Practice Regarding Handover among Nurses Working in Critical Care Units at Selected Teaching Hospitals, Chitwan
by Sarmila Koirala*, Santosh Acharya
Nepalese Army Institute of Health Sciences, College of Nursing, Sanobharyang, Bhandarkhal, Kathmandu, Nepal
*Corresponding author: Sarmila Koirala Nepalese Army Institute of Health Sciences, College of Nursing, Sanobharyang, Bhandarkhal, Kathmandu, Nepal
Received Date: 16 February 2026
Accepted Date: 02 March, 2026
Published Date: 06 March, 2026
Citation: Koirala S and Acharya S (2026) Practice Regarding Handover among Nurses Working in Critical Care Units at Selected Teaching Hospitals, Chitwan. Int J Nurs Health Care Res 9:1700. DOI: https://doi.org/10.29011/2688-9501.101700
Abstract
Background and Objectives: Handover of patient information both within and between professional groups is necessary in ensuring patient safety and continuity of care. Poorly executed handover endangers the patient safety. Despite the importance of handover, there is no standard handover protocol available in the hospitals where study was carried out. Therefore, this study was conducted to find out the practice regarding handover among nurses working in critical care units. Method and Materials: The descriptive cross sectional research design was adopted with 108 nurses working in adult critical care units at two tertiary teaching hospitals of Chitwan district by using non probability, enumerative sampling technique. Data was collected using observation check list for practice regarding handover among nurses since 23rd June, 2017 for 1 month. Receiver Operating Characteristics (ROC) curve was used to find out the level of practice. Chi square was used to find out the association between practice and selected socio demographic variables. Results: The study findings revealed that the overall compliance of practice regarding handover was 49.9%. Only 42.6% of nurses had fair level of practice. The significant influencing variables were professional qualification, level of work performance and duration of handover (p=0.001, p=0.023, p<0.001 respectively). Conclusion: It was concluded that only less than half of the nurses had fair level of practice and positive level perception regarding handover. Therefore, use of standardized handover protocol and special attention needs to be given in addressing the weaknesses associated with handover process.
Keywords: Practice; Perception; Nursing handover; Nurses’ shift change report
Introduction
On a daily basis, in every healthcare facility, the responsibility for the care of patient is transferred between care providers. This process occurs in active environments that are typical of those in healthcare today. The communication of patients’ information to the next care provider can be known as “report”, “end-of-shift report”, “handoff” or “handover”. This communication is the exchange of information necessary for patient care to continue as planned. Three primary things are transferred during every handover i.e. information, authority and responsibility [1]. The formal part of handover is transferring patient care and responsibility from one nurse to another thus, enabling the nurse to deliver safe and ultimately quality nursing care. Clinical handover was identified as one of the key focus areas. Handover is described as the transfer of professional responsibility and accountability for some or all aspects of care for a patient or group of patients to another person or professional group on a temporary or permanent basis [2].
Handover is an integral part of clinical practice. It is so important that it is a process in which information about patient care is communicated in a consistent manner from one health care provider to another. Adverse patient events as a result of inadequate communication have been identified as a leading cause of death and injury in hospitals in the United States despite evidence-based efforts to reduce their occurrence. Nurses play a vital role in the process of communication and exchange of patient’s information through handover however minimal guidelines are available regarding handover in current nursing practice [3]. Globally, major healthcare institutions are looking at strategies to strengthen the efficacy and efficiency transfer of essential patient care information during nursing inter-shift handover. Communication during patient care, handover is ranked as fifth priority patient safety initiatives [4]. Bedside handover allows organizations to address the National Patient Safety Goals established by the Joint Commission addresses hospitals to encourage patients’ active involvement in their own care as a patient safety strategy (goal 13) and to aim to improve the effectiveness of communication among caregivers [5].
Nursing has had a long relationship with handover. Handover is a historic, institutionalized ritual that has remained part of nursing culture throughout the decades. Its roots lie deep in nursing tradition and nursing handover practice continues without questioning its purpose in contemporary times [6]. Nursing handover typically occurs at change of shift and shifts change two, three, or more times daily, seven days a week. The handover is seen as an important part and vital method of passing pertinent information about patients to nurses on next shift. Mainly there are four types of handovers is recorded, written, verbal (traditional) and bedside but nurses receive little formal training in this critical responsibility [7]. Location of handover varied depending on the needs of each specialty and impacted on what information was transferred. Namely, in a medical/surgical unit, handover was at the bedside [8].
The Joint Commission has acknowledged that communication breakdown is the major contributing factor in nearly 70% of adverse medical events with 75% of adverse events leading to patient death. Miscommunication is also a leading contributor of patient harm identified in more than 80% of medical malpractice lawsuits. In 2012, the Journal of Advanced Nursing reported that more than 43% of malpractice claims were related to inaccurate or incomplete patient handovers and that only 43.9% of accurate patient information actually reached the patient care unit during a patient transfer [9]. Accurate and timely communication of vital information between professional registered nurses is essential to assure patient safety. One of the most important times for nurseto-nurse communication is during the handover when information is exchanged and the responsibility of care for the patient is transferred [10]. It cannot be neglected the fact that handover in patient care is not part of the official education programs in nursing schools. So, nurses do not undergo any regular and particular training at undergraduate level and nurses learn the way of giving handover within the wards culture. Although the handover value for the nursing practice remains still one of the most important rituals of the nursing shift but sometimes it probably may not receive the proper attention from nurses [11].
Handover serve many functions, from social bonding to coaching and teaching, to team building but the most important function of handover is information processing to make sure that essential data are transferred for patient safety. Handover has been identified as a point at which errors are likely to occur. Failure in handover is a major preventable cause of patient harm and is principally due to the human factors of poor communication and systemic error. These can lead to inefficiencies, repetitions, delayed decisions, repeated investigations, incorrect diagnoses, incorrect treatment, avoidable readmissions, increased costs and poor communication with the patient. Verbal handover remains the popular way of communication at shift report this method augmented with a preprepared handover sheet will avoid the loss of vital information that may result in serious patient morbidity or mortality [12]. Despite the well-known negative consequences of inadequate nursing handover, very little research has been done to identify best practices. There is remarkable consistency in the anecdotally suggested strategies but there is a paucity of evidence to support them [13].
Though many researches are being conducted and standard protocol regarding handover are being used in developed countries, sentinel events are still occurring. Therefore, researcher is interested in exploring the practice regarding handover among nurses in developing countries like Nepal where very few studies regarding handover are available. Furthermore, it is important to determine how and in what way nurses carry out patient handover, what are taken into consideration during handover and what kind of problems are encountered during the process. Majority of the studies were carried out in western countries and very few have explored the practice regarding handover among nurses in our part of the World. So, the researcher strongly felt the need for in-depth understanding of the practice regarding handover among nurses to lay the foundation to improve future nursing handover processes and to provide suggestions and guidance to the nurses in the light of the results obtained for a better understanding of functions and implications of handover process for its effectiveness.
Materials And Methods
A descriptive cross-sectional study design was used to find out the practice regarding handover among nurses working in critical care units at selected teaching hospitals, Chitwan, Nepal. This study was conducted at critical care units i.e. Medicine Intensive Care Unit (MICU), Neuro Intensive Care Unit (Neuro-ICU), Surgical Intensive Care Unit (SICU) and Coronary Care Unit (CCU) of Chitwan Medical College Teaching Hospital (CMCTH) and College of Medical Science and Teaching Hospital (CMSTH). College of Medical Sciences and Teaching Hospital with 750 beds is the first teaching hospital in Chitwan district affiliated to Kathmandu University established on 1996. Likewise, Chitwan Medical College Teaching Hospital is 750 bedded hospitals affiliated to Tribhuvan University was established on 2006. Both hospitals are situated at Province number 3 and lies at the height of Bharatpur. Both teaching hospitals are tertiary level hospitals at Chitwan, having various critical care units with sufficient patient’s flow. Therefore, these setting were selected to conduct this study. The population of this study were all the nurses who have acquired one of the professional qualification PCL (Proficiency Certificate Level) nursing, BN (Bachelor in Nursing) and B.Sc. (Bachelor of Science in Nursing) working in critical care units and who provided handover during shift change. Non probability, enumerative sampling technique was used. In this study total sample population were (N=113) nurses but sample available during study was (n=108) therefore sample size (n) was 108 nurses. Those nurses, who were working in adult critical care units of CMCTH and CMSTH and those nurses who were available during data collection period and gave informed consent to participate in the study were included in the study.
Standardized guidelines Situation, Background, Assessment, Recommendation (SBAR) [14] along with the added components, preparatory phase (before handover), early phase of handover and after handover was used to observe practice regarding handover among nurses. Practice observation checklist was further categorized into 3 parts i.e. Part A (preparatory phase before handover), Part B (during handover phase which included SBAR components) and Part C (after handover phase). The components preparatory phase (before handover), early phase of handover and after handover were added in the guideline with the permission from the original author who developed SBAR guidelines. The added component in practice observation checklist was developed by the researcher after review of literature. Experts in School of Nursing, Chitwan Medical College had guided and provided their opinion throughout development of instrument.
The content validity of the research instrument was established by consulting research advisor and a group of professionals from nursing research (thesis) committee, School of Nursing, Chitwan Medical College. Pre-testing was done among 12 nurses of Universal College of Medical Science (UCMS), Bhairahawa, Nepal. On the basis of pretesting practice observation checklist was modified. Practice observation checklist had 66 items with dichotomous responses therefore; reliability was calculated by using Kuder Richardson formula 20 (KR-20). Calculated KR20 value for practice instrument was 0.78, which showed a high degree of internal consistency. Calculated inter-rater reliability of practice instrument was 96.9%, which indicated almost perfect strength of agreement between observers.
Prior to the commencement of the study, approval was taken from the Nursing Research (Thesis) Committee (NRC), School of Nursing, Chitwan Medical College Bharatpur-5. Data was collected after getting ethical clearance from Institutional Review Committee of Chitwan Medical College (CMC-IRC). Researcher collected the data from 23rd June 2017 to 22nd July 2017. Researcher herself collected the data in each shift (morning at 7 a.m., evening at 12 noon and night at 7 p.m.) by structured observation using event sampling method. During period of data collection researcher went to the research setting with oncoming nurse 15 minutes earlier in each shift before next shift starts (morning at 6:45 a.m., for evening shift at 11:45 a.m., and night at 6:45p.m.) and spent 2 hours in each shift as well as participated in normal work during that time. The total data collection duration took about 15-20 minutes for each nurse. Practice regarding handover was observed by taking permission from concerned authority (Hospital Director and Matron).
Researcher took written informed consent from each nurse prior to data collection after explaining the purpose of the study. No respondent was forced or coerced or intimidated in any way to participate in the study. Respondents were given right to reject or discontinue from the study at any time without any penalty. Researcher observed practice regarding handover using practice observation checklist by no concealment and participant observation method. It took approximately 5 minutes for nurses to give handover of each patient which was observed by the researcher during the time of shift change. Vital areas were noted during observation and the checklist was filled up immediately after completion of observation of each handover at nursing station without letting the nurses know about it. Researcher collected data from 6-8 nurses daily altogether in three shifts. Practice observation check list were coded as N1 to N108 of 108 nurses.
After collecting data, at first, the data was reviewed and checked for its completeness, consistency and accuracy after getting back from respondents. The collected data was organized, coded and entered in Epi Data 3.1 version and exported to Statistical Package for Social Science (IBM SPSS) version 20 for descriptive and inferential statistics. Descriptive statistics of quantitative data was presented by frequency, percentage, mean, standard deviation and mean percentage. In addition, Kolmogorov – Smirnov test was
used to check the normality of data distribution of practice, then practice score was further classified into two levels based on Receiver operating characteristics (ROC) curve (Figure 1) and mean score respectively. In the inferential statistics chi-square test, likelihood ratio and yate’s correction were used to find out the association between level of practice with the independent variables of the study.
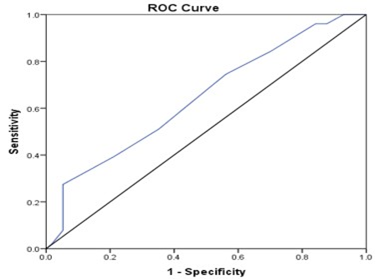
Figure 1: Receiver Operating Characteristics (ROC) Curve Regarding Practice of Handover among Nurses.
Results
|
n=108 |
||
|
Variables |
Frequency |
Percentage |
|
Age group (in years) |
||
|
<20 |
12 |
11.1 |
|
20-24 |
81 |
75 |
|
25 and above |
15 |
13.9 |
|
Mean± SD=22.49 ±1.88, Min=19 years Max= 30years |
||
|
Marital status |
||
|
Married |
23 |
21.3 |
|
Unmarried |
85 |
78.7 |
|
Religion |
||
|
Hindu |
97 |
89.8 |
|
Buddhist |
10 |
9.3 |
|
Christian |
1 |
0.9 |
|
Type of family |
||
|
Nuclear Family |
80 |
74.1 |
|
Joint Family |
28 |
25.9 |
|
reveals that, nurses’ age ranged from 19-30 years with the mean age of 22.49±1.88. Majority of the nurses (75.0%) belonged to age group 20-24 years. All nurses (100.0%) were female and residing outside nursing quarter. Majority of the nurses (78.7%) were unmarried, 89.8% belonged to Hindu religion and 74.1% were from nuclear family. |
||
Table 1: Socio-demographic Variables of the Nurses.
|
n=108 |
||
|
Variables |
Frequency |
Percentage |
|
Professional qualification |
||
|
Proficiency certificate level in nursing (PCL) |
70 |
64.8 |
|
Bachelor level in nursing (BN and B.Sc.) |
38 |
35.2 |
|
Designation |
||
|
Staff nurse |
98 |
90.7 |
|
Senior staff nurse |
10 |
9.3 |
|
Working hospital |
||
|
Chitwan Medical College Teaching Hospital (CMCTH) |
74 |
68.5 |
|
College of Medical Science and Teaching Hospital (CMSTH) |
34 |
31.5 |
|
Working unit |
||
|
Medical Intensive Care Unit |
46 |
42.6 |
|
Surgical Intensive Care Unit |
19 |
17.6 |
|
Neuro Intensive Care Unit |
24 |
22.2 |
|
Coronary Care Unit |
19 |
17.6 |
|
Total professional experience (in years) |
||
|
<1year |
33 |
30.6 |
|
1-3years |
65 |
60.1 |
|
>3years |
10 |
9.3 |
|
Professional experience in critical care unit (in years) |
||
|
<1year |
41 |
38 |
|
1-3years |
63 |
58.3 |
|
>3years |
4 |
3.7 |
|
Mean± SD=1.23 ±0.92, Min=1 month Max= 60 months |
||
|
Working shift |
||
|
Morning |
37 |
34.3 |
|
Evening |
31 |
28.7 |
|
Night |
40 |
37 |
|
Level of work performance |
||
|
Advance beginner |
32 |
29.6 |
|
Competent |
43 |
39.8 |
|
Proficient |
33 |
30.6 |
|
Received in-service education on handover |
||
|
Yes |
48 |
44.4 |
|
No |
60 |
55.6 |
|
Handover duration (in minutes) |
||
|
<2 Minutes |
4 |
3.7 |
|
2-3 Minutes |
67 |
62 |
|
>3 Minutes |
37 |
34.3 |
|
Mean ± SD=2.77 ± 0.63, Min =1.50 minutes Max = 4minutes |
||
|
shows that, among 108 nurses, majority of the nurses (64.8%) had completed PCL, 90.7% were staff nurse, 68.5% nurses were working in CMCTH. Regarding working unit, 42.6% nurses were from Medical ICU whereas, 17.6% of nurses were working in Surgical and Neuro -ICU. In regards to professional experience, 30.6%of nurses had <1year experience. Regarding experience in critical care unit, 38.0% of nurses had <1year experience. Regarding working shift more than one third (37%) of nurses had night duty whereas, 28.7% of nurses had evening duty. Regarding level of work performance, 39.8% of the nurses find them self as competent whereas, 29.6% find themselves as advance beginner. In-service education regarding handover was received by 55.6% of nurses. Regarding duration of handover, 3.7% of nurses took<2 minutes for handover. The mean duration for nursing handover was 2.77 ± 0.63 minutes. |
||
Table 2: Profession Related Variables of the Nurses.
|
n=108 |
||
|
Variables |
Frequency |
Percentage |
|
Availability learning resources related to handover |
||
|
Adequate |
61 |
56.5 |
|
Inadequate |
47 |
43.5 |
|
Presence of positive reinforcement from supervisors |
||
|
Yes |
79 |
73.1 |
|
No |
29 |
26.9 |
|
Nurse patient ratio |
||
|
0.043056 |
12 |
11.1 |
|
0.04375 |
54 |
50 |
|
More than 1:3 |
42 |
38.9 |
|
reveals that, all handovers (100.0%) were given at bedside by verbal with written documentation method. Availability of handover guidelines in the ward was reported by none of the nurses. More than half of the nurses (56.5%) reported that adequate number of resources was available regarding handover in their working unit. Majority of the nurses (73.1%) reported that they get positive reinforcement from supervisors. All nurses (100.0%) reported that they have good interpersonal relationship with their colleagues. Half of the nurses (50.0%) were assigned patient in the ratio of 1:3. |
||
Table 3: Health Care Environment Related Variables.
|
n=108 |
||||
|
Subscale of Practice |
Maximum Possible Score |
Obtained Range |
Mean Score±SD |
Mean Percentage |
|
Preparatory phase (Before) |
8 |
46146 |
4.12±0.32 |
51.5 |
|
During handover |
51 |
19-35 |
26.81±3.28 |
52.5 |
|
Early phase |
7 |
46115 |
3.70±0.45 |
52.8 |
|
Situation(S) |
5 |
46083 |
2.5±0.50 |
50 |
|
Background(B) |
12 |
46176 |
4.5±0.69 |
37.5 |
|
Assessment (A) |
24 |
44470 |
14.36±2.48 |
59.8 |
|
Recommendation(R) |
3 |
0-2 |
1.75±0.45 |
58.3 |
|
After handover |
7 |
46083 |
2.00±0.09 |
28.5 |
|
Total |
66 |
25-41 |
32.94±3.17 |
49.9 |
|
Shows that, practice of nurses regarding handover contained 3 subscales preparatory phase (before handover), during handover and after handover with score of 8, 51 and 7 respectively. Concerning practice of nurses, the total mean score obtained was 32.94 ± 3.17 and mean percentage of 49.9%. Maximum mean score was obtained in during handover subscale which was 26.81 ±3.28 and mean percentage 52.8%. |
||||
Table 4: Mean Score of Practice Regarding Handover among Nurses.
Figure: Receiver Operating Characteristics (ROC) Curve
Accuracy of discrimination is assessed by the area under the receiver operating characteristics (ROC) curve. Because the sensitivity and specificity can be manipulated by adjusting the decision threshold, there is a need to evaluate the accuracy and discrimination of practice over wide range of cut off points. This is possible with the use of ROC curve. The ROC Curve plots the sensitivity (Y-axis) against 1-specificity (X-axis). The area under the ROC curve (AUC) is a measure of how well a parameter can distinguish between two diagnostic groups. For practice score of nurses regarding handover the area under the curve was 0.643. An area under the ROC curve 643 describes a situation in which the practice score of nurses covers 64.3% area of the curve. When the area under the curve is 64.3% the minimum difference of sensitivity and specificity was at the point where sensitivity was 51% with specificity of 64.9% which gave the cutoff point of score 33.5. As overall compliance was found very low (49.9%) from this cutoff point practice was classified into two categories as fair and poor.
|
n=108 of 0 |
||
|
Level of Practice |
Frequency |
Percentage |
|
Fair (score ≥33.5) |
46 |
42.6 |
|
Poor (score <33.5) |
62 |
57.4 |
|
Total |
108 |
100 |
|
Cut off point from ROC Curve (33.5) |
||
|
Depicts that, only 42.6% of the nurses had fair level of practice regarding handover whereas 57.4% of nurses had poor level of practice regarding handover. None of the nurses had good and very good practice. |
||
Table 5: Level of Practice Regarding Handover among Nurses.
|
n=108 |
||||
|
Variables |
Level of Practice |
c2 |
p-value |
|
|
Fair |
Poor |
|||
|
No. (%) |
No. (%) |
|||
|
Age group (in years) |
||||
|
<20 |
4(33.3) |
8(66.7) |
4.292 |
0.117 |
|
20-24 |
32(39.5) |
49(60.5) |
||
|
≥25 |
10(66.7) |
5(33.3) |
||
|
Marital status |
||||
|
Married |
11(47.8) |
12(52.2) |
0.327 |
0.567 |
|
Unmarried |
35(41.2) |
50(58.8) |
||
|
Religion |
||||
|
Hindu |
43(44.3) |
54(55.7) |
0.581 |
0.446¥ |
|
Other than Hindu |
3(27.3) |
8(72.7) |
||
|
Type of family |
||||
|
Nuclear Family |
33(41.2) |
47(58.8) |
0.227 |
0.633* |
|
Joint Family |
13(46.4) |
15(53.6) |
||
|
Significant Level at 0.05 *Likelihood Ratio ¥Yates Correction |
||||
|
Shows that, there was no significant association between level of practice regarding handover among nurses with any socio-demographic variables of nurses. |
||||
Table 6: Association between Level of Practice Regarding Handover among Nurses and Socio-demographic Variables of Nurses.
|
n=108 |
||||
|
Variables |
Level of Practice |
c2 |
p-value |
|
|
Fair |
Poor |
|||
|
No. (%) |
No. (%) |
|||
|
Professional qualification |
||||
|
Proficiency certificate level in nursing |
22 (31.4) |
48(68.6) |
10.141 |
0.001 |
|
Bachelor level in nursing |
24 (63.2) |
14 (36.8) |
||
|
Designation |
||||
|
Staff nurse |
40 (40.8) |
58 (59.2) |
0.694 |
0.405¥ |
|
Senior staff nurse |
6 (60.0) |
4 (40.0) |
||
|
Working hospital |
||||
|
Chitwan Medical College, Teaching Hospital |
46(62.2) |
28(37.8) |
- |
NA |
|
College of Medical Science, Teaching Hospital |
0(0.0) |
34(100.0) |
||
|
Working unit |
||||
|
Medical Intensive Care Unit |
22 (47.8) |
24 (52.2) |
1.89 |
0.596 |
|
Surgical Intensive Care Unit |
9 (47.4) |
10 (52.6) |
||
|
Neuro Intensive Care Unit |
9 (37.5) |
15 (62.5) |
||
|
Coronary Care Unit |
6 (31.6) |
13 (68.4) |
||
|
Total professional experience (in years) |
||||
|
<1year |
13 (39.4) |
20 (60.6) |
0.275 |
0.871* |
|
1-3years |
29 (44.6) |
36 (55.4) |
||
|
>3years |
4 (40.0) |
6 (60.0) |
||
|
Professional experience in critical care unit (in years) |
||||
|
<1year |
19 (46.3) |
22 (53.7) |
0.818 |
0.664* |
|
1-3years |
26 (41.3) |
37 (58.7) |
||
|
>3years |
1 (25.0) |
3 (75.0) |
||
|
Working Shift |
||||
|
Morning |
11 (29.7) |
26 (70.3) |
4.5 |
0.105 |
|
Evening |
17 (54.8) |
14 (45.2) |
||
|
Night |
18 (45.0) |
22 (55.0) |
||
|
Received in-service education on handover |
||||
|
Yes |
22(45.8) |
26(54.2) |
0.371 |
0.542 |
|
No |
34(40.0) |
36(60.0) |
||
|
Level of work performance |
||||
|
Advance beginner |
9 (28.1) |
23 (71.9) |
7.514 |
0.023 |
|
Competent |
25 (58.1) |
18 (41.9) |
||
|
Proficient |
12 (36.4) |
21 (63.6) |
||
|
Handover Duration |
||||
|
≤3 Minutes |
17(23.9) |
54(76.1) |
29.477 |
<0.001 |
|
>3 Minutes |
29(78.4) |
8(21.6) |
||
|
Significant Level at 0.05 *Likelihood Ratio¥Yates Correction |
||||
|
Shows that there was statistically significant association between the level of practice of nurses and professional qualification (p=0.001), level of work performance (p=0.023) and duration of handover (p=<0.001). It indicates that fair level of practice was among nurses who had bachelor level in nursing finds themselves as competent and took >3 minutes for handover. There was no significant association between level of practice of nurses regarding handover and other profession related variables of nurses. |
||||
Table 7: Association between Level of Practice Regarding Handover among Nurses and Profession Related Variables of Nurses.
|
n=108 |
||||
|
Variables |
Level of Practice |
c2 |
p-value |
|
|
Fair |
Poor |
|||
|
No. (%) |
No. (%) |
|||
|
Availability of learning resources |
||||
|
Adequate |
25(41.0) |
36(59.0) |
0.148 |
0.7 |
|
Inadequate |
21(44.7) |
26(55.3) |
||
|
Presence of positive reinforcement |
||||
|
From supervisors regarding handover |
||||
|
Yes |
33(41.8) |
46(58.2) |
0.081 |
0.776 |
|
No |
13(44.8) |
16(55.2) |
||
|
Nurse patient ratio |
||||
|
Less than 1:3 |
30(45.4) |
36(54.5) |
0.569 |
0.451 |
|
More than1:3 |
16(38.1) |
26(61.9) |
||
|
Significant Level at 0.05 |
||||
|
Illustrates that, there was no significant association between level of practice of nurses regarding handover among nurses and any health care environment related variables. |
||||
Table 8: Association between Level of Practice Regarding Handover among Nurses and Health Care Environment Related Variables.
Discussion
In health care institutions, work must continue 24 hours a day and 7 days a week. As nurses are the primary caretakers of the patients a team of nurses need to provide patient care in around-the clock basis which requires transfer of patient care responsibilities along with authority, a process known as “handover”. Although handover has been a routine aspect of nursing practice for decades many literatures have shown that the practice and perception regarding handover still needs improvement. The mean age of nurses was 22.49±1.88. Due to high turnover rate of nurses, hospital has to recruit newly graduates with less professional experience hence most of the nurses belong to age group of 20 - 24 with low mean age. Regarding the gender of the nurse, the present study revealed all the nurses (100.0%) were female. This high proportion of female nurses was most probably due to the fact that the enrolment of the nursing students in Nepalese universities and nursing school available only for females, the profession of nursing in Nepal is mostly feminine. Nearly one fourth of the nurses (21.3%) were married. The present study revealed all the nurses (100.0%) were residing outside the nursing quarter and the reason behind is most of the private hospitals in Nepal have no provision of nursing quarter.
Level of Practice Regarding Handover among Nurses
The findings of the present study revealed that overall compliance of practice regarding handover was only 49.9% which is less than one of the studies which showed 76.0% compliance. (15) In relation to practice, only 42.6% of nurses had fair level of practice followed by 57.4% of nurses had poor level of practice regarding handover. Overall compliance of practice along with fair level of practice regarding handover among less than 50 % indicated poor practice which warrants immediate action for improvement. The differences in the overall compliance of practice regarding handover among nurses in context of Nepal might be due to lack of protocol/guidelines regarding handover, nurses competency level, shrinking of clinical field, privatization of nursing education with profit motive, limited exposure of nurses, brain drain, lack of motivation among nurses, low salary, limited use of evidence based practice, lack of frequent audit regarding handover, political instability, loop holes during accreditation of nursing colleges and hospitals, lack of supervision and monitoring by regulating bodies of nursing at hospital regarding handover.
The overall compliance of Situation, Background, Assessment, Recommendation (SBAR) was 50.0%, 37.5%, 59.8%, 58.3% respectively which is inconsistent to one of the studies that showed compliance of Situation, Background, Assessment, Recommendation as 86.0%, 82.0%, 79.0%, 80.4% respectively. [15] The reason behind this might be that the nurses did not used nursing process properly during handover. Regarding practice of nurses before handover less than one eighth of the nurses (12%) washed hands with sanitizer which is less than one of the studies that revealed 49.1% washed hands [16]. Though hand washing is a vital aspect, especially in critical care units the findings of the study is unacceptable which might be due to negligence of nurses and may lead to cross infection, increase in ICU Mortality rates. None of the nurses informed visitors to ask any queries after handover which is in contrast to the findings of the study conducted by Kilic, Ovayolu, Ovayolu and Ozturk (2017) that revealed 52.1% of the nurses answered the queries of family members after handover. This might lead to decrease in satisfaction level of patient and visitors.
During handover 73.1% of nurses used professional communication skills whereas, none of the nurses encouraged patient to be involved on handover and introduced oncoming nurse to the patient. The study conducted by Kilic, Ovayolu, Ovayolu and Ozturk (2017) showed contrary findings 95.2% of nurses used professional communication skills, 45.6% of the nurse’s involved patient during handover and 45.8% introduced themselves. This might lower the image of nursing in society and dissatisfaction among patient and visitors. None of the nurses stated history of any allergies which is less than findings of study conducted at Turkey, where 87.5% of nurses handed over about treatment and allergies [17]. This might sometimes lead to life threatening conditions of patient. None of the nurses specified about nursing care plans, nursing concerns and actions for the next shift which is less than one of the studies where 68% of the nurses handed over nursing care plans [16]. Though nursing care plan are vital aspects of nursing profession the results showed lack of awareness and applicability of nursing care plans which might decrease the quality of nursing care. After handover only 0.9% of nurses washed hands whereas none of the nurse’s asked patients/visitors about any queries before leaving working unit, thanked the patients for allowing care, used closing words which might again leads to cross infection and self-harm as well as decreased level of satisfaction among patients.
Association between Level of Practice and Selected Variables
Findings of the present study unveiled that practice levels of the nurses’ regarding handover was significantly associated with professional qualification (p=0.001), level of work performance (p=0.023), duration of handover(p=<0.001) and didn’t show statistically significant association with any socio-demographic variables and health care environment related variables which is similar to the research study that revealed there was no significant association between level of knowledge of practice and socio-demographic variables which indicates that professional competency might not be influenced by socio-demographic variables [18]. Professional qualification was significantly associated with level of practice in this study, only 35.2% of nurses acquired bachelor level nursing education which is less than the study done at Turkey, which revealed 51.9% of the nurses got bachelor level nursing education [17] The reason behind the increased number PCL nursing education due to the fact that most of the nurses having bachelor level nursing education reside or pursue in the aboard for better carrier and further education and another fact is due to the enrolment of the nursing student in bachelor level is relatively lower than PCL in Nepal. Similarly, duration of handover was also found significantly associated with level of practice in this study, the handover time ranged between 1.50 to 4 minutes with mean 2.77±0.63 minutes which is inconsistent with the one of the studies that revealed higher duration which ranged from 5-22 minutes with mean 10.95±4 minutes [19].
The reason behind this as seen by researcher was many nurses working in more than one hospital and getting hurried to give handover to carry out duty on another hospital. Though, total professional experience, in-service education, availability of handover protocol/ guidelines was not found statistically significant with level of practice among nurses the researcher interpreted that these variables might influence the practice level. The mean total professional experience and professional experience in the current ward of the nurses were 1.55±1.19 years and 1.23±0.92 years respectively which is less than one of the studies that revealed mean experience of 5.63±5.72 years and 2.9±2.8 respectively [20]. This reason behind the less experience was most of the staff nurses were newly graduated and acquired less experience who were directly involved in patient care. Hence, lack of experience degraded the practice and perception regarding handover. More than half (55.6%) of the nurses reported that they have not received any in-service education regarding handover.
This study is evidently supported by one of the studies that showed significant differences between pre and post educational session of nursing hand off regarding to handoff interventions and impact on patient care (p=0.034) [21] Therefore, the findings of this study are a good basis to formulate the educational activities, as there is need of continuous nursing education program for nurses regarding handover. Improving knowledge and monitoring practice of nurses could significantly reduce the adverse effects that may develop from the inappropriate handover which may become the basis for improving the concept of nursing care quality and patient safety and suggests periodic check or review of knowledge and practice regarding handover among nurses is necessary. In concern of availability of protocol regarding handover none of the nurses reported about availability of written protocol regarding handover in ward, it seems that due to lack of handover protocol nurses practice score regarding handover was not good enough.
This result is less than the findings of study conducted at Korea, which revealed that 13% of the nurses respectively reported the availability of protocol regarding handover in the ward.(20) One of the study revealed that cardiac nursing care performance increased from 1.5±0.6 before intervention to 2.7±0.9 after intervention which was accompanied with 80% [22] Thus, the findings of the present study as both study point out the need of nurses to adhere the protocol regarding handover as well as development of a regulated, practical and comprehensive standard protocol to transmit crucial and relevant information related to the patient care will improve nurses safe practice in the area of basic nursing care and communication about patients’ condition. This study was conducted in only two teaching hospitals. Study was conducted in small sample size which limits to generalization. The study included only outgoing nurses who were giving handovers but not included the oncoming nurses who were taking handover. The study findings can be used by nurses to examine the quality of nursing care in critical care units as reflected by its outcome.
Conclusion
It is concluded that less than half of the nurses have fair level of practice regarding handover. The significant influencing variables for level of practice were professional qualification, level of work performance and handover duration.
Acknowledgement
It is a pleasure, delight and contentment to show gratefulness to individuals who helped me during thesis preparation. Researcher would like to expresses her sincere gratitude to all the nurses who participated in the study and provided the valuable information for this study. Without their participation, cooperation and support it would have been impossible to complete this study.
References
- Behara R, Wears RL, Perry SJ, Eisenberg E, Murphy L, Vanderhoef M, et al. (2005) A Conceptual Framework for Studying the Safety of Transitions in Emergency Care. Advances in Patient Safety: From Research to Implementation. 2.
- Thomas MJW, Schultz TJ, Hannaford N, Runciman WB (2013) Failures in Transition: Learning from Incidents Relating to Clinical Handover in Acute Care. J Healthc Qual 3:49-56.
- Hospital Accreditation Program (2017)
- Poh CL, Parasuram R, Kannusamy P (2013) Nursing intershift handover process in mental health settings: A best practice implementation project. Int J Evid Based Healthc 1:26-32.
- Health A, Accreditation C (2018) Ambulatory Health Care National Patient Safety Goals.
- Cheek J (2000) Postmodern and Poststructural Approaches to Nursing Research.
- Chiò A, Montuschi A, Cammarosano S, De Mercanti S, Cavallo E, Ilardi A, et al. (2007) ALS patients and caregivers communication preferences and information seeking behaviour. Eur J Neurol 1: 55-60.
- Johnson M, Jefferies D, Nicholls D (2012) Developing a minimum data set for electronic nursing handover. J Clin Nurs 3-4:331-43.
- Issues up close - American Nurse Today.
- Hilligoss B, Cohen MD (2011) Hospital Handoffs as Multifunctional Situated Routines: Implications for Researchers and Administrators. Ad Health Care Manag 11:91-132.
- Scovell S (2010) Role of the nurse-to-nurse handover in patient care. Nurs Stand 20: 35-9.
- Pothier D, Monteiro P, Mooktiar M, Shaw A (2005) Pilot study to show the loss of important data in nursing handover. Br J Nurs 20:1090-3.
- Riesenberg LA, Leisch J, Cunningham JM (2010) Nursing Handoffs: A Systematic Review of the Literature. Am J Nurs 4: 24-34.
- Leonard M, Graham S, Bonacum D (2004) The human factor: the critical importance of effective teamwork and communication in providing safe care. Qual Saf Health Care. 1: i85-90.
- Kumar P, Jithesh V, Vij A, Gupta S (2016) Need for a hands-on approach to hand-offs: A study of nursing handovers in an Indian Neurosciences Center. Asian J Neurosurg 1:54-59
- Malekzadeh J, Mazluom SR, Etezadi T, Tasseri A (2013) A standardized shift handover protocol: improving nurses’ safe practice in intensive care units. J caring Sci 3:177-85.
- Parlar Kilic S, Professor A, Ovayolu N, Ovayolu O, Hayrullah Ozturk M. The Approaches and Attitudes of Nurses on Clinical Handover [Internet]. Vol. 10, International Journal of Caring Sciences. [cited 2018 Sep 5]. Available from: www.internationaljournalofcaringsciences.org
- Kapurkar KS, Babar R, Jagadale S, Patil N V (2016) TO ASSESS KNOWLEDGE & KNOWLEDGE OF PRACTICE REGARDING STANDARD OPERATING PROTOCOL FOR IMPLEMENTING BEDSIDE HANDOVER IN NURSING AMONG STAFF NURSES AT KRISHNA HOSPITAL, KARAD. J Evol Med Dent Sci
- Spooner AJ, Chaboyer W, Corley A, Hammond N, Fraser JF (2013) Understanding current intensive care unit nursing handover practices. Int J Nurs Pract 2: 214-20.
- Kim EM, Ko JW, Kim S (2016) Korean nurses’ perspectives regarding handoffs. Contemp Nurse 4:421-9.
- Elhanafy EY, Hammour ZE (2014) Effect of educational sessions about effectiveness of handoff system for nurses on their knowledge and practice. Journal of Community Medicine 3:13-26.
- Etezadi T, Malekzadeh J, Mazlom SR, Tasseeri A (2012) Nursing Handover Written Guideline Implementation: A Way to Improve Safe Performance of Nurses in Intensive Care Units. Mashhad Univ Med Sci 2: 7-18.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.