Morphometry of The Sternum in Osteosynthetic Reconstruction
Sebastian Reindl1*, Paul Schuller2, Matthias Meller1, Michael Beyer1, Josua Decker3 , Stephan Raab1
1 Department of Cardiothoracic Surgery, University Hospital Augsburg, Augsburg, Germany
2 Department of Thoracic Surgery, Klinikum Lippe, Lemgo, Germany
3 Department of Diagnostic and Interventional Radiology, University Hospital Augsburg, Augsburg, Germany
*Corresponding author: Sebastian Reindl, Department for Cardiothoracic Surgery, University Hospital Augsburg, Germany
Received Date: 04 August, 2022
Accepted Date: 16 August, 2022
Published Date: 22 August, 2022
Citation: Reindl S, Schuller P, Meller M, Beyer M, Decker J, et al. (2022) Morphometry of The Sternum in Osteosynthetic Reconstruction. J Orthop Res Ther 7: 1242 DOI: https://doi.org/10.29011/2575-8241.001242
Abstract
Introduction: Osteosynthetic reconstruction of the sternum can be challenging in thoracic surgery. Osteometric data on the complex anatomy of the sternal bone is needed for the choice of appropriate reconstruction techniques. Sternum clips may be an alternative to current available osteosynthesis.
Materials & Methods: Width, intercostal distances, thickness and length of the sternum as well as the distance of the internal thoracic arteries were analyzed in 50 patients who had undergone chest CT. Gender-specific correlation analyses between height, weight and sternum measurements were performed. It was investigated whether sternum clips are the right size to be used on patients concerning osteometric parameters.
Results: 50 patients (m:f = 31:19) aged 64.3 (14.3) years were examined. Body dimensions were 171.4 (9.4) cm height and 76.7 (14.8) kg weight. Osteometric data of the sternum could be assessed as follows: length 53.4 (5.9) mm for manubrium, 98.8 (14.0) mm for corpus and 46.5 (10.7) mm for xiphoid process. The vertical distance between two adjacent intercostal spaces was 29.0 (7.4) mm. The distance to the internal thoracic artery was 14.6 (1.3) mm. A correlation between body dimensions and bone morphometry could be found for the length of the sternum. There are gender-specific differences in length, but not in width.
Conclusion: The suitability of sternum clips regarding their size and dimensions could be anatomically demonstrated for almost all sternum bones. However, this cannot be done in all cases on the manubrium and the costal arch. Osteosynthesis can be adapted to the sternal dimensions of the individual patient.
Introduction
Osteosynthesis of the sternum is challenging for the thoracic surgeon due to the complex morphology of the bone. Common indications for sternal reconstruction are fractures due to thoracic trauma, congenital sternal cleft and median sternotomy in the context of cardiothoracic surgery [1,2] Various methods for sternal reconstruction and closure after median sternotomy have been developed and are available in clinical use - with the most common being the application of wire cerclage and titanium plates [3]. Anatomically, the adult sternum is divided into three parts [4,5] the manubrium (“handle”) with the incisures for clavicula and the 1st rib, the corpus or gladiolus with the incisures of the 3rd to 6th rib and the processus xiphoideus (“swordlike”). The three parts are separated by cartilage zones: at the symphysis manubriosternalis (angulus sterni, "Angle of Louis") articulates the 2nd rib; at the symphysis xiphosternalis articulates the 7th rib involving both connected bone parts (see also Figure 1). The arterial supply of the sternum is mainly via the internal thoracic artery (clinically a. mammaria interna) which arises from the subclavian artery. It runs dorsally on both sides of the anterior chest wall, covered by the endothoracic fascia and the parietal pleura, at variable distances parallel to the lateral sternum edges caudally. Branches are released to the mediastinum, the thymus, bronchi and also to the sternum bone [6,7].
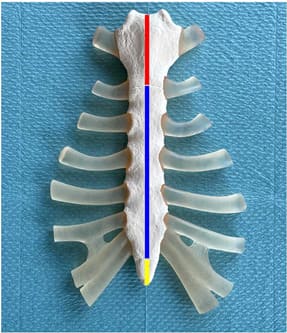
Figure 1: Adult sternum. Shown is the photography of a sternum model with the length of the manubrium outlined by a red, the corpus sterni by a blue, and the xiphoid process by a yellow bar.
In addition to gender and habitual differences, the sternum undergoes ontogenetic changes in osteometry throughout life, as Weaver et al. showed in a study of 330 CT scans published in 2014. For example, the length of the sternal body increases by age 30 whilst the manubrium predominantly shows an increase in width up to 1.6 to 1.8 times the width of the sternal body [8]. However, insufficient data on the exact morphometry of the sternum are available for the surgical decision on how to reconstruct the sternum by osteosynthesis, with mainly autoptic studies being performed for sex determination in anthropology and forensic medicine [9,10] There is also insufficient data in the literature available for the exact location of the internal thoracic artery. Especially for implantation of titanium plates or bone-spanning osteosynthetics the distance of the vessel to the sternum is of great importance. The question here is whether there is enough space to avoid injury to the artery when the osteosynthetics are implanted. In the field of rib osteosynthesis, rib clips (StraCos Trauma, MedXpert, Germany) have meanwhile been established [11] In the absence of data on the use of sternum clips for sternal reconstruction, this study investigates whether sternal clip dimensions are consistent with sternal parameters. Therefore, the aim of this study is to investigate whether sternal clips (StraCos Sternum, MedXpert, Germany) are suitable for osteosynthesis of the sternum and whether they can be safely used with regard to accompanying vessels – i. e. the bilateral internal thoracic artery.
Materials and Methods
To assess whether the sternal clips reflect the anatomical situation of the sternum, 50 randomly selected CT scans of the thorax between 12/2016 and 02/2017 were used to obtain osteometric data of the sternum, adjacent pairs of ribs, and intercostal spaces as well as the lateral distance to the internal thoracic artery on both sides. Sex, height and weight were determined for the selected patients. The underlying indication for the CT scan was not considered but thoracic trauma was excluded. All CT scans were performed on an 2nd generation dual-source CT system (SOMATOM Flash, Siemens Healthineers, Forchheim, Germany) with intravenous application of iodinated contrast material for visualizing the exact course of the arterial vessel. Multiplanar reconstructions in the transverse, coronal and sagittal planes were prepared from the datasets with a slice thickness of 1 mm. Measurements were conducted on a dedicated workstation (Deep Unity, Dedalus Healthcare Systems Group, Germany). Using sagittal reconstructions, first the maximum length of the manubrium, the sternal body and the xiphoid process were measured in the median line. The widths of the manubrium and sternal body – at the level of the 1st to 5th intercostal spaces (ICS) – were then determined in the coronal reconstruction and the vertical parasternal distances between two ICS were measured. The latter measurements were taken between the 1st and 2nd ICS, the 2nd and 3rd ICS, the 3rd and 4th ICS and the 4th and 5th ICS. Lastly, in transverse slice planes at the level of ICS 1 to 5, the thickness of the sternum and the horizontal distance between the lateral sternum margins and the parasternal course of the internal thoracic artery on both sides were determined at the levels of ICS 1, 2 and 4. Individual measurements are shown as examples in Figure 2.
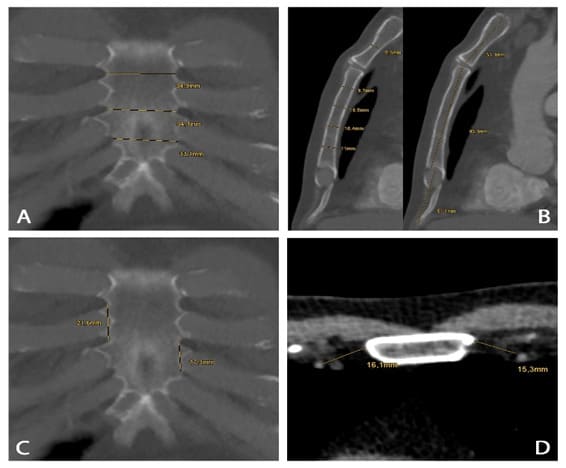
Figure 2: Exemplary measurements of sternal parameters in CT scans. (A) to (D) show exemplary measurements of sternal parameters using multiplanar reconstructions of randomly selected CT scans: width (A) at the level of 3rd to 5th intercostal space; thickness (B, left) at the level of 1st to 5th intercostal space; length (B, right) of manubrium, corpus and xiphoid process in the median line; vertical parasternal distances (C) between 3rd / 4th and 4th / 5th ICS; parasternal distance of the internal thoracic artery on both sides at the levels of ICS 4.
Data were statistically analyzed using R version 4.0.2 (R Core Team, Vienna, Austria) and are presented as mean (standard deviation) including the specific ranges. Because of the rather small sample sizes, exact tests were performed. Dependency of all osteometric parameters to body height and weight was calculated with Pearson’s correlation coefficient, the [95% Confidence Intervals] (CI) are specified. The p-values presented are not adjusted for multiple testing and therefore cannot be compared directly with prespecified significance level of, e. g. 5%. The number of tests performed in this analysis (8 tests) in combination with the sample size needs to be considered when interpretating the results of the tests. Therefore, these should be used purely as support when looking at the correlation between the variables. Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article. The study was approved by ethics committee.
Results
Osteometric Data of The Sternum
A total of 50 patients (m:f = 31:19) with a mean age of 64.3 (14.3) years (range: 25.6-86.1 years ) were examined. Mean height was determined to be 171.4 (9.4) cm (range: 164-192 cm) with a mean weight of 76.7 (14.8) kg (range: 50.0-118.0 kg). Mean length calculated was 53.4 (5.9) mm (range: 40.0-62.9 mm) for the manubrium, 98.8 (14.0) mm (range: 65.7-124.0 mm) for the sternal body and 46.5 (10.7) mm (range: 19.2-68.7 mm) for the xiphoid process. Results are shown in Table 1. Table 2 shows the mean width of the sternum corresponding to the smallest horizontal distance between two opposite intercostal spaces, as well as the mean thickness of the sternum at the level of intercostal spaces 1 to 5. The mean vertical distance between two adjacent intercostal spaces directly parasternal was 29.0 (7.4) mm (range: 10.0-47.9 mm). Details are depicted in Table 3. The horizontal distance between the internal thoracic artery and the lateral border of the sternum on both sides was 14.6 (1.3) mm (range: 4.7–33.3 mm), as shown in Table 4. A correlation could be found for the patients’ height and the length of the sternum: there was a weak correlation for the manubrium (R=0.343, [0.072; 0.567], p=0.0146), a strong correlation for the corpus sterni (R=0.655, [0.461; 0.790], p<0,0001) and a medium correlation for the xiphoid process (R=0.463, [0.212;0.657], p=0.007) (see Figure 3). No correlation could be found between the patients’ weight and the sternum width.
|
|
Sternum length [mm] |
|
|
|
|
Manubrium |
Corpus sterni |
Xiphoid |
|
|
(N=50) |
(N=50) |
(N=50) |
|
Mean (SD) |
53.37 (5.89) |
98.78 (14.03) |
46.51 (10.7) |
|
Min - Max |
40 - 62.9 |
65.7 - 124 |
19.2 - 68.7 |
Table 1 : Sternum length.
|
|
ICS 1 |
ICS 2 |
ICS 3 |
ICS 4 |
ICS 5 |
|
|
(N=50) |
(N=50) |
(N=50) |
(N=50) |
(N=50) |
|
Sternum width [mm] |
|
|
|
|
|
|
Mean (SD) |
35.48 (6.22) |
28.71 (4.42) |
30.3 (4.99) |
33.85 (6.97) |
32.28 (7.68) |
|
Min - Max |
24.6 - 56 |
20.5 - 39.2 |
20 - 44.4 |
21.2 - 56.9 |
17.5 - 57.7 |
|
Sternum thickness [mm] |
|
|
|
|
|
|
Mean (SD) |
16.05 (3.48) |
12.26 (2.21) |
10.52 (1.81) |
9.68 (1.89) |
9.65 (2.21) |
|
Min - Max |
8 - 23.9 |
9 - 17.7 |
7.5 - 15.2 |
6.1 - 14.7 |
4.1 - 15 |
ICS = intercostal space
Table 2: Sternum width and thickness.
|
|
Vertical
distance between two adjacent ICS [mm] |
|
|
|
|
|
ICS
1 and 2 |
ICS
2 and 3 |
ICS
3 and 4 |
ICS
4 and 5 |
|
|
(N=50) |
(N=50) |
(N=50) |
(N=50) |
|
Mean
(SD) |
27.64
(6.7) |
30.11
(7.51) |
31.37
(8.34) |
27.07
(6.47) |
|
Min
- Max |
10.0
- 47.9 |
13.0
- 47.3 |
11.0
- 46.5 |
11.5
- 38.2 |
ICS = intercostal space
Table 3: Vertical distance between two adjacent ICS .
|
|
Distance between internal thoracic artery / sternum edge [mm] |
|||||
|
|
ICS 1 right |
ICS 1 left |
ICS 2 right |
ICS 2 left |
ICS 4 right |
ICS 4 left |
|
|
(N=50) |
(N=50) |
(N=50) |
(N=50) |
(N=50) |
(N=50) |
|
Mean (SD) |
13.0 (4.9) |
12.6 (4.7) |
15.6 (3.5) |
14.9 (3.4) |
15.3 (3.4) |
16.03 (3.9) |
|
Min - Max |
4.7 – 32.0 |
5.0 - 33.3 |
8.6 – 24.7 |
8.3 – 24.7 |
6.8 - 27.4 |
8 - 25.4 |
ICS = intercostal space
Table 4: Distance between internal thoracic artery and sternum edge.
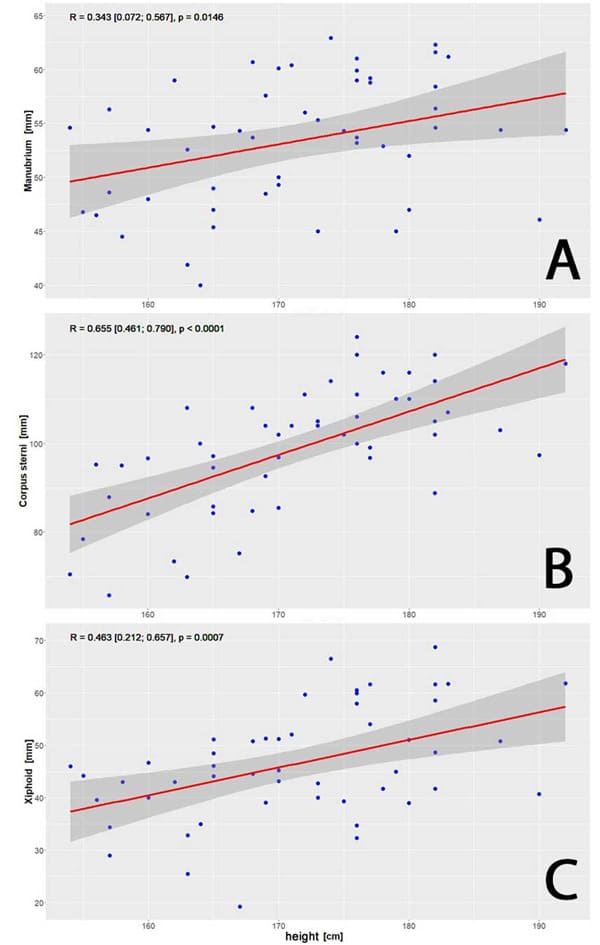
Figure 3: Correlation between patients’ height and sternum length. Correlation for the manubrium (R=0.343, [0.072; 0.567], p=0.0146), A), correlation for the corpus sterni (R=0.655, [0.461; 0.790], p<0,0001, B) and correlation for the xiphoid process (R=0.463, [0.212;0.657], p=0.007, C).
Gender-Specific Differences
Gender-specific differences could be shown for the length of all three bony parts of the sternum. For the manubrium: male vs. female = 55.41 (5.31) mm vs. 50.04 (5.35) mm; the corpus sterni: 106.37 (8,72) mm vs. 86.39 (12.17) mm; and the xiphoid process: 50.3 (10.08) vs. 40.33 (8.77) mm. Hotelling’s T2-Test showed overall differences of sternum width and length between men and women (p < 0.0001). Detailed data is given in Table 5 and Figures 4 and 5.
|
|
Sternum length [mm] |
|||
|
|
Manubrium |
Corpus sterni |
Xiphoid |
|
|
Male |
|
|
|
|
|
n |
31 |
31 |
31 |
|
|
Mean (SD) |
55.41 (5.31) |
106.37 (8.72) |
50.3 (10.08) |
|
|
Min - Max |
45 - 62.9 |
88.8 - 124 |
32.3 - 68.7 |
|
|
Female |
|
|
|
|
|
n |
19 |
19 |
19 |
|
|
Mean (SD) |
50.04 (5.35) |
86.39 (12.17) |
40.33 (8.77) |
|
|
Min - Max |
40 - 59 |
65.7 - 108 |
19.2 - 51.3 |
|
Table 5: Gender-specific differences in the length of sternum bone.
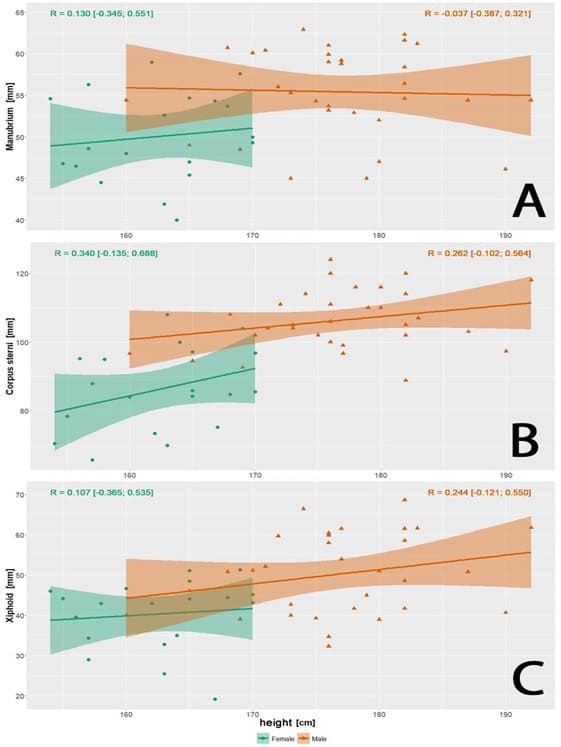
Figure 4: Gender-specific correlations between patients’ height and sternum length. Gender-specific correlations between patients’ height and sternum dimensions. (A) manubrium: female R=0.130 [-0.345;0.551], male R=-0.037 [-0.387;0.321] (B) corpus sterni: female R=0.340 [-0.135;0.688], male R=0.262 [-0.102;0.564] (C) xiphoid: female R=0.107 [-0.365;0.535], male R=0.244 [-0.121;0.550].
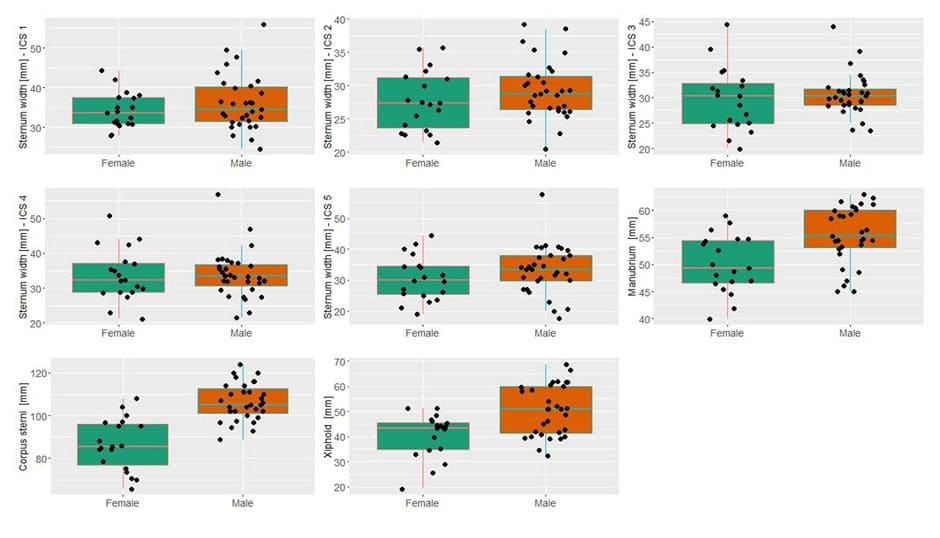
Figure 5: Gender-specific differences in sternum dimensions. Gender-specific boxplots are shown for sternum width at intercostal spaces 1 to 5 (upper row, middle row left and middle) and sternum length for manubrium (middle row right), corpus sterni (lower row left) and xiphoid (lower row middle). Gender-specific differences can be seen for the length of the manubrium: male vs. female = 55.41 (5.31) mm vs. 50.04 (5.35) mm; the corpus sterni: 106.37 (8,72) mm vs. 86.39 (12.17) mm; the xiphoid process: 50.3 (10.08) vs. 40.33 (8.77) mm. Hotelling’s T2-Test showed overall differences of sternum length between men and women (p < 0.0001)
Discussion
Clinical application of sternum clips
Color-coded sternum clips are available in various widths and heights, each of which cover different sternal dimensions:
- Size S: width 26 mm, height 15.5 mm; yellow
- Size M: width 33 mm, height 15.5 mm; pink
- Size L: width 40 mm, height 15.5 mm; blue
The recorded measurements indicate that, in terms of the width of the sternal body, one of the three clip sizes is suitable for implantation in most cases. It can be assumed from this that the yellow size S is suitable for a corpus width < 26 mm, the pink size M is suitable for a width of 26 mm to 33 mm and the blue size L is suitable for 33 mm to 40 mm. The indicated sizes cover 88% of the total of 250 measurements recorded for the sternal width (size S 15%, size M 45%, size L 28%); for 23 measurements another as yet unavailable size XL for a width of 40 to 47 mm is required.
A total of six measurements (2%) would require a clip width > 47 mm and are thus not suitable for the sternum clips. Three of the extra-large measurements were recorded for a patient with normal weight (173 cm, 80 kg) with an unusually wide sternum. A strong correlation with patient height could be identified particularly for the length of the sternal body (Pearson’s correlation R=0.655, [0.461; 0.790], see Figure 3); the length of the manubrium and the xiphoid process also showed a weaker correlation. Regarding the patients´ weight, there was no correlation with the morphometry of the sternum. The distance between two intercostal spaces was determined over all the measured ICS distances, 27.0 (7.4) mm (10 mm min. between 1st and 2nd ICS, 47.9 mm max. between 1st and 2nd ICS). The distances between the intercostal spaces can always be adjusted appropriately over the entire measurement range by stretching or compressing the sternal clips. Regarding the measured distances, there was also no correlation with the height or weight of the patients in the current dataset.
The internal thoracic artery is sufficiently far away in the corpus area that the sternum clips can be implanted without injuring the vessel. On average, the internal thoracic artery is 12.6 (4.7) mm and 16.3 (3.9) mm from the sternum. The minimum measured distance was 4.7 mm. This means that with preparation strictly lateral to the sternum, there is no risk of injuring the internal thoracic artery. There was no significant difference between the sides. It can thus be assumed that in most cases an appropriate sternum clip with two or three segments can be found. An intraoperative example of such a sternal reconstruction along with radiologic control is shown in Figure 6.
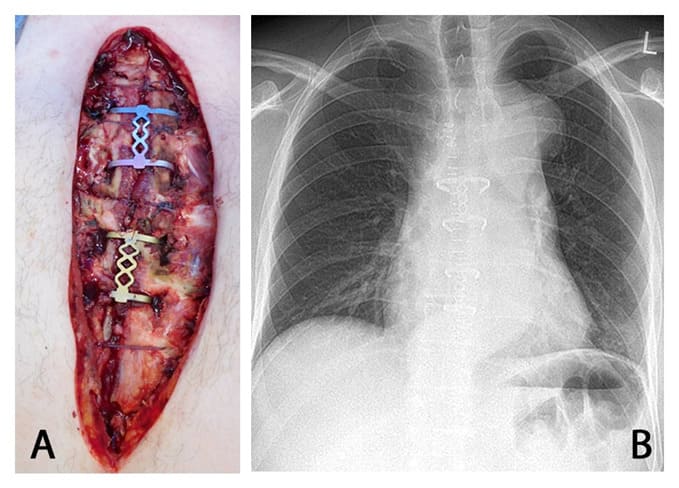
Figure 6: Intraoperative situs after sternum stabilization and postoperative chest x-ray.
(A) shows the intraoperative situs after sternum stabilization using two sternum clips (Medium-Large in 2nd and 3rd ICS, Small-Small in 4th and 5th ICS) and three PDS sutures. (B): postoperative control via chest x-ray, the sternum clips are properly placed.
Conclusion
With few exceptions, the available sternum clips can be used for osteosynthesis of the sternum. Particularly on the sternal body, an appropriate combination can practically always be found due to the clip sizes Small, Medium and Large that are available as well as the ability to vary the length of the clips. Regarding sternal thickness, there was no contraindication to the use of the sternum clips in terms of osteometry. When prepared strictly parasternally and used according to the manufacturer´s instructions, there is no risk of injuring the internal thoracic artery, which runs parallel to the edges of the sternum.
References
- Chandrakanth HV, Kanchan T, Krishan K (2014) Osteometric analysis for sexing of modern sternum – An autopsy study from South India. Legal Medicine 16: 350-356.
- Graeber GM, Nazim M (2007) The anatomy of the ribs and the sternum and their relationship to chest wall structure and function. Thoracic surgery clinics 17: 473-489.
- Gupta M, Sodhi L, Sahni D (2002) Variations in collateral contributions to the blood supply to the sternum. Surgical and radiologic anatomy : SRA 24: 265-270.
- Jesus RA de, Acland RD (1995) Anatomic study of the collateral blood supply of the sternum. The Annals of Thoracic Surgery 59: 163-168.
- Losanoff J (2002) Primary closure of median sternotomy: techniques and principles. Cardiovascular Surgery 10: 102-110.
- Naidu B v, Rajesh PB (2010) Relevant surgical anatomy of the chest wall. Thoracic surgery clinics 20: 453-63.
- Raab S, Grieser T, Sturm M, Beyer M, Reindl S (2019) Management der Rippenfraktur. Zentralblatt für Chirurgie - Zeitschrift für Allgemeine, Viszeral-, Thorax- und Gefäßchirurgie 144: 305-321.
- Robicsek F, Fokin A, Cook J, Bhatia D (2000) Sternal instability after midline sternotomy. Thoracic and Cardiovascular Surgeon 48: 1-8.
- Schimmer C, Reents W, Elert O (2006) Primary closure of median sternotomy: A survey of all German surgical heart centers and a review of the literature concerning sternal closure technique. Thoracic and Cardiovascular Surgeon 54: 408-413.
- Selthofer R, Nikoli} V, Mr~ela T, Radi} R, Lek{an I, Rudè I, Selthofer K (2006) Morphometric Analysis of the Sternum. Collegium antropologicum 30: 43-47.
- Weaver AA, Schoell SL, Nguyen CM, Lynch SK, Stitzel JD (2014) Morphometric analysis of variation in the sternum with sex and age. Journal of Morphology 275: 1284-1299.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.