Public Perception and Practice of Type-II Diabetes Mellitus in Bisha Province: A Cross-Sectional Study
by Partha Nandi1*, Huthayfah Abdullah K Alghamdi2, Mansour Abdullah S Alghamdi2, Faisal Saeed H Alghamdi2, Mohammed Falah M Almuawi2, Mohammed Turki M Almuawi2, Talal Mohammed S Alqarni2, Ziyad Mohammed S Alqarni2, Abdullah M Alshahrani3, Mufarrah H Alharthi3, Abdullah Alhalafi4, Shehab Almalki5, Ibrahim Awad Aljack4, Abubakar M Jibo4, Kamal Eldin Elhassan3
1Professor of Family and Community Medicine, University of Bisha College of Medicine, Kingdom of Saudi Arabia
2MBBS students (Year 6), University of Bisha College of Medicine, Kingdom of Saudi Arabia
3Associate Professor of Family and Community Medicine, University of Bisha College of Medicine, Kingdom of Saudi Arabia
4Assistant Professor of Family and Community Medicine, University of Bisha College of Medicine, Kingdom of Saudi Arabia
5Lecturer of Family and Community Medicine, University of Bisha College of Medicine, Kingdom of Saudi Arabia
*Corresponding author: Partha Nandi, Professor of Family and Community Medicine, University of Bisha College of Medicine,
Kingdom of Saudi Arabia
Received Date: 17 October, 2025
Accepted Date: 25 October, 2025
Published Date: 29 October, 2025
Citation: Nandi P, Alghamdi HA, Alghamdi MA, Alghamdi FS, Almawi MF, et al. (2025) Public Perception and Practice of Type-II Diabetes Mellitus in Bisha Province: A Cross-Sectional Study. J Community Med Public Health 9: 537. https://doi.org/10.29011/2577-2228.100537
Abstract
Background and aim: There is a rapid increase in the number of people with type II diabetes and its complication worldwide with many preventable cases. The current project aimed to raise the knowledge, attitude and practice toward diabetes mellitus (DM) and its complications among general population of Bisha province. Methodology: A cross-sectional study was conducted among Bisha residents between (22nd-27th January 2024). Results: The descriptive statistics were represented with frequencies, percentages, and charts. Chi-square test was used to find association between categorical variables. The study showed that 55% of them have a positive knowledge, and 75% show good practice, but most of them show poor attitude (36.3%). These variables have association with age group. There was no significant association between attitude and gender or education level (p=0.722 and p=0.562) in contrast to knowledge and practice. Conclusion: In Bisha province the knowledge, attitude and practice toward Diabetes mellitus type 2 (T2DM) and its complications is linked to age group.
Keywords: Type 2 diabetes mellitus; Complication
Introduction
Diabetes Mellitus (DM) has become a global health crisis, affecting millions of people worldwide. As a chronic metabolic disorder, DM can significantly impact patients’ quality of life and increase their risk of developing other diseases [1]. In 1979, the National Diabetes Data Group produced a consensus document standardizing the nomenclature and definitions for diabetes mellitus. This document was endorsed one year later by WHO. The two major types of diabetes mellitus were given names descriptive of their clinical presentation: “Insulin-Dependent Diabetes Mellitus” (IDDM) and “Non-Insulin-Dependent Diabetes Mellitus” (NIDDM) [2].
The classification system for diabetes mellitus has evolved over time, with the current system identifying three main types: type 1, type 2, and gestational diabetes [3].
Type 2 diabetes mellitus (T2DM) is considered a major public health concern as an epidemic with considerable number of premature deaths, disabilities, high morbidity, and mortality rates [4]. The incidence of T2DM has tremendously increased globally in the last 20-30 years [5]. Diabetes symptoms might appear suddenly. Type 2 diabetes symptoms might be subtle and take years to become apparent. These symptoms of diabetes include feeling very thirsty, needing to urinate more often than usual, blurred vision, feeling tired, losing weight unintentionally. Type 2 diabetes contributes more than 95% of those who have the disease. This kind of diabetes was only diagnosed with adults until recently, but it is now increasingly happening in children as well [6].
Complications associated with T2DM include hypoglycaemia, hyperosmolar hyperglycemic state, diabetic ketoacidosis, retinopathy, nephropathy, neuropathy, and cardiovascular events [4]. The primary aim of management of DM is to delay the macro and microvascular complications by achieving optimal glycaemic control. This involves lifestyle modification, including regular exercise, healthy diet and weight loss, and drug therapy [7]. With almost seven million diabetic patients, Saudi Arabia is regarded as one of the nations with the highest rates of diabetes [6].
Many issues may arise from long-term type 2 diabetes. A microvascular condition known as diabetic retinopathy can impact one or both of the macula and peripheral retina. For diabetics, it is a leading cause of blindness and vision loss. It can be segregated into two kinds “Proliferative Diabetic Retinopathy” (PDR) and “NonProliferative Diabetic Retinopathy”(NPDR) [8]. The retinopathy characterized by blurred vision, sudden shower of black “floaters” (black or grey specks or strings) in vision, fluctuating vision and dark or empty areas of vision [9]. Nephropathy, a chronic consequence of both types of diabetes mellitus, is defined by decreased kidney Glomerular Filtration Rate (GFR) or increased urine albumin excretion (proteinuria) [8].
This study aims to assess the knowledge, attitude and practice toward type II diabetes and its complication among general population in Bisha province. Although the Type 2 DM is a wellknown disease among all the age groups (as per the previous studies) still the prevalence is very high in KSA (>30%) and is projected to be even higher in near future if the same trend of lifestyle among general population, on average, continues. Hence the study intends to find the reason for such higher percentage of prevalence across all age groups. The findings may assist diabetic people live better lives, lessen the stress on their families, and prevent or limit the risk of complications.
Methodology
Study design
This was a cross-sectional questionnaire-based study. Participants were included with informed consent to participate after they were given full details of the study and its intended aims. The questionnaire was designed in English and then translated to the local spoken language Arabic by proficient speakers of both languages and was revised to be suitable to the general population.
Sampling strategy
Non-randomized convenient sampling was adapted.
Calculating sample size
The following formula is used to determine the sample:


n = The minimum sample size = 207
P = is the proportion of people with good awareness = (p = 0.84) [1].
q = (1- P) = Complimentary probability (1-0.84) = 0.16 d = is the degree of accuracy = 0.05
z = the standard normal deviate value corresponding to 95% confidence interval = 1.96
Data collection
A well-structured, vetted and piloted self-administered online questionnaire used in the current study, which was developed to evaluate the participant’s KAP regarding diabetes and its complication. The questionnaire contained four sections. The first section collected demographic information about the participants. The second section contained questions about knowledge of DM and its complications. The third section collected information about their general attitude toward diabetes. The last section collected information about the practices of participants toward disease and its complication.
Study population (inclusion and exclusion)
The participants for the study were included based on following inclusion and exclusion criteria, such as population who were ≥12 years of age and those who reside in Bisha were included as study participants. And those who were less than 12 years old, did not consent to participate and those who don’t reside in Bisha were excluded from the study.
Data analysis
Data were collected on a google form and entered on a Microsoft Office Excel® (2019) spreadsheet. Statistical data analysis and tables were generated using Microsoft Office Excel® (2019). A Chi-squared test was used to test for significance with the help of IBM SPSS software version 29, and a priori level of p<0.05 was considered statistically significant.
Ethical approval
Upon submission of full project proposal and consent forms made to the Research Ethics Local Committee at the College of medicine, University of Bisha in the Kingdom of Saudi Arabia. The research has been approved on Wednesday 22nd May 2024. The reference number: UB-RELOC H-06-BH-087/ (1508.24).
Results
This table shows the sociodemographic factor of our sample. As shown, most age groups participate in this study are from (above 18-30). The number of males less than the female number. It shows that those who have bachelor’s or diploma have the highest rate of all participants. Most of the participants live in Bisha city (urban) while only 15% live in villages. According to those having diabetes, they make up only 10.6% of all participants.
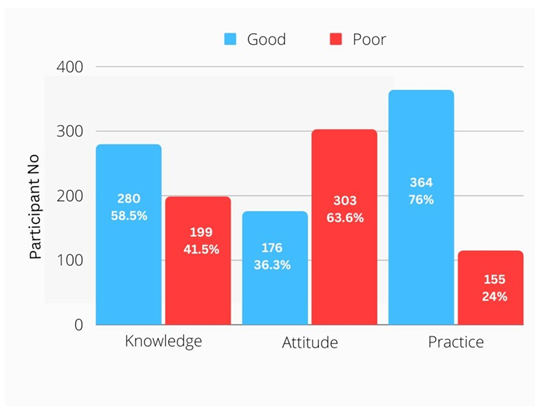
Figure 1: Subjects Levels of knowledge, attitude and practice toward type 2 diabetes and it’s complication.
This figure demonstrates the percentage of good and poor knowledge, attitude and practice. Of them 54% show good knowledge, and only 36.3% have good attitude. Interestingly, most of them have positive practice toward the disease (76%).
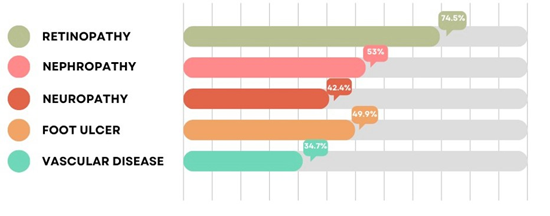
Figure 2: Subjects Levels of knowledge of complication of diabetes type 2.
This figure describes the percentage of knowledge of complication. In our sample most of them chose the retinopathy as a complication, while the vascular disease was the least one chosen. This above table explain the relationship between knowledge and sociodemographic factors. It shows that the age and education have significant relation with knowledge. according to gender, living area or having diabetes or not there is no significant relation.
In this table, age only shows association with attitude. The most common age group has good attitude is from above 18-30. The gender, education, living area or whoever has diabetes show no association. This table explain the association of practice with socio-demographic factors. Most of these factors have a significant relation. The highest one is age which have highly significant relation as shown in the table above. The gender or living area show no significant. The education or having diabetes also have a significant.
Discussion
A total of 479 questionnaires were collected in this study. Approximately, 85% of the respondents were from Bisha urban region (407), of whom 248 were females (51.8%) compared to 231 males (48.2%), with many of the respondents in the 18-30 years’ age group (33.6%). Interestingly, the respondents recorded close to 60% for both their educational background, completed high school and above. The characteristics of the studied population are shown in Table 1.
|
Characteristics |
Category |
n (479) |
Percent (%) |
|
Age |
12-18 years |
60 |
12.5 |
|
Above 18-30 years |
161 |
33.6 |
|
|
31-40 years |
79 |
16.5 |
|
|
41-50 years |
85 |
17.7 |
|
|
51-60 years |
73 |
15.2 |
|
|
Above 60 years |
21 |
4.4 |
|
|
Sex |
Male |
231 |
48.2 |
|
Female |
248 |
51.8 |
|
|
Education |
Primary |
5 |
1 |
|
Intermediate |
24 |
5 |
|
|
High school |
114 |
23.8 |
|
|
Bachelor’s Degree\Diploma |
309 |
64.6 |
|
|
Postgraduate |
26 |
5.4 |
|
|
Residence |
Bisha city |
407 |
85 |
|
Bisha village |
72 |
15 |
|
|
Have diabetes |
Yes |
51 |
10.6 |
|
No |
428 |
89.4 |
Table 1: Sociodemographic distribution of the study population.
Among our sample, 280 (58.5%) had good knowledge scores, while 199 (41.5%) had poor knowledge scores. In comparison to a study conducted in Pakistan, the knowledge rate was close to 47% in Pakistan [10]. While in another study conducted in Riyadh only 16.9% had good knowledge about type 2 diabetes and its complications [12]. In the attitude, 176 (36.3%) participants had positive scores indicated positive attitudes, while 364 (63.6%) had negative scores indicated negative attitudes. Our sample’s attitude was close to people’s attitude in study conducted in Jordan, where it was 46.4% of good attitude [11]. Interestingly, more than half of the participants, 364 (76%), were practicing adequately, whereas 24% of the participants were carefree, and their practices were inadequate for preventing DM and its complication (Figure 1). There were many variations in knowledge of complication of diabetes, the most common complication was chosen by participants is retinopathy (74.5%), while the least one is vascular disease (34.7%) (Figure 2).
Study participant’s score showed that there is significant relation between knowledge, attitudes and practice with age (p=0.012, p=0.018 and p=0.000). We analyzed the gender-wise comparison of people’s knowledge, attitude and practice toward type 2 diabetes and its complication. It was observed that there is no difference or relation found (p=0.063, p=0.712 and p=0.587). Study participant’s knowledge scores showed that higher education had better knowledge scores and good practice compared to those who had low education (p=0.022, and p=0.031), while no difference was found in attitude scores (p=0.526). Also, the study demonstrates that there is no relation when having diabetes and with knowledge and attitude but shows good practice (p=0.030) (Tables 2-5).
|
Variable |
Good |
Poor |
Chi-Square |
P-Value |
|
|
Age |
Dec-18 |
24 |
36 |
14.638a |
0.012 |
|
Above 18-30 |
96 |
65 |
|||
|
31-40 |
56 |
23 |
|||
|
41-50 |
51 |
34 |
|||
|
51-60 |
43 |
30 |
|||
|
Above 60 |
10 |
11 |
|||
|
Sex |
male |
125 |
106 |
3.465a |
0.063 |
|
female |
155 |
93 |
|||
|
Education |
Primary school |
2 |
3 |
11.393a |
0.022 |
|
Intermediate school |
12 |
12 |
|||
|
High school |
55 |
59 |
|||
|
bachelor’s degree\diploma |
191 |
118 |
|||
|
Postgraduate |
20 |
6 |
|||
|
Living Area |
Bisha city |
238 |
169 |
.001a |
0.982 |
|
villages |
42 |
30 |
|||
|
Have DM |
Yes |
27 |
24 |
.715a |
0.398 |
|
No |
253 |
175 |
Table 2: Subjects’ socio-demographic characters and knowledge of type 2 diabetes mellitus and it’s complication.
|
Variable |
Good |
Poor |
Chi-square |
p-value |
|
|
Age |
Dec-18 |
18 |
42 |
13.705a |
0.018 |
|
Above 18-30 |
74 |
87 |
|||
|
31-40 |
18 |
61 |
|||
|
41-50 |
31 |
54 |
|||
|
51-60 |
27 |
46 |
|||
|
Above 60 |
8 |
13 |
|||
|
Sex |
Male |
83 |
148 |
.127a |
0.722 |
|
Female |
93 |
155 |
|||
|
Education |
Primary school |
2 |
3 |
3.193a |
0.562 |
|
Intermediate school |
7 |
17 |
|||
|
High school |
36 |
78 |
|||
|
Bachelor’s degree\diploma |
118 |
191 |
|||
|
Postgraduate |
12 |
14 |
|||
|
Living Area |
Bisha City |
148 |
259 |
.168a |
0.682 |
|
Villages |
28 |
44 |
|||
|
Have DM |
Yes |
17 |
34 |
.286a |
0.593 |
|
No |
159 |
269 |
Table 3: Subjects’ socio-demographic characters and attitude of type 2 diabetes mellitus and it’s complication.
|
Variable |
Good |
Poor |
Chi-Square |
p-value |
|
|
Age |
Dec-18 |
34 |
26 |
24.390a |
0 |
|
Above 18-30 |
115 |
46 |
|||
|
31-40 |
61 |
18 |
|||
|
41-50 |
72 |
13 |
|||
|
51-60 |
63 |
10 |
|||
|
Above 60 |
19 |
2 |
|||
|
Sex |
Male |
173 |
58 |
.296a |
0.587 |
|
Female |
191 |
57 |
|||
|
Education |
Primary school |
3 |
2 |
10.603a |
0.031 |
|
Intermediate school |
14 |
10 |
|||
|
High school |
79 |
35 |
|||
|
Bachelor’s Degree\Diploma |
247 |
62 |
|||
|
Postgraduate |
21 |
5 |
|||
|
Living Area |
Bisha City |
315 |
92 |
2.925a |
0.087 |
|
Villages |
49 |
23 |
|||
|
Have DM |
Yes |
45 |
6 |
4.690a |
0.03 |
|
No |
319 |
109 |
Table 4: Subjects’ socio-demographic characters and practice toward type 2 diabetes mellitus and it’s complication.
|
Do you know what diabetes is? |
Increased sugar levels in blood (74.9%) |
|
Increased production of glucose (4.9%) |
|
|
Increased lipid profiles in blood (1.5%) |
|
|
Don’t know (18.7%) |
|
|
what is/are the complication/s of diabetes mellitus? (multiple choice allows) |
Retinopathy (75.3%) |
|
Neuropathy (54%) |
|
|
Nephropathy (43%) |
|
|
Foot ulcer (50%) |
|
|
Vascular disease (35.1%) |
|
|
Don’t know (16.8%) |
|
what are the main indications of retinopathy? |
Eye weakness (56%) |
|
Pain in eyes (20.6%) |
|
|
Blurred vision (75.5%) |
|
|
Redness in eyes (16%) |
|
|
Do not know (14.5%) |
|
|
The main indication of nephropathy is excessive excretion of protein from the urine |
Strongly agree (28.7%) |
|
agree (36.8%) |
|
|
neutral (27.7%) |
|
|
disagree (4.9%) |
|
|
strongly disagree (1.9%) |
|
|
diabetic patients may develop lack of sensation in extremities |
Strongly agree (42.1%) |
|
agree (39.4%) |
|
|
neutral (14.3%) |
|
|
disagree (2.8%) |
|
|
strongly disagree (1.5%) |
|
|
diabetic patients may develop foot ulcer |
Strongly agree (37.9%) |
|
agree (41.3%) |
|
|
neutral (16.6%) |
|
|
disagree (3%) |
|
|
strongly disagree (1.3%) |
|
|
diabetic patients may develop gangrene |
Strongly agree (51.9%) |
|
agree (33.2%) |
|
|
neutral (10.4%) |
|
|
disagree (3.6%) |
|
|
strongly disagree (0.9%) |
|
|
Patients with T2DM should visit their healthcare providers for regular checkups even if their blood glycemia is under control |
Strongly agree (67.2%) |
|
agree (23.8%) |
|
|
neutral (7.2%) |
|
|
disagree (1.1%) |
|
|
strongly disagree (0.6%) |
|
I believe that there is not much use in trying to have good blood sugar control because the complications of diabetes will happen anyway |
Strongly agree (11.3%) |
|
agree (11.7%) |
|
|
neutral (13%) |
|
|
disagree (30%) |
|
|
strongly disagree (34%) |
|
|
I believe that keeping the blood sugar close to normal can help to prevent the complications of diabetes. |
Strongly agree (50.9%) |
|
agree (34.9%) |
|
|
neutral (11.9%) |
|
|
disagree (1.7%) |
|
|
strongly disagree (0.6%) |
|
|
I believe that type 2 diabetes is a very serious disease. |
Strongly agree (22.1%) |
|
agree (34%) |
|
|
neutral (26.8%) |
|
|
disagree (14.7%) |
|
|
strongly disagree (2.3%) |
|
|
I believe that blood sugar testing is not needed for people with Type 2 diabetes. |
Strongly agree (6.8%) |
|
agree (9.6%) |
|
|
neutral (14.7%) |
|
|
disagree (38.7%) |
|
|
strongly disagree (30.2%) |
|
|
I believe that people who have Type 2 diabetes will probably not get much payoff from tight control of their blood sugars. |
Strongly agree (11.1%) |
|
agree (16.2%) |
|
|
neutral (20%) |
|
|
disagree (31.1%) |
|
|
strongly disagree (21.7%) |
|
|
I believe that tobacco increase complication of diabetes. |
Strongly agree (31.7%) |
|
agree (36%) |
|
|
neutral (23.2%) |
|
|
disagree (7%) |
|
|
strongly disagree (2.1%) |
|
Diabetics should have an eye exam at least once a year |
Strongly agree (47.2%) |
|
agree (39.6%) |
|
|
neutral (9.4%) |
|
|
disagree (2.3%) |
|
|
strongly disagree (1.5%) |
|
|
Diabetic patients should not walk barefoot |
Strongly agree (53.6%) |
|
agree (27.2%) |
|
|
neutral (13%) |
|
|
disagree (3.2%) |
|
|
strongly disagree (3%) |
|
|
Diabetic patients should wear comfortable shoes. |
Strongly agree (64.3%) |
|
agree (27.4%) |
|
|
neutral (7%) |
|
|
disagree (0.6%) |
|
|
strongly disagree (0.6%) |
|
|
Diabetics should check their feet before and after putting on shoes. |
Strongly agree (54.9%) |
|
agree (31.1%) |
|
|
neutral (10.4%) |
|
|
disagree (2.8%) |
|
|
strongly disagree (0.9%) |
|
|
Diabetic patients should do regular exercise. |
Strongly agree (64.7%) |
|
agree (26.2%) |
|
|
neutral (7.4%) |
|
|
disagree (1.3%) |
|
|
strongly disagree (0.4%) |
|
|
Diabetic patients should have special diet to maintain normal blood sugar |
Strongly agree (66.6%) |
|
agree (26.6%) |
|
|
neutral (6%) |
|
|
disagree (0.4%) |
|
|
strongly disagree (0.4%) |
|
|
Diabetic patient should perform regular sugar monitoring |
Strongly agree (73.8%) |
|
agree (21.5%) |
|
|
neutral (4.3%) |
|
|
disagree (0%) |
|
|
strongly disagree (0.4%) |
Table 5: Percentages of response to the items of the questionnaire.
Diabetes mellitus describes a metabolic condition, in the 14th century known as black-death and the oldest known man-made condition in which insulin hormone is not adequately developed or used in the human body, which involved the transformation of carbohydrates into energy [8]. Type 1 diabetes (previously known as insulin-dependent, juvenile or childhood-onset) is characterized by deficient insulin production and requires daily administration of insulin. In 2017 there were 9 million people with type 1 diabetes; most of them live in high-income countries. Neither its cause nor the means to prevent it are known. Type 2 diabetes affects how the body uses sugar (glucose) for energy. It stops the body from using insulin properly, which can lead to high levels of blood sugar if not treated. Type 2 diabetes is often preventable. Factors that contribute to developing type 2 diabetes include being overweight, not getting enough exercise, and genetics. Early diagnosis is important to prevent the worst effects of type 2 diabetes. The best way to detect diabetes early is to get regular check-ups and blood tests with a healthcare provider [6]. Type II diabetes is becoming more commonplace worldwide, and during the next ten years, it is expected to rise significantly, especially in developing countries. According to a 2014 WHO report, 8.5% of persons over the age of 18 had diabetes, and this percentage is expected to rise sharply [6]. Treatment outcomes are recognized to be highly influenced by a patient’s knowledge, attitude, and behavior toward their illness and prevent the complication [5]. Previous study conducted in Jordan show good knowledge with for 53.5% which is close to our study knowledge’s score. according to in Jordan’s study the positive attitude was 46.3% while in our study was lesser than it (36.3%), and this may be due to lack of awareness campaign in our society [9]. Another study conducted in Jeddah, king Abdulaziz university with 1428 participant. In contrast to our study, it shows that there is a significant association between knowledge and gender, and also relation between knowledge and diabetes. According to attitude, also they show a relation between attitude with gender and who have DM. While the practice shows no significant relation like in our study [5], a study conducted in Hail region in general population. The majority of their participants show good knowledge (82%) with significant correlation, like our study, with age and this shows that as age increases, knowledge increases. Knowledge shows no relation between education level and residency. Their attitude was good in comparison to our sample [1]. In a study conducted in Riyadh about the complication of T2DM, higher number of them had inadequate knowledge regarding knowledge. Only 17% of their samples show adequate knowledge, in contrast to our study, which shows good knowledge for complication. Their educational level show presence of association with their knowledge [12].
Conclusion
The results show that a very good number of participants have a good general knowledge toward diabetes and its practice to control and prevent complication, but they have a poor attitude about it. Given the continual increase in the prevalence of the disease, urgent measures need to be implemented to improve disease control and management including awareness campaigns that aim to improve disease knowledge and management and then prevent the complication. Therefore, the current study can be used as a point of direction for future awareness campaigns in the Bisha province with a particular focus on attitude.
Acknowledgment
The authors are thankful to the Deanship of Graduate Studies and Scientific Research at University of Bisha for supporting this work through the Fast-Track Research Support Program. Also, the authors would like to thank all the members of the Bisha population who participated in this study.
Study Limitations
A non-randomized convenient sampling technique was used, which might have led to some biases.
Disclosure
The authors declare no conflicts of interest in this work.
References
- Aljofan M, Altebainawi A, Alrashidi MN (2019 Public knowledge, attitude and practice toward diabetes mellitus in Hail region, Saudi Arabia. Int J Gen Med 12: 255-262.
- Mayfield J (1998) Diagnosis and classification of diabetes mellitus: new criteria. Am Fam Physician 58: 1355-1362,1369-1370.
- CDC (2024) Centers for Disease Control and Prevention.
- Shawahna R, Samaro S, Ahmad Z (2021) Knowledge, attitude, and practice of patients with type 2 diabetes mellitus with regard to their disease: a cross-sectional study among Palestinians of the West Bank. BMC Public Health 21: 472.
- Gazzaz ZJ (2020) Knowledge, attitudes, and practices regarding diabetes mellitus among university students in Jeddah, Saudi Arabia. Diabetes Metab Syndr Obes 13: 5071-5078.
- World Health Organization (no date) Diabetes.
- Herath HMM, Weerasinghe NP, Dias H, Weerarathna TP (2017) Knowledge, attitude and practice related to diabetes mellitus among the general public in Galle district in Southern Sri Lanka: a pilot study. BMC Public Health 17: 535.
- Mezil SA, Abed BA (no date) Complication of Diabetes Mellitus, Annalsofrscb.ro.
- What is retinopathy? (no date) Diabetes.org.
- Gillani AH, Amirul Islam FM, Hayat K, Atif N, Yang C, et al. (2018) Knowledge, attitudes and practices regarding diabetes in the general population: A cross-sectional study from Pakistan. Int J Environ Res Public Health 15: 1906.
- Alsous M, Jalil MA, Odeh M, Al Kurdi R, Alnan M (2019) Public knowledge, attitudes and practices toward diabetes mellitus: A crosssectional study from Jordan. PLoS One 14: e0214479.
- Hassounah G, Al Dossari HJ, Robert AA (2023) Knowledge of complications of diabetes mellitus among patients with type 2 diabetes in Saudi Arabia: A descriptive study. Curr Diabetes Rev 19: e260922209161.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.