Life-Threatening Sublingual Hematoma and Traumatic Lingual Artery Aneurysm after Dental Extraction: Successful Management with Endovascular Embolization and Tracheostomy
by Maarten Verbist1,2*, Patrick Stabel3, Ine Leunen4, Dirk Servaes5, Alexander De Moor1, Laury Grosjean1, Thomas Claeys1
1Department of Oral and Maxillofacial Surgery, AZ Turnhout, Turnhout, Belgium
2OMFS IMPATH Research Group, Leuven University Hospitals
3Head of Department of Vascular and Thoracic Surgery, AZ Turnhout, Turnhout, Belgium
4Intensive Care, AZ Turnhout, Turnhout, Belgium
5Head of Department of General and Abdominal Surgery, AZ Turnhout, Turnhout, Belgium
*Corresponding Author: Maarten Verbist, Department of Oral and Maxillofacial Surgery, AZ Turnhout, Steenweg op Merksplas 44, 2300 Turnhout, Belgium
Received Date: 08 February 2025
Accepted Date: 13 February 2026
Published Date: 16 February 2026
Citation: Verbist M, Stabel P, Leunen I, Servaes D, De Moor A, et al. (2026). Life-Threatening Sublingual Hematoma and Traumatic Lingual Artery Aneurysm after Dental Extraction: Successful Management with Endovascular Embolization and Tracheostomy. Ann Case Report. 11: 2532. DOI: https://doi.org/10.29011/2574-7754.102532
Abstract
Background: Sublingual hematomas following dental extractions are extremely rare but may progress rapidly and cause life-threatening airway compression. Early recognition and interdisciplinary management are essential to prevent acute airway obstruction.
Case presentation: We report a unique case of a 60-year-old male patient with an expanding sublingual hematoma after extraction of multiple teeth in the lower left jaw in another hospital. He presented with stridor, dyspnoea and dysphagia. A first CT-scan revealed active arterial bleeding of the left lingual artery with acute airway obstruction. The patient was urgently transferred to the operating theatre and underwent emergency intubation and drainage of the hematoma. After four days of intubation, a tracheostomy was performed. Initial postoperative CT-scans showed a stable non-resolving hematoma. Ten days after initial surgical exploration, an expanding traumatic lingual artery pseudoaneurysm was observed on CT-scan. The lingual artery was successfully coiled endovascularly.
Management and outcome: Hemostasis was achieved immediately after embolization, followed by a decrease of the sublingual hematoma. The patient recovered completely, with normal swallowing and tongue mobility but residual hypoesthesia of the left lingual nerve.
Conclusion: This case highlights the importance of prompt imaging, airway control, and endovascular intervention in managing potentially life-threatening submandibular hematomas following routine dentoalveolar procedures.
Keywords: Hematoma; Lingual Artery; Endovascular Embolization; Tracheostomy; Tooth Extractions; Oral and Maxillofacial Surgery.
Introduction
Sublingual hematomas are exceptionally uncommon [1]. They can occur spontaneously due to anticoagulant therapy or hypertension (1-3); or after dental implant placement in the anterior mandible [4 -5]. The hematoma can progress rapidly because of the confined anatomy of the oral floor and sublingual and submandibular space. An increase in volume can cause displacement of the tongue base and subsequent airway obstruction, therefore it is also called ‘pseudo-Ludwig Angina’ [1, 7]. It should be considered as an emergency and rapid airway management is crucial. Reported sources of bleeding include branches of the facial, submental, or lingual arteries [1, 6].
We present a recurrent, expanding sublingual hematoma following a mandibular tooth extraction, successfully treated with surgical decompression, emergency tracheostomy and endovascular embolization of the lingual artery. This case emphasizes the importance of early diagnosis, airway security, and multidisciplinary collaboration. To our knowledge, this is the first case report of a sublingual hematoma and lingual pseudoaneurysm after dental extraction, managed with endovascular coiling.
Case Presentation
A 60-year-old Caucasian male without significant medical history underwent a routine extraction of all teeth in the upper jaw, and the lower left premolars under general anaesthesia in another hospital. Shortly after dental extraction, he presented with a diffuse swelling of the mouth floor, without any alarming signs. Within 24 hours, the patient experienced increasing sublingual and submandibular swelling, without symptoms of dysphagia or progressive dyspnoea. Therefore, the treating surgeon choose to explore the hematoma under general anaesthesia 24 hours after dental extraction. No active bleeding was found. And the patient was dismissed the following day.
Five days after the extraction, the patient was hospitalized again due to recurrent swelling and treated with IV-antibiotics to prevent bacterial infection of the hematoma. He was kept in observation for three days and was successfully discharged from the hospital. However, eight hours after discharge, he consulted the emergency department again with severe swelling of the floor of the mouth, dysphagia, and progressive stridor, dyspnoea and severe hypertension.
Clinical examination showed a large swelling, pushing the tongue cranially to the palate and the parapharyngeal space. CT-scan with IV contrast (Iodine) showed progressive active arterial bleeding of the left lingual artery (Figure 1).
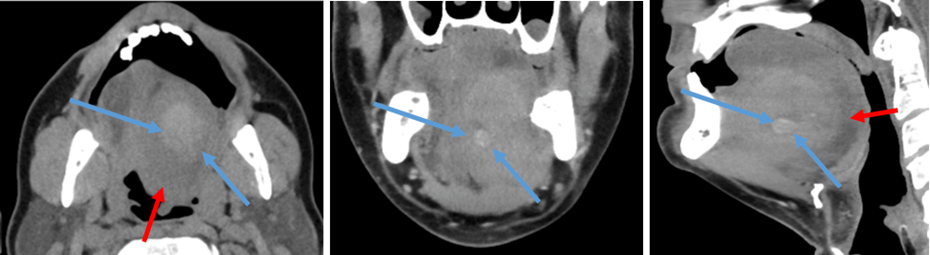
Figure 1: CT scan. Active sublingual bleeding with contrast extravasation (blue arrows) and severe airway compression of the hematoma (red arrows) (axial, coronal and sagittal slices)
The patient was urgently transferred to the operating theatre and underwent emergency intubation. Our experienced surgical team was stand-by to perform a surgical tracheostomy if needed and an immediate drainage of the mouth floor hematoma was performed under general anaesthesia (Figure 2). IV-Tranexamin acid and broad-spectrum antibiotics were given. The patient was left intubated and was transferred to the intensive care unit (ICU). Postoperative clinical and radiological follow-up showed a residual inactive, stable hematoma and normalisation of the arterial diameter of the lingual artery. Four days after intubation, a surgical tracheostomy (Tracoe Twist Plus Canule 8.0) was performed because of the residual mass effect on the airway (Figure 2).

Figure 2: Left, mid: Clinical postoperative situation. Note the severe swelling of the oral floor (red arrow) and the lingual drain in place (blue arrow). Right image: tracheostomy, four days after intubation.
Postoperative scan, ten days after initial evacuation of the hematoma showed a progressive enlargement of the lingual artery, suggesting a traumatic lingual arterial pseudoaneurysm. Selective angiography identified active bleeding from the left lingual artery and coil embolization was performed successfully. Post-embolization angiography confirmed cessation of extravasation (Figure 3).
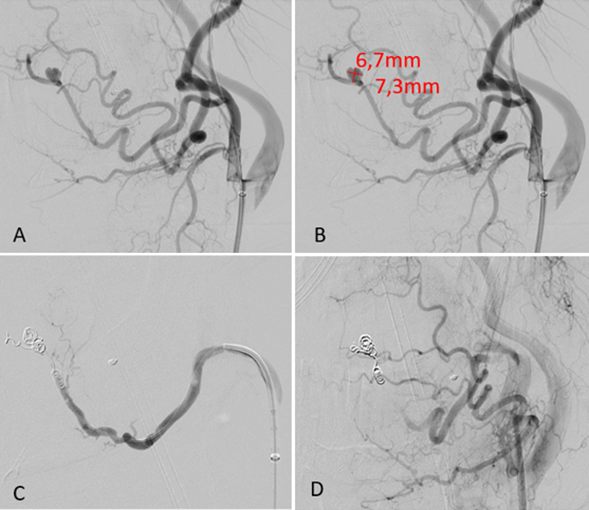
Figure 3: pre (A-B) -and post (C-D) endovascular coiling. Note the dimensions of the aneurysm (7.3x6.7mm) (courtesy: dr. P. Stabel, AZTurnhout).
After endovascular treatment, we observed gradual regression of the hematoma during hospitalization and decannulation was performed six days after embolization. The patient recovered completely, with normal swallowing and tongue mobility, although mild hypoesthesia of the left lingual nerve remained up to three months after surgery (Figure 4).

Figure 4: intra-oral and extra-oral situation 14 days after endovascular coiling.
Discussion
Sublingual hematomas after dental extraction are rare but potentially fatal due to the risk of rapid airway compromise [7]. The floor of the mouth and adjacent cervical compartments have limited compliance; therefore, hematoma expansion can quickly obstruct the oropharyngeal airway.
Previous reports suggest that hypertension [1,3], supratherapeutic oral anticoagulants [1,3,7] and arterial injury involving the submental or facial branches [4,5] is the most common cause of a sublingual hematoma. This case differs from previous cases because of the lack of oral anticoagulants, progressive development of an arterial (pseudo)aneurysm and the use of endovascular coiling. Our hypothesis state that a blunt trauma during extraction, resulted in a slowly growing, traumatic pseudoaneurysm that ruptured a week after the initial extraction and therefore resulted in this rapidly growing, high flow life-threatening sublingual hematoma.
Airway protection has priority based on the Advanced Life Support (ALS)-guidelines [8]. Orotracheal intubation may be difficult or impossible due to tongue base displacement and restricted mandibular mobility. In this case, highly skilled anaesthesiologists could intubate safely with fibre-optic scopy. An experienced surgical team was standby to perform an urgent tracheostomy if necessary. Postoperative imaging showed an increasing diameter of the lingual artery, highlighting the need for further vascular treatment.
Endovascular embolization is increasingly recognized as an effective and minimally invasive treatment for cervicofacial haemorrhage and previous cases of endovascular treatment of lingual pseudoaneurysm are described [9-12]. It allows precise localization and control of bleeding, avoiding the need for extensive surgical exploration and ligation of the external carotid artery [9].
This case underscores the need for surgeons to be alert to early signs of expanding sublingual and submandibular hematomas, even after routine procedures. Collaboration between radiologists, maxillofacial surgeons, endovascular surgeons, and anaesthesiologists is crucial for successful management of this very rare, but life-threatening complication.
Conclusion
Acute sublingual hematomas after routine dentoalveolar procedures can be rapidly life threatening. Prompt recognition, early airway stabilization, and minimally invasive endovascular embolization provide an effective and safe treatment pathway with favourable outcomes.
Ethical considerations: Informed consent for publication of clinical details and images was obtained from the patient. No identifiable information is presented.
Author contributions: M. Verbist-clinical management, manuscript drafting, surgical procedure; D. Servaes- surgical tracheostomy, critical revision manuscript; P. Stabel: angiography and embolization, critical revision manuscript; I. Leunen-airway management, manuscript review; A. De Moor, L. Grosjean, T. Claeys-supervision surgical procedure critical revision manuscript.
References
- Marin E, Fauconnier S, Bauters W, Huvenne W. (2020). Idiopathic spontaneous sublingual hematoma: A case report and literature review. Oral Maxillofac Surg. 24: 117-120.
- González-García R, Schoendorff G, Muñoz-Guerra MF, Rodríguez-Campo FJ, Naval-Gías L, et al. (2006). Upper airway obstruction by sublingual hematoma: A complication of anticoagulation therapy with acenocoumarol. Am J Otolaryngol Head Neck Med Surg. 27: 129-132.
- Satpathy S, Guha R, Satpathy A, Guha P. (2015). Spontaneous sublingual space hematoma secondary to hypertension: A case report and review of literature. Natl J Maxillofac Surg. 6: 96.
- Isaacson TJ. (2004). Sublingual hematoma formation during immediate placement of mandibular endosseous implants. J Am Dent Assoc. 135: 168-172.
- Del Castillo-Pardo De Vera JL, López-Arcas Calleja JM, Burgueño-García M. (2008). Hematoma of the floor of the mouth and airway obstruction during mandibular dental implant placement: A case report. Oral Maxillofac Surg. 12: 223-226.
- Flanagan D. (2003). Important arterial supply of the mandible, control of an arterial hemorrhage, and report of a hemorrhagic incident. J Oral Implantol. 29: 165-173.
- Ekin U, Hazari A, Alyassin N, Alcantara A, Azzam MH, et al. (2025). Successful management of pseudo-Ludwig angina from supratherapeutic warfarin use: A case report. Clin Pract Cases Emerg Med. 9: 90-94.
- Soar J, Böttiger BW, Carli P, Carmona FJ, Cimpoesu D, et al. (2025). European Resuscitation Council Guidelines 2025 adult advanced life support. Resuscitation. 215: 110769.
- Rathod R, Choudhary N, Hosur B, Bansal S. (2021). Early presentation of traumatic pseudoaneurysm of deep lingual artery as a massive oral bleed. BMJ Case Rep. 14: e000000.
- DiStefano JF, Maimon W, Mandel MA. (1977). False aneurysm of the lingual artery. J Oral Surg. 35: 918-920.
- Handa KK, Shunyu NB. (2008). Post traumatic pseudoaneurysm of the lingual artery. Indian J Otolaryngol Head Neck Surg. 60: 356-359.
- Masella PC, Hanson MM, Hall BT, Verghese JJ, Kellicut DC. (2014). Posttraumatic lingual artery pseudoaneurysm treated with ultrasound-guided percutaneous thrombin injection. Ann Vasc Surg. 28: 1317.e11-1317.e15.
- Margallo L, De Zárate EO, Franco M, Garcia-Iruretagoyena M, Cherro R, et al. (2018). Lingual artery pseudoaneurysm after severe facial trauma. Craniomaxillofac Trauma Reconstr. 11: 219-223.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.