Long-Term Outcomes of Combined Core Decompression, Bone Marrow Aspirate Transplantation, and Platelet-Rich Plasma for the treatment of Femoral Head Osteonecrosis in children
by Enrica Cristini1, Ivan Taietti2*, Cecilia Eboli3, Martina Rossano3, Fabiana Di Stasio3, Federica Vianello3, Antonio Mastrangelo4, Irene Borzani5, Stefania Villa6, Giovanni Filocamo3
1Department of Orthopaedics and Traumatology, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy
2Pediatric Immuno-rheumatology Unit, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano IT and University of Pavia, Pavia, Italy
3Pediatric Immuno-rheumatology Unit, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, and University of Milano, Milano, Italy
4Pediatric Nephrology, Dialysis and Transplant Unit, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy
5Pediatric Radiology Unit, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy
6Immune-Hematology Service, Tranfusion Center, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy
Received Date: 17 March 2026
Accepted Date: 24 March 2026
Published Date: 28 March 2026
Citation: Cristini E, Ivan Taietti I, Eboli C, Rossano M, Di Stasio F, et al. (2026) Long-Term Outcomes of Combined Core Decompression, Bone Marrow Aspirate Transplantation, and Platelet-Rich Plasma for the treatment of Femoral Head Osteonecrosis in children. Arch Pediatr 11: 340. DOI: https://doi.org/10.29011/2575-825X.100340 href="https://doi.org/10.29011/2575-825X.100340" target="_blank">https://doi.org/10.29011/2575-825X.100340
Abstract
Osteonecrosis (ON) can result from glucocorticoid use, and it is influenced by genetic, metabolic factors, and blood flow restriction. Treatment approaches for ON vary, and, though to its rarity in pediatric population, its correct therapeutic management is not standardized. We reported the case of a 14-year-old girl affected by granulomatosis with polyangiitis with severe pulmonary and renal involvement, initially treated with high-dose of steroids, rituximab, and cyclophosphamide, and then eculizumab for thrombotic microangiopathy. After six months, while in complete remission, the patient developed bilateral widespread ON of the femoral heads as evidenced by magnetic resonance imaging (MRI). Considering the young age and early stage of ON, after multidisciplinary discussion, core decompression (CD) of the femoral heads was performed with subsequent implantation of bone marrow tissue combined with platelet-rich plasma (PRP) to promote cellular regeneration. The procedure was completed with the injection of biological bone cement in place, according to the subchondroplasty technique. Over a three-year follow-up, she experienced full recovery of joint function, absence of pain, and stable MRI findings, allowing unrestricted participation in sports. Literature review supports that CD combined with regenerative therapies may prevent femoral head collapse and delay or avoid the need for total hip arthroplasty, a less desirable option in pediatric patients due to prosthesis longevity concerns. We highlighted the possibility of using a novel safe and efficient therapeutic approach to ON in pediatric patients. This novel therapeutic approach warrants further investigation through larger studies to establish its role as a first-line treatment in pediatric ON.
Keywords: Avascular Necrosis (AVN); Osteonecrosis of the Femoral Head (ONFH); Glucocorticoids (GC); Stem Cell Therapy; Platelet-Rich Plasma (PRP).
Introduction
Osteonecrosis (ON), also called avascular necrosis (AVN), is a clinical entity characterized by the death of bone tissue (extensive bone and red medulla necrosis) that results in a collapse of bony architecture, destruction of articular cartilage, with pain, and functional impairment. The etiology remains unclear. The mechanism of AVN development is the compromised vascular supply and progressive ischemia of the subchondral bone. This can be secondary to traumatic events or non-traumatic conditions such as idiopathic ones, chronic alcohol intake, glucocorticoid (GC) use, and rheumatic disorders, especially systemic lupus erythematosus (SLE). Non-traumatic AVN is influenced by various genetic, metabolic, and vascular factors [1,2,3]. GC are a major risk factor for AVN development, impacting endothelial cells, promoting hypercoagulability and fat cell hypertrophy, and inhibiting angiogenesis, thus reducing micro-vessel blood flow and oxygen delivery [4].
AVN typically affects the epiphyses of long bones (e.g. femoral head and condyles, distal tibia, and humeral head), often presenting with multifocal distribution [5]. Treatment approaches for ON vary depending on the severity of the condition. Small, silent lesions can often be managed conservatively, whereas symptomatic or larger weight-bearing lesions typically require surgery. Medications like bisphosphonates and warfarin may help prevent progression. Advanced cases often require grafting or hip replacement. Newer regenerative approaches, such as platelet-rich plasma (PRP) and stem cell therapy, are being explored for early disease [6,7]..
No study has focused on therapeutic effect of these novel approaches on the long-term outcome of children with steroidinduced ON of the femoral head (ONFH). We aim to present our experience in a girl with bilateral ONFH treated with core decompression (CD) associated with injection of autologous bone marrow concentrate (BMC) and PRP comparing our experience with literature evidence available to date.
Combined CD, BMC Transplantation, and PRP treatment in practice
A girl presented to our emergency room was diagnosed with antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) granulomatosis with polyangiitis at 14 years old, after a twomonth history of migrating arthralgia involving multiple joints. At disease onset, she presented with palpable purpura at lower limb, gastrointestinal complaints with hematochezia, polyarthritis, and renal involvement. The initial diagnostic hypothesis was of Henoch-Schoenlein Purpura with renal and gastrointestinal involvement. However, suddenly, the patient experienced acute dyspnea and desaturation, leading to urgent chest X-ray with bilateral parenchymal haziness and blood examination with decreased hemoglobin levels, elevated D-dimer, and troponins. Therefore, urgent chest computed tomography (CT) with contrast showed findings consistent with hemorrhagic alveolitis, without signs of pulmonary embolism. High titer positivity for antineutrophil cytoplasmic antibodies proteinase-3 (c-ANCA PR3) was later confirmed. The patient started induction therapy with high dose of methylprednisolone by intravenous pulses (1 gr per day for three days) followed by methylprednisolone 2mg/kg/ day.
The diagnostic workup was completed with kidney biopsy that revealed a necrotizing glomerulonephritis. She was treated with rituximab at 375 mg/m2/weekly, interrupted after the second infusion because of a worsening in renal function that let us to switch to oral cyclophosphamide and repeat high doses of methylprednisolone for other 3 pulses. Despite this treatment, the creatinine level kept increasing and she started to present progressive thrombocytopenia. A treatment with complement inhibition (eculizumab) was started obtaining a sudden and sustained remission [8].
6 months later, the patient started complaining increasing hip joint bilateral pain with bilateral limitation in the inward rotation of the hips. Pelvic X-ray was conducted with normal findings. Therefore, pelvic Magnetic Resonance Imaging (MRI) performed one week after the onset of the symptoms, showed bilateral avascular necrosis of the femoral head (left > right) with preserved height and morphology of both femoral heads (Figure 1).
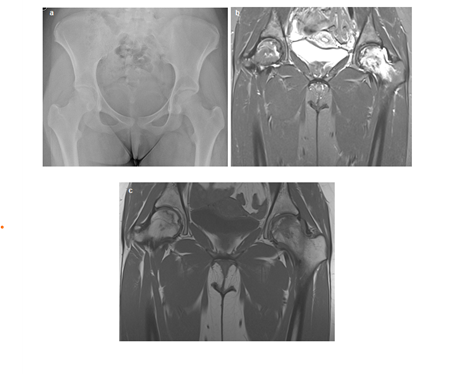
Figure 1 : (a) Hip X-ray at the onset of AVN, revealing no significant bony abnormalities. (b, c) Subsequent coronal Magnetic Resonance Imaging (MRI) performed within days, including STIR (b) and T1-weighted (T1W) (c) sequences, demonstrating diffuse bone marrow edema in both femoral heads, with greater involvement on the left. Notably, the left femoral head exhibits a serpiginous line of hyperintensity, the ‘double line sign’, indicative of subchondral collapse.”
Considering the young age and early stage of ON, after multidisciplinary discussion, she underwent bilateral femoral head decompression surgery and infiltration with PRP, mesenchymal cells, and subchondroplasty. Initially, the bone marrow was reduced from 50 to 6-7 ml through centrifugation to concentrate the cellular component, then combined with platelet-rich plasma (PRP) prepared from umbilical cord blood to promote cellular regeneration. The procedure was completed with the injection of biological bone cement in place according to the subchondroplasty technique. The postoperative course was uneventful. Then she received postoperative hyperbaric therapy. No additional therapy (e.g. bisphosphonate therapy) was administered. Subsequent follow-up included physical therapy to optimize joint function and prevent further complications.
Regular clinical and imaging follow-up have been performed to date showing complete restoration of joint functionality. Three years after the procedure, the girl shows no functional limitation in the hip joints and engages sport activities, and MRI confirmed substantial stability of the condition and stabilization of the cortical profile of the hips (Figure 2).
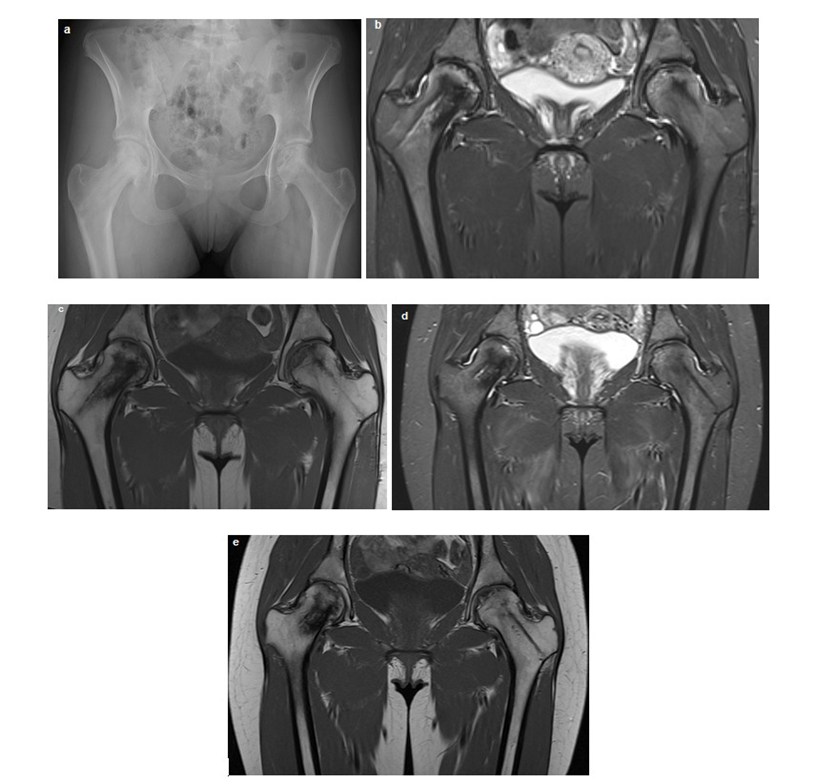
Figure 2: Radiographic and Magnetic Resonance Imaging (MRI) Follow-up of Bilateral Femoral Head Osteonecrosis. (a) Hip X-ray, approximately 12 months post-surgical intervention, demonstrating preserved femoral head height and morphology despite residual bone structural damage, characterized by areas of resorption and sclerosis, more pronounced on the left side. (b, c, d, e) Sequential coronal MRI images, including STIR and T1-weighted (T1W) sequences, acquired at 16 months (b, d) and 3 years (c, e) post-surgery. These images illustrate progressive improvement in bone marrow signal within the femoral heads, with a notable reduction in bilateral bone marrow edema and stabilization of structural bone changes.
Evidence from Literature
Corticosteroid-induced AVN is a rare, but severe complication in children and adolescents with rheumatologic diseases, such as vasculitis (in this case granulomatosis with polyangiitis) [9-12]. Among patients with AAV a prevalence of 18% was reported [13]. It has also been hypothesized that AVN could arise in the absence corticosteroids use, but the literature review conclude that it should not be listed as an independent cause of AVN [14]. Overall, AVN is a multifactorial disease. In autoimmune disorders, immunologic factors have been implicated for its pathogenesis, such as small vessel vasculitis or other disease-associated features and antiphospholipid antibodies [15]. Conversely, genetic factors play a key-role in AVN pathogenesis with some TIMP4 Single Nucleotide Polymorphism (SNPs) associated with decreased risk of steroid-induced ONFH in the population of northern China [16]. Moreover, Yamazaki et al. reported a Japanese trisomy X female adolescent with childhood-onset SLE complicated by ONFH thus suggesting how also chromosomal abnormalities could increase risk of AVN in rheumatic patients [17].
ON is more common in female adolescents [18,19]. It is often a symmetrical process that commonly involves the hip joint [5], and its onset could be insidious or vague in early stages, and even asymptomatic [20]. The high dosage use of steroids is often described as a possible risk factor for avascular ON [21], but it may depend on the possible synergic effect of other immune suppressors [4], and a wide spectrum of factors (e.g. genetic predisposition and epigenetic phenomena, the underlying disease) [1]. The reported patient was also administered with immune suppressants and biologic drugs in addition to steroid treatment. Nevertheless, systemic steroids have been proved to be an independent risk factor for ONFH in AAV patients [22].
Overall, the optimal treatment of ON is controversial, and numerous options have been reported in the literature, including non-operative and surgical procedures. Conservative management is usually enough for silent, small area ON, while symptomatic lesions often necessitate surgical intervention (such as CD or vascularized fibular grafting), with extracorporeal shockwave therapy as an alternative. In cases of medium/large lesions or those involving weight-bearing regions, bone collapse is a common complication, often requiring total joint replacement. Combination therapy with bisphosphonates or warfarin alongside high-dose corticosteroids shows promise in preventing ON. In advanced stages, surgical interventions like bone grafting or hip replacement may become necessary [6,7]. Noteworthy, orthopedic surgery is unfrequently required in pediatric patients [19], and prothesis is not an ideal treatment in the pediatric population due to its possible wear and the long-life treatment with steroids [21]. At present, CD, proximal femoral osteotomy, and vascularized or non-vascularized bone grafting are widely used in adults with hip AVN to delay and prevent femoral head collapse. In recent years, regenerative techniques such as platelet-rich plasma (PRP) and stem cell therapy have been increasingly used to assist in the treatment of early ONFH [23].
To date, there are several reports of alternative treatment options in avascular ON. CD with BMC, and bone grafting stimulate a healing response and can allow for immediate weight-bearing postoperatively. It results in a valid treatment option of early ONFH [24]. BMC contains clinically relevant concentrations of Interleukin 1 receptor antagonist (IL-1Ra), the natural antagonist that competitively binds to IL-1β and IL-1α cell surface receptors, inhibiting IL-1 catabolism, thus responsible for the reported beneficial effect [25]. BMC treatment has been proved effective for corticosteroid-induced ONFH in SLE, also in a female adolescent [26].
Ankem et al. reported intraosseous bioplasty (IOBP) as a safe and reproducible way to treat subchondral defects in young patients with signs of early osteoarthritis of the hip joint. IOBP consists in combining BMC or concentrated PRP with demineralized bone matrix as a bone substitute before injecting into a subchondral bone defect [27]. PRP is generated by centrifugation of peripheral blood resulting in increased platelet concentration. The rationale of PRP use is based on the provision by PLT of multiple growth factors with known roles in target cell activation, cell recruitment, cartilage matrix production, and modulation of the inflammatory response: (i) PDGF induces mesenchymal stem cells (MSC) proliferation and inhibits IL-1β-induced chondrocyte apoptosis and inflammation; (ii) TGF-β1 stimulates chondrogenesis of synovium and bone marrow-derived MSCs, inhibit IL-1β-mediated inflammation, and enhance cartilage healing; (iii) TGF-β2 decreases collagen type 2 cleavage and chondrocyte hypertrophy through inhibition of IL1β and TNF-α. PRP was also reported to be effective alone in the treatment of ON [28].
PRP, as BMC, are currently used in addition to hip decompression for corticosteroid-induced ONFH. Hip decompression is a surgical procedure aimed at relieving pressure within the femoral head, which can help improve blood flow and reduce further damage. BMC and PRP are likely used as adjunct therapies to promote tissue repair and regeneration. This combination therapy provided an excellent long-term prognosis in terms of femoral head collapse and total hip arthroplasty (THA) free survival in adult patients [29]. Moreover, several investigators demonstrated that CD combined with BMC and PRP can completely resolve the necrotic lesion and delay disease progression in patients with early-stage ONFH, thus improving functional outcomes, and radiographic findings, also with significant pain relief [30]. Moreover, PRP used after CD enhances the survivorship free from reoperation for THA and femoral head collapse in the early stages of avascular necrosis of the hip than CD alone [31]. These findings were also confirmed by a meta-analysis by Wang et al [32].
Conclusion
This case study with literature review illustrates the effective use of a combined therapeutic strategy to treat early-stage steroidinduced ONFH in an adolescent with AAV. The favorable longterm outcome, with full functional recovery and radiological stability over three years, highlights the potential of regenerative approaches to maintain joint integrity and delay or prevent the need for THA, which is particularly undesirable in pediatric patients. While current evidence from adult studies supports the efficacy of combining core decompression with biological adjuvants, pediatric data remain scarce. Our findings suggest that such integrative, joint-preserving therapies may represent a valuable first-line option for children and adolescents with glucocorticoidinduced ON.
We also advocate for larger prospective studies with long-term follow-up to validate and clarify the superiority of this procedure in the pediatric population, thereby optimizing treatment protocols.
Acknowledgments
This study was partially funded by the Italian Ministry of Health, current research IRCCS.
Ethical Guidelines
The patient and her parents signed the informed consent, and the patient was included in the study protocol approved by the local Institutional Review Board (Comitato Etico Territoriale Lombardia 3, N 0010572). Informed consent was obtained from the patient and her parents for the publication of the clinical case.
Conflict of Interest
The authors do not declare any competing interests.
References
- Chang C, Greenspan A, Gershwin ME (2020) The pathogenesis, diagnosis and clinical manifestations of steroid-induced osteonecrosis. J Autoimmun 110: 102460.
- Mont MA, Cherian JJ, Sierra RJ, Jones LC, Lieberman JR (2015) Nontraumatic Osteonecrosis of the Femoral Head: Where Do We Stand Today?: A Ten-Year Update. J Bone Joint Surg Am 97: 16041627.
- Muñoz-Grajales C, Yilmaz EB, Svenungsson E, Touma Z (2023) Systemic lupus erythematosus and damage: What has changed over the past 20 years? Best Pract Res Clin Rheumatol 37:101893.
- Kwon HH, Bang SY, Won S, Park Y, Yi JH, et al. (2018) Synergistic effect of cumulative corticosteroid dose and immunosuppressants on avascular necrosis in patients with systemic lupus erythematosus. Lupus 27: 1644-1651.
- Powell C, Chang C, Naguwa SM, Cheema G, Gershwin ME (2010) Steroid induced osteonecrosis: An analysis of steroid dosing risk. Autoimmun Rev 9: 721-743.
- Caramaschi P, Biasi D, Dal Forno I, Adami S (2012) Osteonecrosis in Systemic Lupus Erythematosus: An Early, Frequent, and Not Always Symptomatic Complication. Autoimmune Dis 1 : e725249.
- Kunze KN, Sullivan SW, Nwachukwu BU (2022) Updates on Management of Avascular Necrosis Using Hip Arthroscopy for Core Decompression. Front Surg 9: 662722.
- Ribes D, Belliere J, Piedrafita A, Faguer S (2019) Glucocorticoidfree induction regimen in severe ANCA-associated vasculitis using a combination of rituximab and eculizumab. Rheumatology (Oxford) 58: 2335-2337.
- Shigemura T, Nakamura J, Kishida S, et al. Incidence of osteonecrosis associated with corticosteroid therapy among different underlying diseases: prospective MRI study. Rheumatology (Oxford) 50: 20232028.
- Hirahara K, Kano Y, Asano Y, Shiohara T (2013) Osteonecrosis of the femoral head in a patient with Henoch-Schönlein purpura and druginduced hypersensitivity syndrome treated with corticosteroids. Acta Derm Venereol 93: 85-86.
- Mimura N, Iwamoto T, Furuta S, Ikeda K, Kobayashi Y, et al. (2023) Prevalence and risk factors of osteonecrosis of the femoral head in patients with ANCA-associated vasculitis: a multicentre cohort study. RMD Open 9: e002787.
- Nejadhosseinian M, Babagoli M, Faezi ST, Haerian H, Shahram F, et al. (2023) Osteonecrosis as a rare musculoskeletal complication in Behcet’s disease- the largest case series with literature review. BMC Rheumatol 7: 42.
- Mimura N, Iwamoto T, Furuta S Ikeda K, Kobayashi Y, et al. (2023) Prevalence and risk factors of osteonecrosis of the femoral head in patients with ANCA-associated vasculitis: a multicentre cohort study. RMD Open 9: e002787.
- Abraham RR, Meyerhoff JO (2013) Does vasculitis alone cause AVN? A review of literature. Rheumatol Int 33: 2671-2673.
- Tektonidou MG, Moutsopoulos HM (2004) Immunologic factors in the pathogenesis of osteonecrosis. Orthop Clin North Am 35: 259-263.
- Wang J, An F, Cao Y, Gao H, Sun M, et al. (2019)Association of TIMP4 gene variants with steroid-induced osteonecrosis of the femoral head in the population of northern China. Peer J 7: e6270.
- Yamazaki S, Akutsu Y, Shimbo A, Shimizu M, Segawa Y, et al. (2021) Childhood-onset systemic lupus erythematosus with trisomy X and the increased risk for bone complications: a case report. Pediatr Rheumatol Online J 19: 20.
- Yang Y, Kumar S, Lim LSH, Silverman ED, Levy DM (2015) Risk Factors for Symptomatic Avascular Necrosis in Childhood-onset Systemic Lupus Erythematosus. J Rheumatolo 42: 2304-2309.
- Taietti I, Zini F, Conti EA, Cristini E, Borzani I, et al. (2025) Avascular necrosis in pediatric rheumatic diseases: an Italian retrospective multicentre study. Ital J Pediatr 51: 20.
- Tsai HL, Chang JW, Lu JH, Liu CS (2022) Epidemiology and risk factors associated with avascular necrosis in patients with autoimmune diseases: a nationwide study. Korean J Intern Med 37: 864-876.
- Hannon CP, Goodman SM, Austin MS, Yates A, Guyatt G, et al. (2023) 2023 American College of Rheumatology and American Association of Hip and Knee Surgeons Clinical Practice Guideline for the Optimal Timing of Elective Hip or Knee Arthroplasty for Patients With Symptomatic Moderate-to-Severe Osteoarthritis or Advanced Symptomatic Osteonecrosis With Secondary Arthritis for Whom Nonoperative Therapy Is Ineffective. The Journal of Arthroplasty 38: 2193-2201.
- Mimura N, Iwamoto T, Furuta S, Ikeda K, Kobayashi Y, et al. (2023) Prevalence and risk factors of osteonecrosis of the femoral head in patients with ANCA-associated vasculitis: a multicentre cohort study RMD Open 9: e002787.
- Hines JT, Jo WL, Cui Q, Mont MA, Koo KH, et al. (2021) Osteonecrosis of the Femoral Head: an Updated Review of ARCO on Pathogenesis, Staging and Treatment. J Korean Med Sci 36: e177.
- Arbeloa-Gutierrez L, Dean CS, Chahla J, Pascual-Garrido C (2016) Core Decompression Augmented With Autologous Bone Marrow Aspiration Concentrate for Early Avascular Necrosis of the Femoral Head. Arthroscopy Techniques 5 : e615-e620.
- Cassano JM, Kennedy JG, Ross KA, Fraser EJ, Goodale MB, et al. (2018) Bone marrow concentrate and platelet-rich plasma differ in cell distribution and interleukin 1 receptor antagonist protein concentration. Knee Surg Sports Traumatol Arthrosc 26: 333-342.
- Yoshioka T, Mishima H, Akaogi H, Sakai S, Li M, et al. (2011) Concentrated autologous bone marrow aspirate transplantation treatment for corticosteroid-induced osteonecrosis of the femoral head in systemic lupus erythematosus. Int Orthop 35: 823-829.
- Ankem HK, Diulus SC, Maldonado DR, Declet VO, Rosinsky PJ, et al. (2020) Arthroscopic-Assisted Intraosseous Bioplasty of the Acetabulum. Arthrosc Tech 9: e1531-e1539.
- Ibrahim V, Dowling H (2012) Platelet-Rich Plasma as a Nonsurgical Treatment Option for Osteonecrosis. PM R 4:1015-1019.
- Houdek MT, Wyles CC, Smith JRH, Terzic A, Behfar A, et al.(2021) Hip decompression combined with bone marrow concentrate and plateletrich plasma for corticosteroid-induced osteonecrosis of the femoral head. Bone Jt Open 2: 926-931.
- Martin JR, Houdek MT, Sierra RJ (2013) Use of concentrated bone marrow aspirate and platelet rich plasma during minimally invasive decompression of the femoral head in the treatment of osteonecrosis. Croat Med J 54: 219-224.
- Aggarwal AK, Poornalingam K, Jain A, Prakash M (2021)Combining Platelet-Rich Plasma Instillation With Core Decompression Improves Functional Outcome and Delays Progression in Early-Stage Avascular Necrosis of Femoral Head: a 4.5- to 6-Year Prospective Randomized Comparative Study. J Arthroplasty 36: 54-61.
- Wang J, Xu P, Zhou L (2023) Comparison of current treatment strategy for osteonecrosis of the femoral head from the perspective of cell therapy. Front Cell Dev Biol 11: 995816.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.