Outcomes of Robotic Hiatal Hernia Repair with Doughnut Technique- A Multiple Centre Study
by Haris Konstantinidis1,2, Christos Charisis1,2, Christos Smyrlis1, Rozen Dimov3, Yiming Chen4, Long R Jiao4*
1Department of Robotic General and Oncologic Surgical, Interbalkan Medical Centre, Asclepius 10 str, 55535 Pylea, Thessaloniki, Greece
2Department of Robotic and M.I.S. General Surgery, American Institute of Minimally Invasive Surgery, Limassol, Cyprus
3Department of General Surgery Clinic, Hospital Kaspela, Plovdiv, Bulgaria
4Department of Academic Surgery, The Royal Marsden Hospital, Imperial College of London, United Kingdom
*Corresponding Author: Long R Jiao, Department of Academic Surgery The Royal Marsden Hospital 203 Fulham Rd., London SW3 6JJ, United Kingdom
Received Date: 08 April 2026
Accepted Date: 14 April 2026
Published Date: 16 April 2026
Citation: Konstantinidis H, Charisis C, Smyrlis C, Dimov R, Chen Y, Jiao LR, (2026) Outcomes of Robotic Hiatal Hernia Repair with Doughnut Technique- A Multiple Centre Study. J Surg 11: 11607 DOI: https://doi.org/10.29011/2575-9760.011607
Abstract
Background: Hiatal Hernia Repair (HHR) is routinely performed Laparoscopically (L-HHR). However, the robotic approach is gaining momentum replacing the laparoscopic approach to overcome difficulties related to poor vision and instrumentation in difficult cases to avoid intraoperative complications and conversion to open surgery. Furthermore, bioabsorbable meshes are used increasingly for HHR to reduce recurrence rates and avoid problems related to conventional non-absorbable synthetic meshes. The current multicentre study reports the outcome of robotic HHR (RA- HHR) in complex cases with our innovative ‘’Doughnut’’ technique by using a bioabsorbable Phasix™ ST.
Objective : A multicenter retrospective study to evaluate the safety, efficacy, and long-term outcomes of robotic HHR with Phasix™ ST mesh.
Methods: Between December 2017 and December 2024, a total of 507 patients who underwent RHHR with Doughnut technique using Phasix™ ST mesh across multiple centres were analyzed. All patients had either large and recurrent Hiatal Hernia (HH) or HH with prepositional factors. The large HH is defined as HH with a hiatal defect of 5 cm or more measured intraoperatively. Patient’s demographics, operative details, and postoperative outcomes were collected. The primary outcomes were hernia recurrence, mesh-related complications (infection, migration, erosion), and postoperative dysphagia. Statistical analyses included Kaplan-Meier survival curves and subgroup analyses for hernia size and primary vs. recurrent hernias.
Results: The cohort consisted of 247 females (48.7%) and 260 males (51.3%), with a median age of 54 years and median BMI of 28. The majority (91.3%) underwent primary RA-HHR while the rest recurrent HH with no prior mesh utilization (8.7%). The median operative time was 63 minutes, and there were no conversions to open surgery. At a median follow-up of 17 months, the recurrence rate was 1.4% without mesh-related complications. Transient dysphagia was observed in 5.7% of patients but all resolved spontaneously at the subsequent follow up. Recurrence-free survival at 24 months was 98.6%. No significant differences in recurrence rates were found when compared hernia size (>5 cm vs 3-5cm, p = 0.63) and primary with recurrent HHR (p = 0.47).
Conclusion: Robotic-assisted hiatal hernia repair with Doughnut technique using Phasix™ ST mesh offers a low recurrence rate.
Keywords: Hiatal Hernia; Hiatal Mesh Repair; Minimally Invasive Surgery; Phasix™ St; Robotic Hiatal Hernia Repair
Introduction
Robotic-Assisted Hiatal Hernia Repair (RA-HHR) offers enhanced precision through three-dimensional visualization and articulating instruments, potentially optimizing outcomes for complex cases [1] replacing both open and laparoscopic procedures. To reduce recurrence rates, mesh augmentation is used increasingly. While the traditional non-absorbable synthetic meshes such us polypropylene and polytetrafluoroethylene are associated with long-term risks of erosion, adhesion, and infection [2]. Bioabsorbable meshes such as the Phasix™ series have emerged as promising alternatives due to their ability to provide temporary mechanical support, minimizing foreign body retention risks through gradual degradation [3]. However, balancing anti-adhesion properties and durability remains controversial for absorbable meshes, particularly in complex or large hernias (>5 cm) [4]. Furthermore, the outcome of RA-HHR with bioabsorbable mesh such as Phasix™ ST [5] and high-risk populations in patients with obesity, chronic cough and recurrent hernias remains uncertain. Phasix™ ST, a novel bioabsorbable mesh, combines a Poly-4-Hydroxybutyrate (P4HB) scaffold with a hydrogel barrier designed to reduce visceral adhesions while maintaining sufficient tensile strength during tissue integration [6]. Preclinical studies demonstrate that its hydrogel layer significantly reduces adhesion formation, and the P4HB substrate degrades over 12–18 months, aligning with the critical tissue remodeling phase post-hernia repair[ [7]. Despite these advantages, clinical evidence for Phasix™ ST in human hiatal hernia repair in roboticassisted procedures remains limited with no multicenter studies to date. This multicentre study evaluates the safety and efficacy of Phasix™ ST in complex RA-HHR with Doughnut technique characterized by a 360-degree coverage of the hiatal defect. Clinical outcomes including recurrence rates and mesh-related complications were analyzed. In doing so, we are hoping to address the critical knowledge gaps and refine surgical strategies for HHR using a combination of robotic platform and advanced bioabsorbable materials.
Methods
Study Design and Patient Selection
This retrospective multicentre study included consecutive patients undergoing RA-HHR with the Phasix™ ST mesh (BD, Franklin Lakes, NJ) at participating institutions between December 2017 and December 2024. All surgeons have performed over 500 robotic upper GI procedures.
Inclusion Criteria:
- symptomatic hiatal hernia (type I–IV) confirmed by preoperative endoscopy or imaging
- primary or recurrent repair
- Hiatal defect /diameter ≥5 cm measured after full
dissection of the crura
- Hiatal defect / diameter 3-5 cm with coexisting risk factors such as obesity defined as BMI ≥30, chronic cough and heavy labor
Exclusion Criteria Included:
- emergency surgery
- concurrent major abdominal procedures such as bariatric surgery
- pregnancy.
The study protocol was approved by institutional review boards at all centers, and informed consent was waived due to retrospective design (Declaration of Helsinki principles followed) [8].
Surgical Technique
All procedures were performed using the da Vinci X® and Xi® robotic platforms (Intuitive Surgical, Sunnyvale, CA).
Patient Positioning and Port Insertion
Patients are positioned in the supine position with at least 15 degrees reverse Trendelenburg, and table lowered down for better ergonomics for the assistant surgeon. The legs are parted with the hips and knees slightly flexed; arms are tucked on the sides of the trunk. The surgical assistant sits or stands at the left of the patient. Pneumoperitoneum is induced with a supra umbilical Hassan technique which is used as the 8mm camera port - arm 1. Standardization of port placement is recommended, allowing for some variance based on the patient’s body conformation. The robot is docked cephalad or from the patient’s right side respectively for X and Xi systems. One robotic arm is positioned to the right of the camera port as arm 2, and two to the left of the camera port as arms 3 and 4 at least 5 cm apart in horizontal position. The 10 mm assistant port lies at the left mid axillary line and is used for suction, insertion of sutures, swabs, laparoscopic grasper and mesh insertion.
Robotic Instrumentation.
The authors’ preferred initial instrument insertion after the camera insertion in arm 2 is an ultrasonic device, bipolar fenestrated forceps in arm 3 and needle holder in arm 4 as a liver retractor initially. Arm 2 and 4 instruments swap when dissection finishes, to utilize the suturing reconstruction. Suction/irrigation device and grasping forceps are also used by the assistant in a laparoscopic manner.
Hernia Reduction and Crural Dissection – Doughnut Technique
The Doughnut technique was well described previously [9]. In brief, the initial step was the full retraction of hernia components back into the abdominal cavity, followed by a full excision of the hernia sac to reduce the risk of mesothoracic seroma formation. The diaphragmatic crura, as well as the abdominal and the lower thoracic esophagus, were fully dissected and exposed. The intraoperative greater diameter of the hiatus defect was taken for all patients for homogeneous measurements. In all patients, a primary closure of the hiatal defect was made with interrupted nonabsorbable sutures (Ethibond 2-0). In cases of large defects, sutures were also placed anterior to the esophagus, to avoid angulation of the esophagus, thereby reducing the risk of dysphagia. Once primary closure of the defect was achieved, an 8–10 cm-diameter round-shape PhasixTM ST mesh with a 2–2.5 cm central opening was placed circumferentially around the esophagus in an on-lay fashion, while hydrogel barrier faces viscera and adhesive part the crura. The mesh was fixed to the diaphragm either with interrupted sutures, or more common with a tucker device, with special care to avoid injuries of the aorta, the vena cava, and the pericardium. After the mesh was fixed, a standard 360° Nissen fundoplication completed the intervention. After removal of its central part the mesh, it resembles the shape of a doughnut, supporting circumferential the oesophageal hiatal defect, hence the name Doughnut (Figure 1).
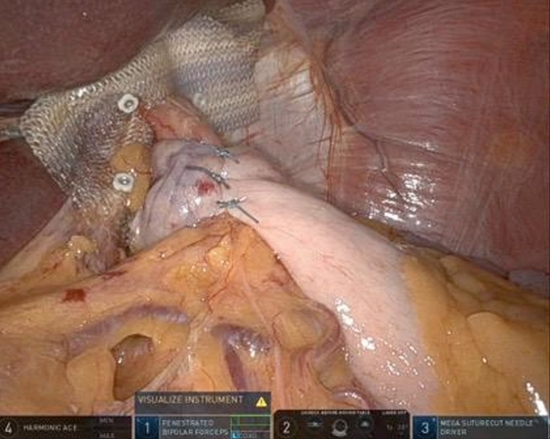
Figure 1: Doughnut repair.
Data Collection
Demographic, operative, and outcome variables were extracted from electronic medical records including preoperative data on age, sex, BMI, hernia type (primary vs. recurrent), size (categorized as 3–5 cm or >5 cm), and comorbidities, intraoperative data on operative time (skin-to-skin) and intraoperative complications, and postoperative data on hospital stay, 30-day complications (Clavien-Dindo classification [7]), dysphagia severity (Eckardt score [1]), hernia recurrence confirmed on endoscopy/CT, and mesh-related adverse events such as infection, migration, erosion.
Statistical Analysis
Continuous variables were expressed as median (range); categorical variables as frequencies (%). Recurrence-free survival was analyzed using Kaplan-Meier curves. Subgroup analyses compared outcomes for primary vs. recurrent hernias and hernia size (>5 cm vs. 3–5 cm) via Fisher’s exact test and Mann-Whitney U test. Statistical significance was set at p < 0.05. Analyses were performed using R v4.3.1 (R Foundation for Statistical Computing).
Results
Patient Characteristics
A total of 507 patients underwent robotic hiatal hernia repair with doughnut technique using Phasix™ ST mesh across participating centres. The cohort comprised 247 females (48.7%) and 260 males (51.3%) with a median age of 54 years (range, 27–76 years). Median BMI was 28 (range, 19.2–44). Primary repairs accounted for 463 cases (91.3%), while 44 (8.7%) were recurrent hernias. There were 367 cases (72.4%) with HH size defects >5 cm in diameter and 96 (18.9%) 3–5 cm with coexisting risk factors of obesity (12%), chronic cough (2,1%) and heavy labor (4,8%).
Operative Outcomes
Median operative time was 63 mins (range, 38–143 mins ) with no conversions to open surgery. All patients were discharged on the first postoperative day. There was no intraoperative complications in 506 cases (99.8%) but one patient had minor bleeding from a short gastric vessel which was controlled robotically without transfusion.
Postoperative Outcomes
At a median follow-up of 17 months (range, 3–24 months), recurrence was identified in 7 patients (1.4%), all presenting with mild symptoms of episodic acidic reflux which were managed conservatively without reoperation. Transient dysphagia defined as Eckardt score ≥3 occurred in 29 patients (5.7%) which resolved spontaneously within a median of 3 months (range,1–6 months). No mesh-related complications were observed. At follow up, one patient was diagnosed with prepyloric gastric cancer at 6 months postoperatively and treated with robotic subtotal gastrectomy. There was no major adhesion found around the mesh. One patient developed early distal esophageal cancer at 12 months who required subsequent oesophagectomy at another centre. At subgroup analysis of this cohort of patients who underwent RA-HHR with bioabsorbable Phasix™, there was no difference in recurrence rate comparing HH >5m with that 3-5cm with coexisting factors (5/367, 1.4% vs 2/96, 2.1% respectively. p = 0.63) and primary with recurrent HH repair (6/463, 1.3% vs 1/44, 2.3% respectively. p = 0.47). At 24-month follow up, the recurrence-free survival was 98.6% (95% CI: 97.1–99.4%) (Figure 2).
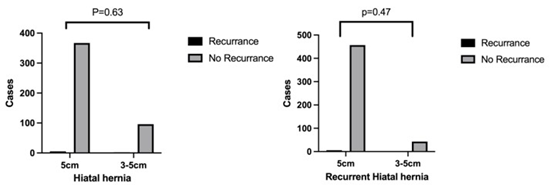
Figure 1: Recurrence rate based on the size of the hiatal hernia.
Discussion
This multicentre study demonstrates that robotic hiatal hernia repair with Phasix™ ST mesh achieves low recurrence rates (1.4%) and no mesh-related complications. This was achieved in both primary and recurrent cases with hernia size >5cm. Our results compare favorably with the historical data for nonabsorbable mesh report of the recurrence rates of 5–15% and mesh erosion risks of 1–3% over a similar length of follow-up [10]. The absence of mesh-related adverse events aligns with preclinical studies highlighting Phasix™ ST’s hydrogel barrier as a critical innovation for reducing visceral adhesions and erosion risks [11]. Notably, transient dysphagia (5.7%) resolved spontaneously in all cases, suggesting that postoperative inflammation rather than mesh rigidity may drive early swallowing dysfunction, a hypothesis supported by animal models of absorbable mesh integration [11]. When compared with laparoscopic series of median operative time of 90–120 minutes, our result showed that this could be achieved with 63 minutes demonstrating clearly the efficiency of robotic assisted hiatal hernia repair with its superiority over laparoscopic repair in terms of vision and instrumentation for complex upper GI operations as we see increasingly in other subspecialties once surgeons are over the learning curve for robotic surgery [12,13]. Robotic platform can offer an enhanced dexterity in mediastinal dissection and mesh fixation. This is further supported by zero conversion to open surgery compared with laparoscopic surgery of conversion rates of 2–5% for large hernias [14]. The result is further supported by the similar findings of robotic vs laparoscopic cholecystectomy for complex tertiary referral gallbladder operation [12]. Our result showed a now recurrence rate in high-risk subgroups. This challenges the conventional concerns about absorbable mesh durability. Phasix™ ST’s 12–18-month degradation timeline [1] appears sufficient to bridge the critical tissue remodeling phase, while avoiding long-term foreign body risks. This aligns with Roth et al.findings in ventral hernia repair, where Phasix™ maintained mechanical integrity until 12 months post-implantation [15]. However, longer follow-up (>24 months) is needed to confirm these results, as late recurrences may emerge beyond the mesh degradation period. In our cohort, there were two cases of incidental malignancies (gastric and esophageal cancers) identified during follow-up which were consistent with populationlevel cancer incidence rates [14] but highlighted the importance of routine postoperative surveillance in patients with hiatal hernia who often harbor comorbidities such as obesity and GERD which are associated with gastrointestinal malignancies [16].
Limitations
First, the retrospective design introduces potential selection bias though standardized inclusion criteria across centres mitigate this risk. Second, median follow-up of 17 months precludes assessment of very late recurrences (>3 years). Third, the predominance of primary repairs (91.3%) limits generalizability to recurrent hernia populations. We feel that the future will be robotic surgery which will inevitably replace laparoscopic surgery. As such, it is important to adequately expose and train surgical fellows to robotic surgery. Additionally, cost-effectiveness analyses should evaluate whether reduced complication rates, length of stay and conversion rate to open operation will offset the higher initial cost of robotic surgery and bioabsorbable meshes.
References
- Soliman B G (2020) “Robot-assisted hiatal hernia repair demonstrates favorable short-term outcomes compared to laparoscopic hiatal hernia repair,” Surg. Endosc 34: 2495-2502.
- Oelschlager B K (2006) “Biologic prosthesis reduces recurrence after laparoscopic paraesophageal hernia repair: a multicenter, prospective, randomized trial,” Ann. Surg 244: 481-490.
- Deeken C R, Abdo M S, Frisella M M, Matthews B D (2011) “Physicomechanical evaluation of absorbable and nonabsorbable barrier composite meshes for laparoscopic ventral hernia repair,” Surg. Endosc 25: 1541-1552.
- Nie Y (2021) “Laparoscopic fixation of biological mesh at hiatus with glue and suture during hiatal hernia repair,” BMC Surg 21: 158,
- Panait L, Novitsky Y W (2017) “Hiatal Hernia Repair: Current Evidence for Use of Absorbable Mesh to Reinforce Hiatal Closure,” Surg. Technol. Int 30: 182-187.
- C. R. Deeken C R, Matthews B D (2013) “Characterization of the Mechanical Strength, Resorption Properties, and Histologic Characteristics of a Fully Absorbable Material (Poly-4-hydroxybutyratePHASIX Mesh) in a Porcine Model of Hernia Repair,” ISRN Surg 2013: 238067.
- Deeken C R, Chen D C, Lopez-Cano M, Martin D P, Badhwar A (2023) “Fully resorbable poly-4-hydroxybutyrate (P4HB) mesh for soft tissue repair and reconstruction: A scoping review,” Front. Surg 10: 1157661.
- World Medical Association (2013) “World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects,” JAMA 310: 2191-2194.
- Konstantinidis H, Charisis C (2023) “Surgical treatment of large and complicated hiatal hernias with the new resorbable mesh with hydrogel barrier (PhasixTM ST): a preliminary study,” J. Robot. Surg 17: 141-146.
- Watson D I (2020) “Five Year Follow-up of a Randomized Controlled Trial of Laparoscopic Repair of Very Large Hiatus Hernia With Sutures Versus Absorbable Versus Nonabsorbable Mesh,” Ann. Surg272: 241247.
- Shi K, Xue B, Liao J, Qu Y, Qian Z (2017) “Polymeric hydrogels for post-operative adhesion prevention: A review,” Mater. Express 7: 417438.
- Kawka M (2025) “Robotic versus laparoscopic cholecystectomy for difficult gallbladders: an observational study of tertiary centre cases,” Surg. Endosc 39: 2958-2963.
- Ding H (2023) “Robotic Distal Pancreatectomy Yields Superior Outcomes Compared to Laparoscopic Technique: A Single Surgeon Experience of 123 Consecutive Cases,” Cancers 15: 5492.
- Lindmark M, Strigård K, Löwenmark T, Dahlstrand U, Gunnarsson U (2018) “Risk Factors for Surgical Complications in Ventral Hernia Repair,” World J. Surg 42: 3528-3536.
- Roth J S (2022) “Long-Term, Prospective, Multicenter Study of Poly4-Hydroxybutyrate Mesh (Phasix Mesh) for Hernia Repair in Cohort at Risk for Complication: 60-Month Follow-Up,” J. Am. Coll. Surg 235: 894-904.
- Schlottmann F, Dreifuss N H, Patti M G (2020) “Obesity and esophageal cancer: GERD, Barrett´s esophagus, and molecular carcinogenic pathways,” Expert Rev. Gastroenterol. Hepatol 14: 425-433.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.