New Frontiers in the Evolution of Minimal Invasive Surgery (MIS) and Artificial Reproductive Technologies (ART) 1965 - 2025
by Liselotte Mettler*
Department of Obstetrics and Gynecology, University Clinics of Schleswig Holstein (UKSH), Arnold Heller Strasse 3, Haus C, 24105 Kiel, Germany
*Corresponding author: Liselotte Mettler, Department of Obstetrics and Gynecology, University Clinics of Schleswig Holstein (UKSH), Arnold Heller Strasse 3, Haus C, 24105 Kiel, Germany
Received Date: 08 November 2024
Accepted Date: 14 November 2024
Published Date: 16 November 2024
Citation: Mettler L (2024) New Frontiers in the Evolution of Minimal Invasive Surgery (MIS) and Artificial Reproductive Technologies (ART) 1965 - 2025. J Surg 9: 11181 https://doi.org/10.29011/2575-9760.11181
Abstract
In this article for Journal of SURGERY we focus on “molecular aspects” but also deal with the macroscopic realistic developments that enabled us to recognize and use health improvements by starting on the molecular level for surgery. Molecular imaging technologies are increasingly used to diagnose, monitor, and guide treatment in various gynecological performances for. the treatment of infertility, cancer and many others. In this review, the history, current status, and future prospects of the use of molecular technologies as instrument to help realize precision treatment with Minimal Invasive Surgery - MIS - and Artificial Reproductive Technologies -ART - are summarized.
With 60 years of development, both of these technologies are well established and ready to be improved by applying molecular imaging and molecular genetic technologies. The surgery is addressed with focus on the main components that form the conceptual basis of intraoperative molecular imaging. Paramount for successful interventions is the relevance and accessibility of surgical targets. Preimplantation genetic testing is commonly performed in conjunction with IVF. It refers to various genetic assays performed on embryos before transfer to identify possible genetic disorders. For example, preimplantation genetic testing for aneuploidy (PGT-A) screens for whole chromosome abnormalities, whereas preimplantation genetic testing for monogenic disorders (PGT-M) screens for single-gene disorders in high-risk patients. In addition, selection of the correct combination of imaging agents and modalities is critical to visualize both microscopic and bulk disease sites with high affinity and specificity. In this context developments within engineering/imaging physics continue to drive the improvement of Image-Guided Surgery and Artificial Reproductive Technologies.
Keywords: Artificial Reproductive Technologies (ART); Current realities in MIS and ART and future aspects on molecular basic structures in MIS and ART; Minimal Invasive Surgery (MIS); Molecular Genetic Basis (MGB)
Introduction
Minimal Invasive Surgery (MIS)
The development of Minimal Invasive Surgery (MIS) started multidisciplinary in medicine over 200 years ago. However, the real ground stone was set by Georg Kelling in 1903 at the Natural Scientists meeting in Hamburg, Germany, when he performed the world’s first endoscopic exploration looking into the stomach of a dog, using air insufflation and Nitze’s cystoscope [1,2]. Later in the 20th century, French and German gynecologists, Raoul Palmer, Hans Frangenheim, Kurt Semm, Hans Lindemann and Jacques Hamou, set milestones for laparopscopy and hysteroscopy [3]. As a contemporary witness, it is my pleasure to share with you some features of endoscopic surgery, what later became known as Minimal Invasive Surgery (MIS). This surgical approach soon spread from gynecology to all medical disciplines, particularly into general surgery in the late 1980s. As gynecologists, we performed the first laparoscopic appendectomy in Kiel in 1981 [4,5]. Later, general surgeons, urologists and all surgical medical specialties widened the field in a glorious way. The technical development in instrumentation, apparatuses, optics, lenses and lens systems, energy sources, suturing, minimalization, digitalization and artificial intelligence led to today’s open field of endoscopic surgery in procedures of benign cases as well as in malignancies [6] Kurt SEMM went from diagnostic to operative gyne-endoscopic surgery and described hysterectomies in the same time frame as Harry Reich in the USA. Camran Nezhat was the first to publish on video laparoscopy [7].
Today we have long time entered into adding molecular imaging technologies increasingly into the field to diagnose, monitor, and guide treatment specifically in cancer cases. In this direction, the current status and future prospects of the use of molecular imaging as an instrument to help realize precision surgery is addressed with focus on the main components that form the conceptual basis of intraoperative molecular imaging. Very important for successful interventions is the relevance and accessibility of surgical targets. In addition, selection of the correct combination of imaging agents and modalities is critical to visualize both microscopic and bulk disease sites with high affinity and specificity. In this context developments within engineering/imaging physics continue to drive the growth of image-guided surgery. Particularly important herein is enhancement of sensitivity through improved contrast and spatial resolution, features that are critical if sites of cancer involvement are not to be overlooked during surgery. By facilitating the connection between surgical planning and surgical execution, digital surgery technologies such as computer-aided visualization successfully complement these technologies. Diagnostic and operative hysteroscopy started with Hans Lindemann, Kurt Semm and Jacques Hamou [8-10], also in the 1980s.
Endoscopic surgery started with a bent position of the surgeon, looking directly through a laparoscope, to video laparoscopy in a comfortable standing position and more recently to robotic assisted laparoscopic surgery in a sitting position with more to come like automatic surgery with high precision and artificial intelligence support, always following the rules of our Greek doctor and philosopher Hippokrates [11] who said, be courageous in surgery but do not hurt.
Artificial Reproductive Technologies (ART)
This fascinating field started with multinational publications in the 1960s, mainly from our British colleagues, Robert Edwards and Patrick Steptoe. The following citations are mentioned in this special issue directly in the text, as they express best the long preparation towards increasing the understanding for this technology (1965-1978):
- Edwards RG: Maturation in vitro of human ovarian oocytes. Lancet 1965;2,926-92
- Steptoe P: Laparoscopy and ovulation. Lancet 1968;2,913
- Steptoe PC, Edwards RG: Laparoscopic recovery of preovulatory human oocytes after priming of ovulation with gonadotrophins. Lancet 1970;1,683-689
- Steptoe PC, Edwards RG: Reimplantation of a human embryo with subsequent tubal pregnancy. Lancet 1976:1,880-882
- Steptoe PC, Edwards RG: Birth after reimplantation of a human embryo. Lancet 1978:2,366
After the British successes in the years 1980-1981, IVF pregnancies were described around the world (England, Australia, USA and India). In September 1981, Patrick Steptoe and Robert Edwards invited their friends, clinicians and researchers from around the world to the “First Bourne Hall Meeting” with 25 participants from around the world
Five concepts were developed that guide IVF protocols and procedures until today:
- Stimulated cycles are better than natural cycles for a better number of oocytes and better prediction of ovulation, HMG, 1984 pituitary downregulation (GnRh agonists- flare up effect). The historical perspectives in gonadotrophin therapy are best detailed by Bruno Lunenfeld: Human Reproduction Update, Volume 10, Issue 6, November/December 2004, Pages 453-467. Donini with the purification of FSH, Andrew Shally, Arimura and Castin with the synthesis of GnRH play a leading role in it.
- Ultrasonography to monitor the growth of follicles
- Focus on Embryo Transfer (ET)/ progesterone for luteal phase support - start on the day of follicular puncture
- Control of culture media and laboratory procedures is essential.
- Effect of CO2 on oocyte quality with laparoscopy was found not to be good, all ovum pick-ups in these early years were done under laparoscopic vision with the use of CO2 abdominal insufflation, the pressure was kept as low as possible and the needle injection done quickly.
However, ART has revolutionized the field of reproductive medicine by offering new possibilities for individuals and couples to conceive and have children of their own. For example, ART can help individuals overcome issues such as blocked fallopian tubes, male factor infertility (including low sperm count or motility), and age-related fertility decline. By using ART, individuals and couples can increase their chances of achieving a successful pregnancy and experiencing the joys of parenthood.
Facts and developments of Endoscopic Surgery / Minimal Invasive Surgery in Gynecology and Artificial Reproductive Technologies (ART)
Minimal Invasive Surgery (MIS)
Based on the milestones in the development of endoscopic surgery, today’s modern surgical achievements can be well understood and are being continuously further developed. All the following colleagues have already passed away, but their achievements still guide us today:
1) Philipp Bozzini (1773 - 1809) and the light guide
2) Antonin Jean Desormeaux (1815 - 1894) and his endoscopes
3) Georg Kelling (1866 - 1945) and his air insufflation apparatus
4) Max Nitze (1848 - 1906), an early urological endoscopist who developed cystoscopy
5) Heinrich Kalk (1895 - 1973) and his insufflation apparatus which allowed abdominal biopsies of the liver etc.
6) Raoul Palmer (1904 - 1985), the European father of endoscopy in the lithotomy position
7) Hans Frangenheim (1920 - 2001) built his first abdominal insufflator in 1959
8) Harold Hopkins (1918 - 1994) developed the rod lens system of Modern endoscopes
9) Karl Storz (1911 - 1996) was responsible for the development of the cold light source in 1960
10) Patrick Steptoe performed many laparoscopies in Great Britain and developed the human in vitro fertilization and embryo transfer technique (IVF - ET) together with Robert Edwards
11) Hans-Joachim Lindemann, born in 1920, laid the groundwork for hysteroscopy
12) Kurt Semm (1923 - 2003), the father of operative gynecological endoscopy
13) Erich Mühe (1938 - 2005) first cholecystectomy - however, Philippe Mouret (born 1938) from Lyon, France is worldwide known for his first cholecystectomy in 1987 as he was able to publish it.
14) Jordan M. Phillips (1923 - 2008), propagator and “prophet” for gyne-endoscopic surgery worldwide.
15) Maurice Bruhat (1934 - 2014)
16) Thoralf Schollmeyer (1962 - 2014)
17) Peter John Maher (1940-2023)
The last 60 years - a rocky road, what do I know about it and who are the present and future giants in our field? [6].
There arises the question what gives life and a certain professional field a meaning? It is always only the connection to human beings in our field, colleagues, co-workers and technical advisers that make our work meaningful. Just as life is full of adventures, sadness and joy, also the field of endoscopic surgery experienced its ups and downs over 60 years before finally finding the wide acceptance of today. It was a rocky road, and many surgeons had to accept blasphemy, professional inconveniences and mistrust but of course also a lot of understanding, joy, success and acceptance from patients, colleagues, hospitals, governments and families. Unlike in any other field the international family of colleagues and friends in this field has grown rapidly and it is interesting how everyone has given new contributions into this evolution.
Still active in our profession today are : Harry Reich, Jacques Hamou, Jacques Donnez, Denis Querleu, Mark Possover, Arnaud Wattiez, Christopher Sutton, Ray Garry, Ellis Downes, Frank Loffer, Tom Lyons, Camran Nezhat, Farr Nezhat, Ceana Nezhat, Robert Zuravin, Linda Bradley, Karl-Werner Schweppe, Diethelm Wallwiener, Hans Tinneberg, Ivo Meinhold-Heerlein, Ibrahim Alkatout, Günter Noe, Goentje Peters, Johannes Ackermann, Bernd Holthaus, Thilo Wedel, Bruno van Herendael, Prashant Mangeshikar, Prakash Trivedi, Bhaskar Goolab, Artin Ternamian, Chi Long Lee, Hirohiko Yamada, Robert O’Shea, Adel Shervin,
Lotte Clevin, Linda Michels, Maurice Abrao, Michelle Canis, Ted Anderson and many others. Kurt Semm dedicated his life to the development of endoscopic surgery. Today endoscopic surgeons form a big medical technical family with increasing success in the treatment of patients.
In the 21st century according to the rapid development in the past century 80% of gynecological surgical procedures are performed by Minimal Invasive Surgery
MIS, which is still often referred to wrongly as keyhole surgery, allows u to perform procedures with smaller incisions but better vision. It results in less pain, faster recovery times and lower complication rates for patients. We have already made significant advances in gynecological practice, particularly in the treatment of conditions such as, endometriosis, fibroids, ovarian and adnexal tumors and in the performance of hysterectomies in laparoscopy and in the treatment of polyps, fibroids, adhesions and congenital uterine anomalies (CUA) in hysteroscopy. The ability to operate with just a few small incisions has not only improved the patient’s positive experience but also increased the efficiency of these procedures. Several areas in gynecological malignancies, such as radical hysterectomies and lymphadenectomies, have been performed for 20 years by MIS but are still under evaluation. MIS is already part of the medical student’s curriculum with surgical procedures in several countries globally. Laparoscopy training on the pelvi-trainer was established as an integral part of the medical curriculum in many Medical Schools. The ongoing positive evaluations of students also support the maintenance of these courses in the future. It was possible to show that it is possible to implement a concept of this nature sustainably and permanently. The multilevel training concept could be easily implemented. Modern media permit exchange and comparisons between students and teachers. The integration of MIS training programs in medical curricula will expand and intensify the scope of medical education as well as improve the skills of future surgeons [6].
Many national and global societies have developed to guide training performances, such as the European Society of Gynecological Endoscopy (ESGE), the American Society of MIS and Robotic Surgery (AAGL), the Asian Pacific Association of Gynecological Endoscopy (APAGE) and the International Society of Gynecological Endoscopy (ISGE).
Artificial Reproductive Technologies
Controlled ovarian hyperstimulation has been addressed by many authors [12-30]. What has happened in the last 4-5 decades (19802025) in ART?
1980 - 1981: The first IVF pregnancies were described around the world and the beginning of international experience exchange - ESHRE, IVF Annual meetings, ASRM, etc. Between 1982- 1988 transvaginal ultrasound guided follicular puncture was developed. Initial trials described transvesical follicular aspiration, but quickly the transvaginal way was found by Wikland, M. et al.: Collection of human oocytes by the use of sonography. Fertil Steril 1983,39,603-608. There were also many other publications, e.g. on Gamete Intra Fallopian Tube Transfer and Zygote Intra Fallopian Tube Transfer (GIFT, ZIFT). However, the breakthrough came with Sub Zonal Sperm Injection and Intra Zytoplasmatic Sperm Injection (SUSI/ICSI), developed in 1986 (Palermo).
1990 - 2000: Pharmaceutical advancement, better fertilization techniques, ultrasound guided embryo transfer, vitrification, trophectoderm biopsy for genetic screening with PCR, sex determination of the fetus. Handyside, A et al. Pregnancies from human preimplantation embryos sexed by Y specific DNA amplifications Nature 1990, 344,768-770. MESA, microsurgical epididymal sperm aspiration, TESE (Testicular Sperm Extraction) and micro TESE, in vitro maturation (IVM) was developed, GnRH antagonists, rec. FSH and LH.
2000 - 2010: Technological improvements and international knowledge transfer, protocol improvements, donor oocytes and donor embryos, surrogacy, cryoconservation of ovarian and testicular tissue.
2010 - 2025: Here we talk about the freezing of embryos for transfer in a consecutive cycle (freeze all concept). Pregnancy rates are better as we transfer without hyperstimulation.
Next Generation Sequencing (NGS) and other technologies continue. We learn more about inheritance of disease by ART and the medical tourism and third-party involvement is growing.
We nearly overcame COVID 19, AIDS and HIV but are still confronting cases. There is a lot of talk about artificial gametes and artificial placenta. Stem cell concepts are continuously discussed and developed. Finally, let us be aware of what we have learned for good practice in ART. It is important to know the ovarian reserve, understand controlled ovarian hyperstimulation and perform a safe transvaginal follicular puncture of oocytes. The embryo transfer is performed under ultrasound control with a filled bladder into the uterine cavity at about 1cm distance to the uterine fundus. We understand successful embryology, preimplantation genetics and screening (PGTA and PGTS) and preimplantation genetic testing is almost routinely performed in modern IVF centers.
Current Situation of MIS and ART
State of MIS in 2024
Good surgery. has goals that are identical whether laparotomy, laparoscopy or endoscopic procedures are performed; regardless of the angle, location or means of access. They are identical for all fields of endoscopic surgery reaching today into robotic single and multiple port surgery [6]
Robotic tools, three-dimensional vision and force feedback are essential features in surgery. They make surgery more precise and easier. The surgical goals remain as:
- Recognition of relevant pathology
- Possibility of radical treatment in endometriosis and cancer
- Minimal trauma, bleeding and tissue laceration
- Adhesion prevention
- Preservation of urogenital tract in women of reproductive age
- Utilization of the best instruments (with as many degrees of liberty as possible, robotic transmission, etc.)
- Preventing organ decent
While moving towards image guided augmented reality surgery with increasing molecular recognition of tissue surgeons continue along the path of minimal trauma, maximum vision and good tactile feeling to come to ensure optimal surgical success until the time of better image-guided surgery, the application of “magic bullets” to destroy cancer without side effects becomes reality and better molecular-genetic recognition of disease makes extensive surgeries unnecessary in the future. Tissue extraction in contained bags or as homogenized tissue, to be genetically and by proteomics examined after its extraction, will hopefully finally be easily possible. Surgery with minimal bleedings, with articulated and robotic instruments with multiple degrees of liberty and precision coagulation is necessary. Computer-assisted instruments tips will allow the surgeon to position the angles to the desired tissue planes and give tactile feedback.
Only with good knowledge of “clinical anatomy” endoscopic surgical procedures (Figure 1) can be understood. The training of laparoscopic surgery on body donors definitely enriches all learning efforts (Figures 2 and 3). When teaching on body donors there is no time pressure, which - of course - at life surgical demonstrations has to be discussed. Figure 4 shows the final surgical situation after SLH (Subtotal Laparoscopic Hysterectomy) performed in a body donor compared to a patient.

Figure 1: Clinical anatomy of the minor pelvis.
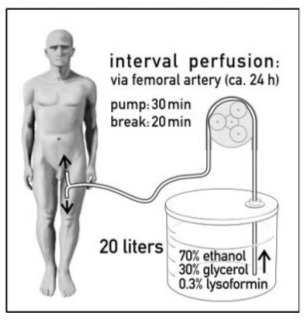
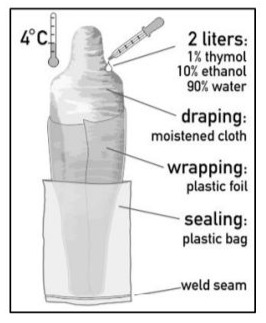
Figure 2: 2a: Interval perfusion mechanism 2b: Interval perfusion mechanism in body donors via femoral artery. on body donors with ethanol glycerol.

Figure 3: Ibrahim Alkatout and Johannes Ackermann operating in the Kiel Anatomy Department on a body donor by laparoscopy.
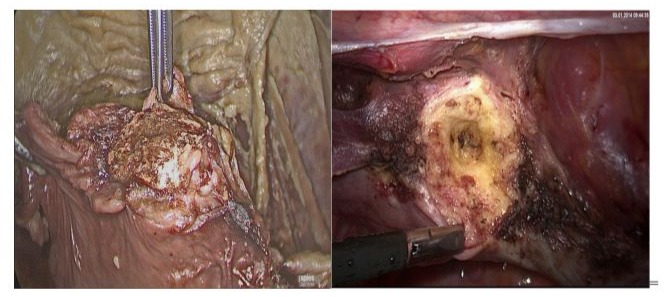
Figure 4: Cervical stump after a body donor Laparoscopic Subtotal Hysterectomy (LSH) (4a) in comparison to a patient LSH (4b)
From a chemical perspective, most of the efforts towards designing disease specific imaging agents find their origins in nuclear medicine and its subdiscipline of radiochemistry. Radiology guided surgery applications for sentinel nodes (radiocolloids, somatostatin receptor overexpressing lesions (peptides, and prostate specific membrane antigen (PSMA) expressing lesions (small molecules, have established. This is primarily driven by the common availability of tracer generators in clinics worldwide. This further focused tracer design, with recent examples of widely implemented agents is currently investigated in detail [31]. Besides the application-specific design of radiotracers there are various attempts to use off-the-shelve PET tracers for image guidance by exploring gamma rays [32,33], and beta particles Advantages of the use of radiotracers are that they can be applied under a micro-dosing regime, are compatible with quantitative biodistribution studies and support non-invasive pre-operative imaging approaches such as scintigraphy, single photon emission computed tomography (SPECT) and PET.
State of ART in 2024
Ten million babies and more have now been born around the world with the help of ART, worldwide 1-5 % of babies are born after an ART treatment. At ESHRE 2024 in Amsterdam, the European Society of Human Reproduction and Embryology held its 40th anniversary annual meeting from July 7 to 10, 2024. With more than 1120 posters and oral presentations, ESHRE 2024 celebrated successes from across the reproduction and embryology field.
At the first ESHRE meeting in Bonn, Germany in 1984 about 40 delegates from around the world gathered and had big dreams. Bob Edwards stated, ESHRE will be great one day” and here we are. At many press conferences in Germany and worldwide ART was established and defended (Figures 5 and 6).
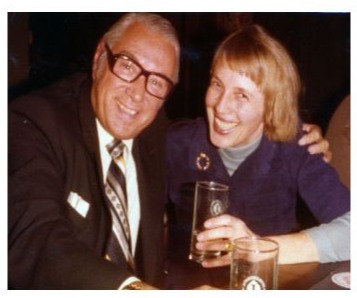
Figure 5: Patrick Steptoe and Lilo Mettler in an interview at the first ESHRE meeting in Bonn in 1984.
Figure 6: Bob Edwards and Lilo Mettler in 1982 after the announcement of the first IVF baby born in Kiel.
Some of the highlights from the 2024 ESHRE conference were:
- No increased risk of serious adverse events after fertility preservation in women with cancer
- An update on the Endometriosis Longitudinal Fertility Study (ELFS)
- The Copenhagen *Pregnancy Loss study”: More than 30 million pregnancy losses are reported to occur every year, effecting around 25% of pregnancies, yet, despite this, the mechanisms behind pregnancy loss are not fully understood. The previous idea that pregnancy loss is a result of fetal genetics does not paint a true picture. Although fetal genetics are understood to cause the loss in a majority of cases (5060%), a non-genetic cause is thought to be responsible in a substantial number of losses (40-50%) as well.
- Phase 2 clinical trial results for an innovative “aldehyde derivative”, a non-hormonal substance, OXO-001 were presented. OXO-001 seems to be active on the level of the endometrium. The Phase 2 trial involved 96 women up to 40 years old, all of whom received donor eggs for single embryo transfer. The trial was double-blinded and randomized, comparing the effects of OXO-001 to a placebo. The results were encouraging: 75.9% of women who took OXO-001 had a biochemically confirmed pregnancy, compared to 52.4% in the placebo group. Clinically confirmed pregnancy rates, ongoing pregnancy rates, and live birth rates all showed marked improvements with OXO-001 pretreatment.
Specifically, the ongoing pregnancy rate at ten weeks post-embryo transfer was 46.3% for OXO-001 users, compared to 35.7% for those on the placebo. The live birth rate was also higher for OXO001 at 42.6%, compared to 35.7% for the placebo. Although these results were not statistically powered to confirm significance, they provide good reason to continue to a Phase 3 trial.
Future visions and logical features come with technological development, Artificial Intelligence (AI) and ethical acceptance
MIS in the next 25 years (2025-2050)
The future is based on the history of laparoscopy which is a unique mixture of various trends in different fields, spurred by the activities of established societies as well as opportunities of their publication and influenced by the world’s progress, recession, war, piece and the love of the individuals for life. The influence of industry, which has kept pace and actively supported this development for years, is the driving force besides the heroes of doctors and engineers that introduce new ideas. Without suitable technology, this dissemination would not have been possible. Endoscopic development and its future do depend on new inventions, on the audacity of leading heroes, their input into this field but also on their management of life to continue to survive and in a healthy and successful cooperation with the medical technical industry and the governments of our countries which grant us the peace and freedom for new achievements.
The integration of robotics into surgery has further advanced this development. Robot-assisted systems provide precise control and allow us to perform complex procedures with a level of accuracy that is often unattainable with traditional methods. The 3D visualization and improved mobility of the instruments allow us to get into hard-to-reach areas of the body while sparing the surrounding tissue. This is particularly important in gynecology, where the anatomy is often complex and variable. Another advantage of robotic surgery is the ability to improve ergonomics during the procedure. A surgeon can work in a more comfortable sitting position which reduces fatigue and maintains concentration during longer operations. This not only leads to better results for the patients, but also to greater satisfaction for the surgeons.
The future of minimally invasive and robotic surgery will also be shaped by technological innovation, and artificial intelligence (AI). AI will play an increasingly important role by helping us plan procedures and analyze real-time data during surgery. AIsupported systems can recognize patterns in patient data that help us to create individual treatment plans based on the specific needs of each patient. This personalized approach could significantly improve outcomes and further reduce complication rates. In addition, AI will be able to perform precise analysis during surgery by evaluating image data in real time. This could help us to identify potential problems early and make immediate adjustments. The combination of robotic surgery and AI will take the precision and safety of our procedures to a new level. Another exciting aspect is the possibility of remote surgery. With the advancement of robotics and communication infrastructure, surgeons already are able to perform procedures remotely, which could be of great benefit to domestic or underserved areas in particular. This would greatly improve access to specialized surgical procedures and could help to make healthcare more equitable around the world.
In summary, the future of minimally invasive and robotic surgery is bright, and the combination of innovative technologies, AI and robotic systems will not only revolutionize the way we operate, but also significantly improve patient experience and outcomes. All surgeons are looking forward to being part of this exciting development and taking full advantage of the opportunities that the future offers. Continuous training and adaptation to new technologies will be crucial to ensure that we can provide the best possible care to our patients.
ART New achievements and challenges 2025-2050
It is absolutely not the intention of this paper to go into a discussion on the future of fertility with ideas of revolutionizing human reproduction as stated by Emily Witt in 2023, and many others where she leads a discussion on researchers that are attempting to produce oocytes without human ovaries. This discussion on sperm cells is already around a bit longer. Technically in oocyte retrieval a more or less automated and very exact follicular puncture, can be foreseen, automated laboratory processment of gametes and embryos and an automated embryo transfer, based on previous imaging measurements.
Like the first successful IVF outcome with the delivery of Louise Brown in 1978, the Japanese experiment of reproductive biologists, Katsuhiko Hayashi and Mitinori Saitou in 2016 may challenge the science of human reproduction. They published in Nature that they produced oocytes from skin of the tip of a mouse tail, reprogrammed them into stem cells and then turned those stem cells into egg cells (oocytes). The eggs, once fertilized, were transferred to the uteruses of female mice, which gave birth to ten pups; some of the pups went on to have babies of their own. Hayashi and Saitou provided the first proof of what’s known as invitro gametogenesis (IVG), the production of gametes outside the body. The mice that descended from the lab-made egg cells were described as “grossly normal” [34].
The introduction of AI in ART procedures will revolutionize reproductive techniques, but it will definitely need a cautious and thoughtful approach, particularly when drafting legislative and regulatory frameworks solidly grounded in ethics precepts and core values, prioritizing human dignity and upholding fundamental rights to privacy, data protection, and equality. Continuous publications detail latest findings and discuss possible dangers [35-39]. Ultimately, such goals can only be achieved by preserving human control in order to make AI meet our needs, while at the same time operating transparently and achieving equitable outcomes.
Only a few factors are essential to a successful aspiration of healthy Metaphase-2 oocytes (egg retrieval). Priority has the controlled ovarian hyperstimulation as detailed in a 2024 publication on the subject [39].
Secondly, technical details have to be observed like:
- Setting the right aspiration pressure depending on the thickness of the utilized needle (gauge)
- Applying continuous vacuum suction before penetrating the follicles
- Maintaining a stable pressure throughout the entire procedure
- Avoiding applying negative aspiration pressure when withdrawing the needle from the follicles.
With exact imaging, AI and robotic control of the movements, automated egg retrieval will come soon.
Summary
Molecular basis for MIS and ART. Where have we come from and where are we going?
Multi-omic experimental approaches are revolutionizing the field of biological and medical sciences, opening new possibilities for understanding complex diseases and improving health care. These technologies analyze multiple types of biological information, such as genomics, transcriptomics, proteomics, metabolomics, etc, to gain a comprehensive understanding of biological systems. In MIS with all the robotic assistance advances and in ART with all the achieved success rates new approaches are expected, which ensure automated, programmed MIS, follicular punctures, embryo transfers as well as genetically based ovarian hyperstimulation. An advanced three-dimensional machine vision system is essential in making intelligent surgical robots smarter and safer. As the medical field moves towards more laparoscopic approaches for surgeries, it will be important to have an automated robotic system designed to assist such procedures.
Robotic anastomosis in bowel surgery, for example, is one way to ensure that surgical tasks that require high precision and repeatability can be performed with more accuracy and precision in every patient, independent of surgical skill. Staplers already exist, but more programmatic imaging assessments are required. The plan is a unique surgical approach to patient care with more predictable and consistent patient’s outcome. In ART, genomicbased recognition on best ovarian hyper- stimulation with optimal outcome for automated ovum pick up, higher fertilization rates and successful embryo transfers with optimal pregnancy rates is expected.
References
- Kelling G (1898) Endoskopie für Magen und Speiseröhre: 2. Gegliedertes, winklig streckbares Gastroskop mit rotierbarem Sehprisma. Münchener Med Wochenschrift 45: 1556.
- Schollmeyer T (2007) Georg Kelling (1866-1945): the root of modern day minimal invasive surgery. A forgotten legend? Arch Gynecol Obstet 276: 505-509.
- Mettler L (2017) The evolution of gynecologic endoscopic surgery over 50 years - a pleasant adventure. Medical Research Archives 5.
- Semm K (1983) Endoscopic appendectomy. Endoscopy 1983: 59-64.
- Goetz F, A Pier, C Bacher (1990) Modified laparoscopic appendectomy in surgery. A report on 388 operations. Surg Endosc 4: 6-9.
- Alkatout I, Mettler L (2019) Practical Manual for Laparoscopic & Hysteroscopic Gynecological Surgery. 3rd Edition, Jaypee Brothers Medical Publishers, New Delhi, India 2019.
- Nezhat C, Page B (2011) The advent of advanced operative videolaparoscopy. In: Nezhat’s history of endoscopy. Tuttlingen: Endo Press 2011: 159-179.
- Lindemann HJ (1979) CO2-hysteroscopy today. Endoscopy 11: 94100.
- Semm K (1976) Pelviskopie und Hysteroskopie.Farbatlas und Lehrbuch1976, Stuttgart, New York: Schattauer Verlag 1976.
- Hamou J (1981) Microhysteroscopy: a new procedure and its original applications in gynecology. J Reprod Med 1981.
- Hippocrates (2009) Whiteley, Kathleen Diseases of Women Book 1 - Greek Text with English Translation and Footnotes 2009.
- De Graaf (1672) De Mullerium Organis 1672.
- Martin Naboth (1707) De Sterilitate 1707.
- Morgagni 1769.
- Kyusaku Ogino (1882-1975) and Herman Knaus (1892-1975) and the Oginus-Knaus method
- John Smulders, in the 1930s, the rhythm method
- 1950: Gregory Pincus The Hormones (5 editions 1948 -1964)
- Kelley Kristin (2010) The Aschheim-Zondek Test for Pregnancy”. Embryo Project Encyclopedia.
- Cole HH, Hart GH (1930) The potency of blood serum of mares in progressive stages of pregnancy in effecting sexual maturity of the immature rat. Am J Physiol 83: 57-68.
- Edwards RG, Fowler RE (1959) Fetal mortality in adult mice after superovulation with gonadotropins. J Exp Zool 141: 299-322
- Gemzell CA, Diczfalusy E, Tillinger G (1958) Clinical effect of human pituitary follicle-stimulating hormone (FSH) J Clin Endocrinol Metab 18: 1333-1348.
- Donini P, Puzzuoli D, Alessio DI (1964) Purification of gonadotrophin from menopausal urine by gel filtration on sephadex. Acta Endocrinol (Copenh) 1964 45: 329-334.
- Shally, Arimura and Kastin H. Matsuo Y. Baba T.W. Redding r.M.G Nair and L. Debeljuk (1971) “Gonadotropin-Releasing Hormone: One polypeptide Regulates Secretion of Luteinizing and Follicle-Stimulating Hormones.” Science 173: 1036 -1038.
- Watson JD, Crick FH (1953) Molecular structure of nucleic acids; a structure for deoxyribose nucleic acid. Nature 171: 737-738.
- Devroey P, Van Steirteghem A, Mannaerts B, Coelingh Bennink H (1992) First singleton term birth after ovarian superovulation with rhFSH. Lancet 340: 1108-1109.
- Germond M, Dessole S, Senn A, Loumaye E, Howles C, et al. (1992) Successful in-vitro fertilization and embryo transfer after treatment with recombinant human FSH. Lancet 339: 1170.
- Wikland et al. (1983) Collection of human oocytes by the use of sonography. Fertil Steril 39: 603-608.
- Rock J, Menkin MF (1944) In vitro fertilization and cleavage of human ovarian eggs. Science 100: 105-107.
- Steptoe PC, Edwards RG (1976) Reimplantation of a human embryo with subsequent tubal pregnancy. Lancet 1: 880-882.
- Steptoe PC, Edwards RG (1978) Birth after the reimplantation of a human embryo. Lancet 12.
- Graham MM (2012) Clinical Molecular Imaging with Radiotracers: Current Status. Med Princ Pract 21: 197-208.
- Cazzato RL, Garnon J, Shaygi B, Koch G, Tsoumakidou G, et al. (2018) PET/CT-guided interventions: Indications, advantages, disadvantages and the state of the art. Minim Invasive Ther Allied Technol 27: 27-32.
- Collamati F, Maccora D, Alfieri S, Bocci V, Cartoni A, et al. (2020) Radio guided surgery with β (-) radiation in pancreatic Neuroendocrine Tumors: a feasibility study. Sci Rep 10: 4015.
- Cyranoski D (2016) Mouse eggs made from skin cells in a dish. Nature 301.
- Boekelheide K, Blumberg B, Chapin RE (2012) Predicting later-life outcomes of early-life exposures. Environmental Health Perspectives 120: 1353-1361.
- Beall SA, Decherney A (2012) The History and Challenges Surrounding Ovarian Stimulation in the Treatment of Infertility, fertil steril 97: 795801.
- Bruno Lunenfeld (2004) Historical perspectives in gonadotrophin therapy. Human Reproduction Update 2004: 453-467.
- Wyns C, Bergh C, et al. (2016) ART in Europe, 2016: European IVFmonitoring consortium (EIM)‡ for the European Society of Human Reproduction and Embryology (ESHRE), results generated from European registries by ESHRE 2016.
- Agarwal M, Mettler L, Marikinti K (2024) Handbook on Ovulation Induction in ART. Knowledge Bridge India 2024.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.