Patterns of Preventable Illness and Referral Outcomes Among Women and Children Attending a Rural Primary Care Clinic in Punjab, Pakistan
by Daniyal MM Elahi1*, Harris Elahi1, Nadia Elahi1, Selina Nishtar2, Filiz Ozmisir3
1Independent Researcher, Toronto, Canada
2Independent Researcher, Kettering, United Kingdom
3Founder, Refugee Girls Worldwide, Canada
*Corresponding author: Daniyal M.M. Elahi, Independent Researcher, Toronto, Canada
Received Date: 14 January, 2026
Accepted Date: 22 January, 2026
Published Date: 26 January, 2026
Citation: Elahi DMM, Elahi H, Elahi N, Nishtar S, Ozmisir F (2026) Patterns of Preventable Illness and Referral Outcomes Among Women and Children Attending a Rural Primary Care Clinic in Punjab, Pakistan. J Community Med Public Health 10: 552. https://doi.org/10.29011/2577-2228.100552
Abstract
Background: Women and children in rural Pakistan experience a high burden of preventable illness, compounded by barriers to timely access to primary care. Community-based primary care clinics play a critical role in early management and gatekeeping within health systems by managing high-volume, low-acuity conditions and identifying cases requiring referral; however, local data describing utilization and referral patterns remain limited. Objective: To describe patterns of clinic utilization, preventable illness burden, and referral outcomes among women and children attending a rural primary care clinic in Punjab, Pakistan. Methods: A descriptive observational study was conducted using prospectively collected, de-identified clinic encounter data over a one-month period. Visits were categorized by presenting condition, preventability, and referral outcome. Descriptive statistics, two-variable analysis, and probability-based measures were used to examine associations between preventability and referral. Results: A total of 356 clinic visits were analyzed. Children accounted for 61.5% of visits. Gastrointestinal, respiratory, and skin-related conditions comprised 60.7% of presentations. Overall, 57.0% of visits were classified as likely preventable. The overall referral rate was 22.5%. Visits classified as not preventable had a higher probability of referral (34.6%) compared with preventable visits (13.3%). Conclusion: Preventable conditions account for the majority of clinic visits among women and children in this rural setting, while non-preventable conditions disproportionately drive referrals. These findings highlight the gatekeeping function of communitybased primary care clinics and support the use of routine clinic-level data to inform prevention strategies and health system planning in low-resource maternal and child health settings.
Keywords: Maternal and child health; Primary care; Preventable illness; Rural health; Clinic utilization; Referral patterns; Pakistan
Introduction
Maternal and child health remains a major public health priority in Pakistan, particularly in rural areas where preventable conditions contribute substantially to morbidity and health system burden [13]. Barriers such as limited access to care, financial constraints, and delayed health-seeking behavior have been shown to exacerbate disease severity at presentation among women and children [2,3].
Community-based primary care clinics serve as essential entry points into the health system, providing early management of common conditions and identifying cases requiring referral to higher-level facilities [4]. Despite their importance, clinic-level data describing utilization patterns, preventability, and referral outcomes in rural Pakistan remain limited.
Primary Care Theory emphasizes the role of community-based clinics in delivering first-contact care, preventive services, continuity, and coordination within health systems. In low-resource rural settings, primary care clinics function as gatekeepers— managing high volumes of low-acuity and preventable conditions locally while identifying and referring cases requiring escalation. Understanding patterns of preventable illness and referral within this framework is essential for strengthening maternal and child health systems.
This study provides descriptive clinic-level evidence on illness patterns and referral dynamics among women and children attending a rural primary care clinic in Punjab, Pakistan.
Methods
Study Design
Descriptive observational study using prospectively collected, deidentified clinic encounter data.
Study Setting
A rural primary care clinic in Punjab, Pakistan, providing outpatient services exclusively to women and children.
Study Period
Four consecutive weeks.
Study Population
All women (≥18 years) and children (0-17 years) attending the clinic during the study period were included. Each clinic visit was treated as a single observation.
Data Collection
Data were recorded by the on-site primary care physician as part of the routine clinical workflow using a standardized encounter log. Data collection reflected usual care practices in the clinic and did not alter clinical decision-making. No personal identifiers were collected, and variables and definitions were held constant throughout the study period.
Variables
Patient group: Child / Adult woman
Primary condition category: Gastrointestinal; Respiratory; Skin/ Wound; Fever; Maternal/Women’s Health; Other (chronic followup, musculoskeletal, minor injury)
Preventability: Likely preventable / Not preventable
Referral outcome: Referred / Not referred
Preventability was classified using pragmatic, operational definitions informed by prior studies examining avoidable illness related to hygiene, nutrition, early care-seeking, and preventive education [1-3]. In routine primary care practice, assessments of preventability are often intuitive and based on clinical judgment rather than standardized tools. Although validated instruments exist for chronic disease risk assessment, no validated tools currently exist to assess visit-level preventability of acute conditions in rural low-resource settings. For this study, a standardized operational definition was applied consistently across encounters to support descriptive analysis while reflecting real-world primary care practice.
For this study, a standardized operational definition was applied consistently across encounters to support descriptive analysis while reflecting real-world primary care practice. Examples of conditions classified as likely preventable included acute diarrhea, uncomplicated upper respiratory infections, and minor skin infections associated with hygiene or delayed early care; conditions classified as not preventable included presentations requiring escalation, suspected serious infection, or conditions needing diagnostic evaluation or specialist management.
Data Analysis
Descriptive statistics were used to summarize visit distributions. Two-variable analysis examined the relationship between preventability and referral outcome. Basic and conditional probabilities were calculated. No inferential statistical testing was performed.
Results
Study Sample
A total of 356 clinic visits were recorded during the study period.
Patient Characteristics
Children accounted for the majority of clinic visits (Table 1).
|
Patient Group |
Visits (n) |
Percentage (%) |
|
Children |
219 |
61.5 |
|
Adult women |
137 |
38.5 |
|
Total |
356 |
100 |
Table 1: Patient group distribution.
Distribution of Presenting Conditions
Gastrointestinal, respiratory, and skin-related conditions accounted for 60.7% of all clinic visits (Table 2) (Figure 1).
Figure 1: Illustrates the distribution of presenting condition categories over the one-month study period. Gastrointestinal, respiratory, and skin-related conditions accounted for the majority of clinic visits. Lower-frequency conditions were grouped into an “Other” category to improve interpretability.
|
Condition Category |
Visits (n) |
Percentage (%) |
|
Gastrointestinal |
81 |
22.8 |
|
Respiratory |
72 |
20.2 |
|
Skin / Wound |
63 |
17.7 |
|
Fever |
54 |
15.2 |
|
Maternal / Women’s Health |
41 |
11.5 |
|
Other |
45 |
12.6 |
|
Total |
356 |
100.0 |
Table 2: Distribution of presenting conditions.
Preventability of Clinic Visits
More than half of all visits were classified as likely preventable (Table 3).
|
Preventability |
Visits (n) |
Percentage (%) |
|
Likely preventable |
203 |
57.0 |
|
Not preventable |
153 |
43.0 |
|
Total |
356 |
100.0 |
Table 3: Preventability classification.
Referral Outcomes
The overall referral rate was 22.5% (80/356). Visits classified as not preventable were referred more frequently than preventable visits (Table 4).
|
Preventability |
Referred (n) |
Not Referred (n) |
Total (n) |
|
Likely preventable |
27 |
176 |
203 |
|
Not preventable |
53 |
100 |
153 |
|
Total |
80 |
276 |
356 |
Table 4: Preventability by referral outcome.
Figure 2 illustrates the difference in referral rates between visits classified as likely preventable and those classified as not preventable.
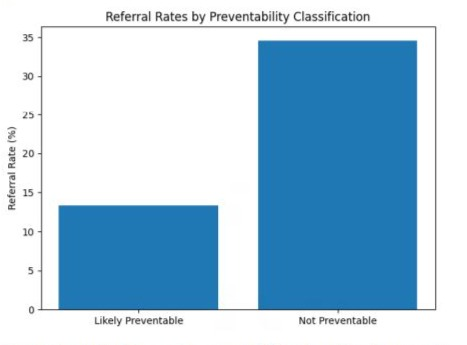
Figure 2: Referral rates by preventability classification among clinic visits.
Probability Analysis
P(Referral) = 80 / 356 ≈ 0.225
P(Referral | Preventable) = 27 / 203 ≈ 0.133
P(Referral | Not Preventable) = 53 / 153 ≈ 0.346
Visits classified as not preventable were more than twice as likely to result in referral. Referral probability was approximately 2.6 times higher in visits classified as not preventable compared with likely preventable visits (0.346 vs 0.133).
Discussion
This study provides clinic-level evidence on patterns of illness presentation, preventability, and referral outcomes among women and children attending a rural primary care clinic in Punjab, Pakistan. Preventable conditions accounted for the majority of clinic visits, while non-preventable conditions disproportionately contributed to referrals.
The predominance of gastrointestinal, respiratory, and skin-related conditions is consistent with prior studies documenting avoidable morbidity among women and children in rural Pakistan [1-3,6]. The stability of condition distributions over the one-month period suggests that routinely collected clinic data can yield meaningful insights for service evaluation.
Although preventable conditions represented most visits, referral probability was substantially higher among non-preventable cases. Similar patterns have been described in primary care systems where clinics manage high-volume, low-acuity conditions locally while escalating care for more complex presentations [4,7]. These findings highlight the importance of strengthening preventive capacity while maintaining effective referral pathways for higherrisk cases.
From a primary care perspective, effective management of preventable conditions at the community level may reduce unnecessary referrals, support workload management, and preserve referral capacity for higher-risk cases. By addressing high-volume, low-acuity conditions locally, primary care clinics contribute to continuity of care and help reduce downstream burden on hospitals and referral facilities.
Policy Implications
The high proportion of preventable clinic visits underscores the potential impact of targeted preventive interventions delivered during routine primary care encounters. Nurse-led education, engagement of Lady Health Workers, and structured counseling on hygiene, nutrition, and early symptom recognition may be particularly effective in reducing avoidable morbidity among women and children.
Referral patterns emphasize the need for reliable referral systems and coordination between community clinics and higher-level facilities. Supporting standardized clinic-level data collection may enable evidence-informed resource allocation and service planning.
Future Research
Future studies could extend data collection over longer periods to examine seasonal variation and trends. Additional variables such as age subgroups or repeat visits could further refine understanding of utilization patterns. Evaluating preventive interventions and their impact on clinic visits and referral rates would also be valuable.
Limitations
This study was conducted at a single clinic and may not be generalizable. Preventability classifications were based on operational definitions rather than standardized criteria. Referral decisions reflected clinical judgment and resource availability. The descriptive design precludes causal inference.
Bias and Data Considerations
Potential sources of bias include classification bias in preventability assignment, selection bias related to clinic attendance, and information bias arising from routine documentation. Unmeasured confounders such as socioeconomic status and distance to care may have influenced findings.
Ethics Statement
This study utilized de-identified, aggregate service data collected for program evaluation purposes. No personal health information was accessed.
Funding Statement
This research received no external funding. Conflict of Interest
The authors declare no conflicts of interest.
Author Contributions
D.E. conceptualized the study, conducted data analysis, and drafted the manuscript.
H.E. assisted with data organization and analysis.
N.E. contributed to interpretation of findings and manuscript review.
S.N. supported oversight of results, contextual interpretation and manuscript revision.
All authors reviewed and approved the final manuscript.
Acknowledgements
The authors thank Mr. Michael Stephens, Upper School Faculty, Crescent School, for constructive guidance on the statistical design and analytic approach. The authors also acknowledge the clinical staff for assistance with data collection, and Refugee Girls Worldwide for support of community health initiatives.
Daniyal Elahi is a pre-medical student with a strong interest in primary care and public health. Through clinical shadowing and applied health research, he has explored how community-based clinics address preventable illness and support maternal and child health, reinforcing his commitment to pursuing medicine.
References
- Das JK, Siddiqui F, Padhani ZA, Khan MH, Jabeen S, et al. (2023) Health behaviors and care seeking practices for childhood diarrhea and pneumonia in a rural district of Pakistan: A qualitative study. PLoS One 18: e0285868.
- Memon Z, Zaidi S, Riaz A (2015) Residual Barriers for Utilization of Maternal and Child Health Services: Community Perceptions from Rural Pakistan. Glob J Health Sci 8: 47-57.
- Aftab W, Shipton L, Rabbani F, Sangrasi K, Perveen S, et al. (2018) Exploring health care seeking knowledge, perceptions and practices for childhood diarrhea and pneumonia in Pakistan. BMC Health Serv Res 18: 44.
- Starfield B (1994) Primary care and health outcomes: A conceptual framework. Milbank Q 72: 357-387.
- UNICEF/WHO (2025) Pakistan Maternal, Newborn and Child Health Profile. UNICEF Data.
- Huda M, Rabbani F, Shipton L, Aftab W, Khan KS, et al. (2023) Listening to Caregivers: Narratives of Health Seeking for Children Under Five with Pneumonia and Diarrhea: Insights from the NIGRAAN Trial in Pakistan. J Multidiscip Healthc 16: 3629-3640.
- Iqbal S, Maqsood S, Zakar R, Zakar MZ, Fischer F (2017) Continuum of care in maternal, newborn and child health in Pakistan: analysis of trends and determinants from 2006 to 2012. BMC Health Serv Res 17: 189.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.