Rare Case of Urachal Mucinous Low-Grade Neoplasm with Bladder Infiltration: A Case Report
by Anja Kortenhorn1*, Ruth Himmelsbach1, Kosmas Kandilaris2, Christian Gratzke1, Cordula A Jilg1
1Department of Urology, Medical University Center, Freiburg, Germany
2Department of Pathology, Medical University Center, Freiburg, Germany
*Corresponding Author: Anja Kortenhorn, Department of Urology, Medical University Center, Freiburg, Germany
Received Date: 04 February 2026
Accepted Date: 09 February 2026
Published Date: 11 February 2026
Citation: Kortenhorn A, Himmelsbach R, Kandilaris K, Gratzke C, Jilg CA. (2026). Rare Case of Urachal Mucinous Low-Grade Neoplasm with Bladder Infiltration: A Case Report. Ann Case Report. 11: 2526. DOI: https://doi.org/10.29011/2574-7754.102526
Abstract
Low-grade mucinous neoplasms originating from the urachus are extremely rare, with less than 30 reported cases to date. When left untreated, ruptures of cystic masses may lead to intraperitoneal spread causing pseudomyxoma peritonei (PMP). In this case report a 59-year-old patient presented with recurrent swelling of the right groin after enucleation of an indeterminate cystic mass had been performed at an external hospital three months prior. Imaging revealed a tumorous mass with suspected bladder infiltration. More common primary sites of mucinous tumours such as the GI tract as well as intraperitoneal spread had been ruled out preoperatively. Complete surgical removal of the mass including partial cystectomy was performed. The procedure was technically challenging due to extensive unusual ossification of the anterior abdominal musculature resulting from a work accident with symphyseal disruption, yet primary wound closure was achieved. Tumour recurrence was observed three months following initial incomplete resection, which highlights the importance of early diagnosis and proper treatment including radical complete surgical removal, ideally without opening the lesion, to optimize outcome. This report adds to the limited literature on low-grade mucinous neoplasms presenting with extraperitoneal manifestation and urinary tract involvement, emphasizing diagnostic challenges and the need for multidisciplinary management.
Keywords: Case Report; Urachus; Mucinous Cystic Tumour Of Low Malignant Potential; Urachal Tumour; Mucin-Producing Urachal Tumour; Urachal Cystic Neoplasm.
Introduction
Low-grade mucinous neoplasms are rare tumours characterized by slow growth and mucin production, most commonly arising in the appendix, less frequent in the ovaries or the pancreas [1,2] or, in rare cases, also originating from the urachus [3]. Although these neoplasms typically remain localized, they may occasionally spread via local invasion or peritoneal dissemination. Rupturing or perforating tumours may lead to a spread of mucin and neoplastic cells within the peritoneal cavity, creating a clinical syndrome marked by mucinous ascites and mucinous implants within the peritoneal cavity, called pseudomyxoma peritonei (PMP) [4,5]. PMP can be associated with high morbidity and mortality, as the disease shows progressive but mostly indolent dynamic with the possibility of intestinal obstruction and malnutrition [6].
Clinical presentation may vary from asymptomatic to lower abdominal pain, indolent swelling or symptoms of PMP such as abdominal distention [2]. Treatment regimens focus on complete resection or in case of PMP cytoreductive surgery and may be complimented by hyperthermic intraperitoneal chemotherapy (HIPEC) [7].
Methods
Care was provided at university hospital of Freiburg, Germany. The patient provided written consent for a review of medical records and for publication of a case report, in accordance with institutional policy. Data regarding clinical history, diagnostic imaging, and pathology were collected retrospectively.
Case Presentation
A 59-year-old male patient presented with indolent recurrent swelling in the right groin region. Three months prior, enucleation of an indeterminate cystic mass had been performed at an external clinic following sonographic and MR imaging regarding a localized swelling. External histopathological examinations suggested plenty of extracellular mucin matching the appearance of PMP.
Upon presentation, physical examination revealed a localized swelling reaching from the symphysis to the right groin into the right scrotum (Figure 1). Repeated cross-sectional imaging showed no sign of intraperitoneal involvement. In the region of the former tumour bed (external surgical procedure), imaging revealed a polylubulated cystoid lesion reaching from the ventral bladder wall to almost skin level with suspect invasion of the bladder, interpreted as either early recurrence or remaining tumour material (Figure 2 A-C).

Figure 1: Preoperative swelling of the lower right abdomen and right hemiscrotum.
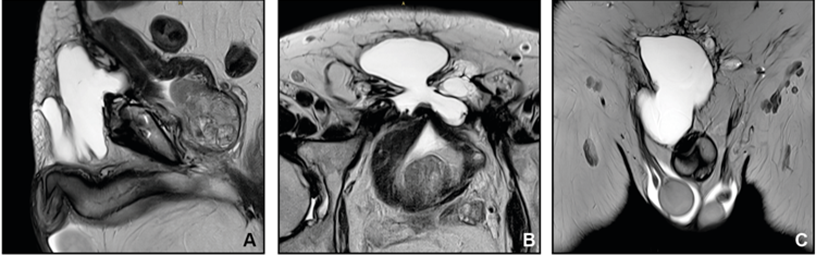
Figure 2: Preoperative MRI in sagittal (A), axial (B) and coronal (C) plane showing a multilobulated cystoid lesion extending from the ventral bladder wall to almost skin level with suspected invasion of the bladder.
In search of a possible primary lesion diagnostic workup was complemented by colonoscopy, gastroscopy and cystoscopy. No pathological findings were identified. The appendix, as the most common origin of mucinous tumours leading to PMP, had been removed several decades prior due to acute appendicitis, without abnormal pathological findings.
At the time of surgery, there was no evidence of PMP or other metastatic lesions. A multicompartmental tumour resection was performed, extending from the presymphyseal area to the right hemiscrotum, with retrosymphyseal involvement. Intraoperatively, the tumour was found to have pronounced adhesions to the right spermatic cord. As preoperative imaging suggested, a porous could be followed to the anterior wall of the urinary bladder, necessitating a partial cystectomy of approximately 1–2 cm (Figure 3). The cystic tumour mass was filled with mucinous material, which was evacuated in a controlled manner without spillage of mucinous material. Above the rectus fascia, a bone-like scar tissue was found measuring approximately 5x3cm, most likely a result of operation after a work accident with symphyseal disruption several years ago. This accident resulted in bladder dysfunction requiring intermittent self-catheterization. This defect complicated coverage and wound closure, yet primary wound closure was achievable (Figure 4). The peritoneum remained intact and was not opened at any point during the procedure.
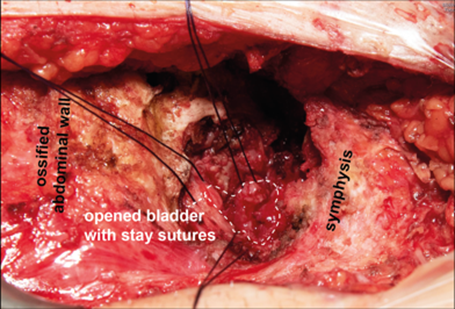
Figure 3: Intraoperative situs after tumour resection showing the defect in the ventral bladder wall marked with stay sutures and ossified scarring tissue.

Figure 4: Primary wound closure with two Redon drains complicated by scar tissue as shown in Figure 3, but ultimately achieved without high tension through Donati sutures.
Histopathological analysis revealed an intestinal glandular proliferation with mild architectural atypia and extracellular mucinous deposits in fibroadipose connective tissue (Figure 5). Molecular pathological analysis identified a GNAS hotspot variant (p.R201H) corroborating the diagnosis of a low-grade mucinous neoplasia. Considering the localization of the lesion and preoperative imaging without signs of intraperitoneal involvement, urachal origin was deemed most likely.
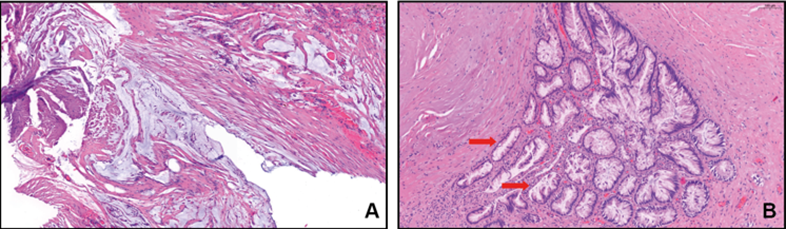
Figure 5: Histopathological images showing (A) local mucinous deposits in fibrosed fatty and connective tissue and (B) intestinal glandular epithelia with mild architectural atypia. Arrows indicate folding of the epithelium with slight nuclear stratification.
On postoperative day seven, following a normal cystogram confirming bladder integrity, intermittent self-catheterization was resumed. Despite the challenging wound closure, primary wound healing was satisfactory (Figure 6). Short-term follow-up revealed a postoperative seroma, but no evidence of early recurrence of mucinous structures. Ongoing surveillance will be conducted through short-term cross-sectional imaging.

Figure 6: Primary wound healing of the incision in the lower abdomen on postoperative day 14 with all sutures removed.
Discussion
This report presents a case of a mucinous tumour infiltrating the bladder with features of low malignant intestinal neoplasia. Considering the localization und preoperative rule out of other possible primary sites, the lesion most likely originated from the urachus. Mucinous Cystic Tumours of Low Malignant Potential (MCTLMP) arising from the urachus are exceptionally rare and diagnostically challenging [2,5]. Urachal tumours in its entirety account for only <1% of bladder cancers [8]. Urachal neoplasms can be further divided into glandular and non-glandular neoplasms. Glandular neoplasms have been compared and classified similarly to glandular lesions of the ovaries [9]. To date, less than 30 cases of low grade mucinous neoplasms of the urachus have been reported, highlighting the rarity and uncertainty associated with this entity [2,3].
Neoplasms with low-grade malignant features usually do not show invasive behaviour. In this case bladder invasion can be explained by the anatomic localization. The urachus is an embryonic remnant connecting the anterior bladder wall to the umbilicus, which allows tumour growth originating from the urachus to extend into the bladder wall. Urachal MCTLMP most commonly arise from these urachal remnants but may also arise de novo from the bladder mucosa itself [2]. While in this case the scarring tissue after the work accident complicated the surgical procedure, causal connection to development of the cystic low-grade neoplasm seems unlikely.
Clinical presentation can range from a completely asymptomatic incidental finding to localized swelling, lower abdominal pain or mucinous urinary secretion [2]. In rare cases, even low-grade malignant mucinous cystic neoplasms can rupture into the peritoneal cavity, and cause PMP. So far, there have been 4 reported cases of PMP caused by urachal MCTLMP [3,5]. Thus, early diagnostic and treatment is essential, and lower abdominal cystic masses in the absence of an appendiceal or colonic origin should raise suspicion for urachal origin [6,10]. Therapeutic strategies are currently based on the recommendations for mucinous neoplasms of the appendix due to the low number of cases and include complete surgical excision and, in the case of PMP, cytoreductive surgery and HIPEC. However, given the unusual anatomical location, individualized treatment approaches need to be considered [3]. Whenever feasible, complete surgical removal should be pursued for long-term remission free survival. As this case study shows, incomplete resection can lead to early recurrence.
Conclusion
Experience in diagnostic evaluation and therapeutic management of cystic urachal neoplasms remains sparse due to their rare occurrence. Early diagnosis and complete surgical removal are essential in preventing complications and progression such as PMP. Despite their rare occurrence, urachal neoplasms should be considered in differential diagnosis of lower abdominal cystic lesions. At this stage, therapeutic approaches must be developed on a case-by-case basis, tailored individually for each patient.
Declarations
Contributors: All authors contributed to planning, literature review, and conduct of the review article. All authors have reviewed and agreed on the final manuscript.
Competing interests: None.
Patient consent for publication: Informed consent was obtained from the patient, consent form available upon request.
Ethics approval and consent to participate: Not required.
Availability of data and materials: Not applicable.
Funding: No Funding.
References
- Lu C, Embel VK, Fox ME, Donne R, Parker GS. (2024). Diagnostic uncertainty and management of low-grade appendiceal mucinous neoplasm-a case report and review of the literature. J Surg Case Rep 2024: rjae717.
- Schmeusser B, Wiedemer J, Obery D, Buckley K, Yu M. (2022). Urachal mucinous cystic tumor of low malignant potential in a polymorbid female: A case report and review of the literature. Int Cancer Conf J 11: 104–108.
- Behrenbruch C, Moran B. (2024). Pseudomyxoma peritonei originating from low-grade mucinous neoplasm of the urachus. ANZ J Surg 94: 755–756.
- Bignell M, Carr NJ, Mohamed F. (2016). Pathophysiology and classification of pseudomyxoma peritonei. Pleura Peritoneum 1: 3–13.
- Chen L, Di M, Sun L, Fu Q. (2023). Rare urachal mucinous cystic tumor of low malignant potential with peritoneal pseudomyxoma: A case report. Exp Ther Med 26: 555.
- Allievi N, Samuel VM, Carr N, Shah N, Di Fabio F, et al. (2023). Pseudomyxoma peritonei arising from urachal mucinous neoplasms: A case series and updated literature review. Indian J Surg Oncol 14: 144–150.
- Shringi S, Agrawal AK, Gadkari P. (2024). A review of pseudomyxoma peritonei: Insights into diagnosis, management, and prognosis. Cureus 16: e61244.
- Paner GP, Lopez-Beltran A, Sirohi D, Amin MB. (2016). Updates in the pathologic diagnosis and classification of epithelial neoplasms of urachal origin. Adv Anat Pathol 23: 71–83.
- Amin MB, Smith SC, Eble JN, Rao P, Choi WWL, et al. (2014). Glandular neoplasms of the urachus: A report of 55 cases emphasizing mucinous cystic tumors with proposed classification. Am J Surg Pathol 38: 1033–1045.
- Brennan K, Johnson P, Curtis H, Arnason T. (2019). Urachal mucinous cystic tumor of low malignant potential with concurrent sigmoid colon adenocarcinoma. Case Rep Gastrointest Med 2019: 1434838.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.