Milestones of Laparoscopic Common Bile Duct Exploration in Gadarif, Eastern Sudan
by Sami Eldirdiri Elgaili Salah1, Mohamed Seif Eldawla Saeed Ahmed2, Samual Eldirdiri Elgaili Salah1
1University of Gadarif, Faculty of Medicine, Hospital Street, Gadarif, Sudan
2Al-Neelain University, El gamhuriya avenue, Khartoum, Sudan
*Corresponding Author: Sami Eldirdiri Elgaili Salah, University of Gadarif, Faculty of Medicine, Hospital Street, Gadarif, Sudan
Received Date: 13 March 2026
Accepted Date: 01 April 2026
Published Date: 03 April 2026
Citation: Salah SEE, Ahmed MSES, Salah SEE (2026) Milestones of Laparoscopic Common Bile Duct Exploration in Gadarif, Eastern Sudan. J Surg 11: 11596 DOI: https://doi.org/10.29011/2575-9760.011596
Abstract
Background: Common bile duct stones (CBDS) are found in 6% to 12% of patients with gallbladder stones. LCBDE is as effective as ERCP in clearing the CBDS with a shorter time in the OR and hospital stay and removing the GB as well. However, patient’s condition, operator’s expertise and local resources should be taken into account in making treatment decisions.
Material and Method: This is hospital based cross sectional study. In Gadarif, eastern Sudan, a city with no ERCP service while laparoscopy is available. Forty-eight patients underwent laparoscopic common bile duct exploration in GTH Eastern Sudan in the period from 2020 - 2024.
Result: Out of 48 patients complete stone clearance was achieved in 45 (clearance rate 93.6%). Male to female ratio was equal, the operative time range from 73 to 200 minutes. Postoperatively, CBD drainage was mainly through T-Tube (79.2%). Out of 43 patients; 2 patients admitted for More than 5 days, one for COVID-19 and the other for non-surgical reason. In the remaining patients, the mean hospital stay was 38 hours. Minor complications were reported in 5 patients (10.4 %) and conversion to open in another 5 patients
Conclusion: Even in limited resources setup, LCBDE is the logical management for CBD stones, especially where there are no ERCP services, as it is proven to be comparably feasible, safe and cost effective for patients who were served by general surgeons.
Keyword: Gadarif; Laparoscopic Common Bile Duct Exploration; LCBDE; Sudan
Introduction
Gallstone Disease (GSD) is one of the most common problems affecting the digestive tract. Autopsy reports have shown a prevalence of gallstones from 11% to 36%. The prevalence of gallstones is related to many factors, including age, gender, and ethnic background. Women are three times more likely to develop gallstones than men, and first-degree relatives of patients with gallstones have a twofold greater prevalence [1]. Common Bile Duct Stones (CBDS) are found in 6% to 12% of patients with stones in the gallbladder. The incidence increases with age. About 20% to 25% of patients above the age of 60 with symptomatic gallstones have stones in the common bile duct as well as in the gallbladder. They may be formed within the gallbladder and migrate down the cystic duct to the common bile duct. These are classified as secondary common bile duct stones, in contrast to the primary stones that form in the bile ducts [1]. They can result in several health problems, including pain, jaundice, infection and acute pancreatitis. A variety of imaging modalities can be employed to identify the condition, while management of confirmed cases of CBDSs may involve Endoscopic Retrograde Cholangiopancreatography (ERCP), surgery and radiological methods of stone extraction. Clinicians are therefore confronted with a few potentially valid options to diagnose and treat individuals with suspected CBDS [2]. Choledocholithiasis can be treated by either open, laparoscopic, percutaneous, or endoscopic means either in One Stages: Cholecystectomy + CBD exploration or Rendez-vous Technique or in Two Stages: ERCP followed by cholecystectomy or Cholecystectomy followed by ERCP. The current treatment for CBDS alone is endoscopic sphincterotomy and stone extraction. In patients requiring cholecystectomy for symptomatic gallstone disease, endoscopic stone extraction is performed before the operation. However, single-stage treatment with ductal stone clearance at the time of laparoscopic cholecystectomy which is known as Laparoscopic Common Bile Duct Exploration (LCBDE) is proven by early randomized trials in the late 1990s to be as effective as ERCP in clearing the common bile duct of stones and there is a non-significant trend to shorter time in the operating theatre, and a significantly shorter hospital stay in patients treated by LCBDE. [3] Due to limited resources in our country and non-availability of ERCP service in our state, now we consider LCBDE + LC as a logical surgical approach for CBD stone in Gadarif Teaching Hospital (GTH) as it show the same result of pre/post operative ERCP and LC in single session, by one team, equivalent success rates and patient morbidity, Moreover in fit patients (ASA I & II) single-stage laparoscopic treatment is the better option [4].
Objectives
Our study aims to assess the outcome of laparoscopic common bile duct exploration in a limited remote provincial hospital in the constrained health system of Sudan, where there is no facility for ERCP available in our state. Measuring the length of hospital stay, operative time, rate of complications (retained CBD stone, failure, bile leak) and rate of conversion.
Methods
This was hospital based descriptive cross-sectional study conducted at Gadarif Teaching Hospital, Eastern Sudan (420 km from Khartoum, the capital of Sudan). The study includes all patients undergoing LCBDE for CBD stone in period between June 2020 and December 2024. Sampling was done with total coverage due to limited patient number (48 patients).
Results
Patient Characteristics: A total of 48 patients with the age range from 20 to 82 years (mean age 54.5 years); with equal gender distribution underwent LCBDE. Most of the patients 38, presented with jaundice and pruritus (80%), followed by right hypochondrial pain in 24 patients (50%), while only few patients presented with dyspepsia or nausea and vomiting (Figure 1). Duration of symptoms exceeded 1 year in 17 patients, (34.5%). Four patients (8.3%) had prior ERCP, and two patients (4.2%) had previous history of cholecystectomy i.e primary CBD stone (Table 1).
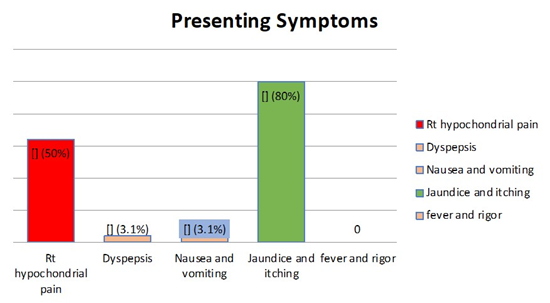
Figure 1: Presenting Symptoms of Patients Underwent LCBDE at GTH 2020-2024
|
Frequency |
Percent |
|
|
Duration of symptoms Less than 1 year |
13 |
27.6 |
|
1-3 years |
17 |
34.5 |
|
3-5 years |
6 |
13.8 |
|
More than 5 years |
12 |
24.1 |
|
History of ERCP |
4 |
8.3 |
|
History of cholecystectomy |
2 |
4.2 |
|
LFT Normal |
8 |
16.7 |
|
Abnormal |
40 |
83.3 |
Table 1: Clinical and Labarotary Findings of Patients Underwent LCBDE at GTH 2020-2024.
Imaging: Ultrasound showed CBD dilatation in 97% and single CBD stone in 90%. Stones were 7–15 mm in 62.5%, with 13% exceeding 15 mm.
Operative Outcomes: Operative time ranges between 73 and 200 minutes (median 113). Stone clearance was achieved in 45 patients (93.6%). Bile duct drainage was through T-tube in 37 patients 77%, trans-cystic drain in 4 patients (8%), while in 4% no drain was left behind in those who were already had a pre-operative ERCP, sphincterotomy and stented.
Postoperative Outcomes: Complications were encountered in 8 patients (16%) of the patients with overall conversion to open in 5 patients (10.4%), biliary stricture 2, and retained stone, bleeding and bile leak was encountered in 1 patient for each. All these 5 patients were sent for ERCP after optimizing their general condition. The mean hospital stay was 38 ± 19 hours with 2 patients stayed for more than 5 days (COVID-19, non-surgical illness). No intraoperative mortality was encountered in this series. (Table 2) Many factors and variables were studied to identify if any is affecting complications, however no significant correlation was found (Table 3)
|
Frequency |
Percent |
|
|
Clearance by Choledochoscopy |
45 |
93.75 |
|
Operative Complications |
5 |
10.41 |
|
CBD drainage No drainage (1ry closures) |
1 |
2.1 |
|
T-tube |
38 |
79.2 |
|
Trans-cystic drain |
4 |
8.3 |
|
Converted to Open |
5 |
10.4 |
|
Hospital Stay: More than 5 days |
2 |
6.3 |
|
Reason for stay Surgical |
0 |
0 |
|
Non-surgical |
1 |
50 |
|
COVID-19 |
1 |
50 |
Table 2: Outcome of patients underwent LCBDE at GTH 20202024.
|
Factor |
Odds ration |
p-value |
|
Age |
0.9 |
0.4 |
|
Gender |
. |
0.99 |
|
Duration of symptoms |
0.2 |
0.1 |
|
History of ERCP |
. |
0.9 |
|
History of Cholecystectomy |
0.9 |
|
|
Abnormal LFTs |
1.6 |
0.6 |
|
Number of stones in the gall bladder |
1.9 |
0.4 |
|
CBD caliber |
. |
1 |
|
Size of stone in the CBD |
0.6 |
0.6 |
|
Number of stones CBD |
3 |
0.4 |
|
Impacted stone |
1.9 |
0.6 |
|
Operation time |
1 |
0.9 |
Table 3: Factors Affecting Complications and Conversion, binary logistic regression.
Discussion
Treatment of CBD stones has variable methods, ranging from open surgery OCBDE, laparoscopic exploration LCBDE and endoscopic based ERCP. Each procedure has different efficacy, safety and feasibility. Till now the literatures are arguing about which is the best for different situations. The cornerstone of this argue is comparing a single stage versus two stages procedure. A Cochrane database review by Martin et al in 2006 evaluating ERCP vs Open, pre-op ERCP vs LCBDE, and post-op ERCP vs LCBDE, includes 13 trials that randomized 1351 patients and concluded that: In the era of open surgery CBDE was superior to ERCP, and in the era of laparoscopy: there was no difference between laparoscopic and ERCP clearance of CBD stone(s) while ERCP increases the number of surgical procedures in patients with CBD stone(s) [5]. Another prospective randomized trial in 2010 showed that both ERCP+LC and LC+LCBDE were highly effective in detecting and removing common bile duct stones and were equivalent in overall cost and patient acceptance. However, the overall duration of hospitalization was shorter and physician fees lower for LC+LCBDE [6]. Evidence from 4 Databases: PubMed, Embase, Cochrane Central Register of CTs and the Science Citation Index in 2012 has shown that Single-stage management is equivalent to two-stage management and requires fewer procedures. However, patient’s condition, operator’s expertise and local resources should be considered in making treatment decisions. [7]. When it comes to 2018 systematic review and Meta-analysis of RCTs concluded that: Single-stage LCBDE is superior to ERCP + LC in terms of technical success and shorter hospital stay in good-risk patients with gallstones and CBD stones, where expertise, operative time and instruments are available [8]. Our Study focus on assessing laparoscopic common bile duct exploration efficacy in terms of clearance rate of stones, operation time and rate of complications in limited resources setup. A recent study with a similar sample concluded that both LCBDE and ERCP are safe and effective for choledocholithiasis. ERCP offers faster recovery and is better suited for smaller, uncomplicated stones. LCBDE provides a more definitive solution for complex cases with larger stones, leading to shorter hospital stays. Treatment choice should be tailored based on stone characteristics, patient condition, and available expertise. [9] Our results showed that LCBDE in GTH has a clearance rate of 93.58% which is considered a very good rate giving that it’s done in limited setup.
As there are no facilities for ERCP or Magnetic Resonance Imaging (MRI) in the whole state. This finding is constant with Long Pal et al study who reported clearance rate of LCBDE VS pre-operative ERCP+ LC was (94.1% vs 90.1%) [10]. This indicate that clearance rate of our study despite the limited setup is like that of well-developed center and is higher than that of ERCP clearance rate reported in the literatures as the use of ERCP necessitates increased number of procedures per patient to clear the stones. However, the reported clearance of open surgery is higher than that of laparoscopic surgery in general not only in our study, but due to its high degree of morbidity and mortality, it becomes less common. [5]. Most of our patients stayed limited time in hospital, 0 - 3 days with average of 38 hours. It’s similar to B Topal et al study that was done in Belgium which compared the hospital staying time between laparoscopic exploration alone and Laparoscopic+ ERCP and it was significantly higher in the double stage procedure and increased cost for the later too. From the economical point of view CBDE patients should preferably be treated via a one-stage procedure as long as safety and efficacy of this approach are provide [11]. Hospital stay in our study was even less than that reported in some studies from similar settings [12,13]. This can be due to the limited admission feasibility among low-income Sudanese patients and limited setting in our hospital. However, this didn’t affect the outcome of our patients, as the complication rate reported was 10.4 %, in form of biliary stricture, leaks and bleeding, this may be attributed to the fact that CBD drainage was mainly through T-Tube (79.9%) in our series, which has many reported complications such as bile leakage, peritonitis, T-tube dislocation or obstruction and sepsis. In addition, the fact that the patient stays with the drainage catheter for a long time was historically known to reduces patient comfort, increases the risk of complications and costs [14,15]. Recently, primary closure method with lower complications and higher success rates have been used. However, this technique requires advanced laparoscopic experience or preoperative sphincterotomy [16], we did it in only one case who had a previous sphincterotomy. The complication rate in this study is similar to the study done in Sohag University Hospital in Egypt as they reported the morbidity rate was 15% in the form of wound infection, bile leak, missed stone and ileus [13]. This similarly can be explained by the fact that both studies had been done nearly similar setting. Although, these results differ from a study published in Italy, which reported a complication rate of LCBDE VS PRE-OPERATIVE ERCP as (7.6% vs 12.0) with majority of complications is bile leaks [10]. This can be explained by the fact that it’s done in a more experienced center and hence better setup. Moreover, the complication rate in open CBDE in Mena et al was higher (laparoscopic 5% vs. open 15%). Wound infection and ileus were the main complications in the open group. Rafailidis et al, Grubnik et al and Halawani et al, also showed the higher complication rate of the open approach vs. LCBDE [1719]. Although OCBDE is a safe and effective approach for the treatment of CBDS, nowadays with advancement in the equipment and laparoscopic skills, LCBDE can be performed with high efficiency, safety, low morbidity and mortality [17,19]. However, open surgery is still the standard for removal of the bile duct stones. If the surgical team has a lack of the laparoscopic experience, or highly expert endoscopists are not available, open surgery should be employed. The operation time range from a minimum of 40 minutes to a maximum of 200 minutes, this variability can be due to variability of patient condition, different clearance measures and the experience of the laparoscopic surgeon who did the operation. However, the range is still concomitant with that reported in literature with long experience or nearby settings [20,13]. On the other hand, the open surgery takes less time but with the cost of increasing hospital stay and ERCP takes even longer time [20]. Unfortunately, no significant correlation was established in our study between different variables and operation time and complication, this can be explained by the low sample size we used. Which can be considered as one of the limitations for our study.
Conclusion
Traditionally, compared to ERCP, open CBDE has been proven to be superior in the pre-laparoscopy era. Surgeons should be encouraged and trained to do LCBDE especially where there are no ERCP services, as it is proven to be comparably feasible, safe and cost effective for patients who were served by general surgeons. No matter when ERCP, pre or post, the completion of 1 disease entity, needs 2 different specialized teams has been proved to be costly.
References
- Pham TH, Hunter JG (eds.) (2015) Gallbladder and the Extrahepatic Biliary System in Schwartz, Principals of Surgery 10th edition 2015 USA, McGraw-Hill Education 2015: 1309-1340.
- Williams E, Beckingham I, Sayed G El, Gurusamy K, Sturgess R, et al (2017) Updated guideline on the management of common bile duct stones ( CBDS ) 66: 765-782.
- M Rhodes, L Sussman, L Cohen, MP Lewis (1998) Randomised trial of laparoscopic exploration of common bile duct versus postoperative endoscopic retrograde cholangiography for common bile duct stones. The Lancet 351: 159-161.
- Cuschieri A, Lezoche E, Morino M, Croce E, Lacy A, Toouli J, Faggioni A, Ribeiro VM, Jakimowicz J, Visa J, Hanna GB (1999) E.A.E.S. multicenter prospective randomized trial comparing two-stage vs single-stage management of patients with gallstone disease and ductal calculi. Surg Endosc 13: 952-957.
- Martin DJ, Vernon DR, Toouli J (2006) Surgical versus endoscopic treatment of bile duct stones. Cochrane Database Syst Rev 19: CD003327.
- Rogers SJ, Cello JP, Horn JK, Siperstein AE, Schecter WP, Campbell AR, Mackersie RC, Rodas A, Kreuwel HT, Harris HW (2010) Prospective randomized trial of LC+LCBDE vs ERCP/S+LC for common bile duct stone disease. Arch Surg 145: 28-33.
- Lu J, Cheng Y, Xiong XZ, Lin YX, Wu SJ, Cheng NS (2012) Two-stage vs single-stage management for concomitant gallstones and common bile duct stones. World J Gastroenterol 18: 3156-3166.
- Singh AN, Kilambi R (2018) Single-stage laparoscopic common bile duct exploration and cholecystectomy versus two-stage endoscopic stone extraction followed by laparoscopic cholecystectomy for patients with gallbladder stones with common bile duct stones: systematic review and meta-analysis of randomized trials with trial sequential analysis. Surg Endosc 32: 3763-3776.
- Anandaravi BN, Jose S (2026) Laparoscopic common bile duct exploration versus endoscopic retrograde cholangiopancreatography as the first line treatment for choledocholithiasis. Int Surg J 13: 339345.
- Pan L, Chen M, Ji L, Zheng L, Yan P, Fang J, Zhang B, Cai X (2018) The Safety and Efficacy of Laparoscopic Common Bile Duct Exploration Combined with Cholecystectomy for the Management of Cholecysto-choledocholithiasis: An Up-to-date Meta-analysis. Ann Surg 268: 247-253.
- Topal B, Vromman K, Aerts R, Verslype C, Van Steenbergen W, Penninckx F (2010) Hospital cost categories of one-stage versus twostage management of common bile duct stones. Surg Endosc 24: 413416.
- Yildirim M, Dasiran F, Ozsoy U, Daldal E, Kocabay A, Okan I (2021) The Efficiency of Laparoscopic Common Bile Duct Exploration in Endoscopic Retrograde-Cholangiopancreatography-Limited Setting in a Peripheral University Hospital. J Laparoendosc Adv Surg Tech A 31: 665-671.
- Helmy MZ, Ahmed AE (2018) Safety and efficacy of laparoscopic versus open surgery in management of common bile duct stones: experience at the Sohag University Hospital, Egypt. Int Surg J 5: 37273732.
- Wills VL, Gibson K, Karihaloot C, Jorgensen JO (2002) Complications of biliary T-tubes after choledochotomy. ANZ J Surg72: 177-180.
- Şahiner İT, Kendirci M (2017) Retrospective Clinical Study of the Effects of T-Tube Placement for Bile Duct Stricture. Med Sci Monit 23: 4328-4333.
- Jameel M, Darmas B, Baker AL (2008) Trend towards primary closure following laparoscopic exploration of the common bile duct. Ann R Coll Surg Engl 90: 29-35.
- Poulose BK, Holzman PA (2006) National analysis of in-hospital resources utilization in choledocholithiasis management using propensity scores. Surg Endosc 20: 186-190.
- Eidy M, Jesmi F, Raygan F, Pishgahroudsari M, Pazouki A (2015) Evaluating the effect of drain site on abdominal pain after laparoscopic gastric bypass surgery for morbid obesity: a randomized controlled trial. Bariatr Surg Pract Patient Care10: 38-41.
- Halawani HM, Tamim H, Khalifeh F, Mailhac A, Taher A, et al (2017) Outcomes of laparoscopic vs open common bile duct exploration: analysis of the NSQIP database. J Am Coll Surg 224: 833-840.
- Quaresima S, Balla A, Guerrieri M, Campagnacci R, Lezoche E, et al (2017) A 23 year experience with laparoscopic common bile duct exploration. HPB (Oxford) 19: 29-35.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.