix (9cm), ventral presentation of the lower anterior uterine segment and a placenta praevia.
After confirmation of the diagnosis of uterine sacculation due to a fixed retroverted uterus a delivery by midline laparotomy caesarean section was planned. The caesarean section was performed at 37+2 weeks of gestation. The abdomen was entered through a midline incision. The uterus appeared incarcerated with an extremely elongated cervix. After identifying the uterine fundus, a transverse uterine incision was performed there to avoid an accidental incision into the cervix. First a healthy male newborn (weight: 2710g; length: 51cm; APGAR scores of 8/9/10 at 1, 5, and 10min; umbilical artery blood pH 7, 27) was delivered from breech position, followed by the delivery of a second healthy male (weight: 2610g; length: 49cm; APGAR scores of 8/8/10 at 1, 5, and10min; umbilical artery blood pH 7, 28) also from breech position. The postoperative course was uneventful.
Third case: About 8 months after the second case a 28 year old gravida 4 para 2 was admitted to our emergency unit due to severe persistent abdominal pain in 16+1 weeks of gestation in a twin pregnancy. In her medical history she reported two previous caesarean sections and a surgical antefixation of the retroflected uterus.
The initial ultrasound examination showed two vital fetuses in utero. Furthermore intra-abdominal free fluid was detected. During the vaginal examination the fundus of the uterus was palpable while the cervix was anteriorly displaced behind the pubic symphysis (Figure 3).

Figure 3: Transvaginal view of the elongated cervix (picture above *), intra-abdominal hematoma (Picture below *), and cervix (#)
As there was no certain cause for the severe symptoms presented, an emergency MRI was performed. Due to severe pain and nausea the patient was not able to endure the whole scan. Thus the scan had to be stopped prematurely. As far as assessable the MRI showed an inhomogeneous mass (10x5cm) enclosed to the uterus. This was suspected to be a hematoma. Also a great amount of intraabdominal free fluid was revealed. Combining these findings with the known medical history of the patient a spontaneous uterine rupture had to be suspected. An emergency laparotomy was immediately performed as the patient was also showing signs of hemorrhagic shock.
Upon entering the abdominal cavity an abundant amount of blood was drained. The bleeding site was immediately identified as a ruptured anterior wall of the uterus. Placental tissue was already pouring into the abdomen. Due to the severe bleeding, placental abruption and premature rupture of membranes the fetuses were non-viable and were delivered stillborn.
The fundus of the uterus appeared to be incarcerated into the pouch of Douglas causing a uterine sacculation. A reason for the incarceration could not be identified. The uterine rupture appeared over the whole length of the previous uterine incision in the caesarean section (Figure 4).

Figure 4: Intraoperative view of the ruptured cesaerian scar
The uterus was repositioned while the blood loss accumulated to about 1500 ml. The following postoperative course was uneventful.
The patient was strongly advised to avoid another pregnancy.
Discussion
The incarceration and sacculation of uterus can have a devastating impact on pregnancy and can cause a variety of complications such as abortion, fetal death, uterine rupture, intrauterine growth restriction and preterm labor. Due to the rare occurrence - 1 in 3000 pregnancies [3] and unspecific symptoms such as dysuria, back pain, constipation, vaginal bleeding, pelvic pain and urinary retention the diagnosis is difficult to obtain. It has been described that most cases were diagnosed by pelvic examination and ultrasound. An MRI, however, seems required to confirm the anatomical abnormalities.The main risk factors are leiomyoma, previous operation, previous retroverted uterus, endometriosis, pelvic adhesions, adenomyosis, deep sacral concavity and STD [4].
In case number one the patient was diagnosed with a uterine sacculation due to a retroverted uterus caused by a fundal myoma at 20 weeks of gestation. A surgical correction or myomectomy was not considered during pregnancy as the patient did not report any clinical symptoms. Furthermore the patient had no previous surgeries in her medical history. The second patient was diagnosed late into the 3rd Trimester. Due to the advanced gestational age no further interventions were considered to correct the incarceration before delivery. Thus it appeared justifiable in both cases to plan an elective caesarean for 37+2 weeks of gestation.
The patient in case number three reported a high risk constellation of a previous operation, a previous retroflexed uterus and a twin pregnancy. As retroversion occurs in 11-19% of women at the time of conception and rarely persists after 14-16 weeks no further management had been considered this early into her pregnancy [5]. The findings in ultrasound and MRI could have led to consideration of correcting the retroflexed uterus through either non-invasive or surgical methods to reduce the risk for complications. This special case in a twin pregnancy shows that because the uterine size is bigger than that of a singleton case, the complications related to the sacculation uterus occur at an earlier gestational age than those of sacculation uterus cases with singleton pregnancies [6-8].
Conclusion
In conclusion, the descriptions of these three cases show that there were severe differences in the fetal and maternal outcomes depending on the medical history of the patient. Therefore women with risk factors such as previous operations and especially a previous retroverted uterus should be closely examined even in the first trimester. This is particularly important in the case of a twin pregnancy. Supplementary it should be considered to perform further diagnostic measures in the second trimester if a uterine incarceration is suspected in a patient with those risk factors.
Declarations
Ethics approval and Consent to participate: All data and images in the manuscript are anonymized so that they cannot be traced back.
Conflict of Interest: The authors declare that there was no conflict of interest
Funding: The authors declare that no funds, grants, or other support was received during the preparation of this manuscript.
Author Contributions
Franziska Oelrich: manuskript writing, data management, data analysis and literature research.
Kimberly van Ravenzwaay: manuskript editing/writing and literature research.
Dr. med. Peter Kollerz: data collection and data analysis.
Prof. Dr. med. Constanze Banz-Jansen: project development/ overview and manuscript editing.
All authors read and approved the final manuscript.
References
- Schmidt S, Köhler W, Brucker C. (2019). Sakkulation des Uterus als Risikofaktor in der Schwangerschaft. Gynäkologe. 52: 229-232.
- Linder N, Tauscher A, Borte G. (2015). Die Sakkulation des Uterus – Eine seltene, aber bedrohliche Komplikation in der Schwangerschaft. RöFo. 187: 57-58.
- Gottschalk EM, Siedentopf JP, Schoenborn I, Gartenschlaeger S, Dudenhausen JW, et al. (2008). Prenatal sonographic and MRI findings in a pregnancy complicated by uterine sacculation: case report and review of the literature. Ultrasound Obstet Gynecol. 32: 582-586.
- Kim YS, Kwon BS, Lee YJ. (2021). Clinical approach and management of uterine incarceration according to trimester of pregnancy: Case report and literature review. Taiwan J Obstet Gynecol. 60: 911-915.
- Van der Tuuk K, Krenning RA, Krenning G, Monincx WM. (2009). Recurrent incarceration of the retroverted gravid uterus at term - two times transvaginal caesarean section: a case report. J Med Case Rep. 3: 103.
- Tong C, Wang Y, Liu Z, Zhao Y, Xu Y, et al. (2019). Spontaneous reduction of an incarcerated gravid uterus after myomectomy in the second trimester: A case report. Medicine (Baltimore). 98: 1-4.
- Heilenkötter U. (2018). Fixierte Retroflexio uteri bei fortgeschrittener Schwangerschaft: Verlauf der Kaiserschnitte bei zwei Patientinnen mit Achsenumkehr der Gebärmutter. Frauenarzt. 59: 558-559.
- Faber R, Stepan H. (2017). Sonografische Beurteilung des unteren Uterinsegments in der Schwangerschaft. Frauenarzt. 58: 825-834.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.