Knowledge, Practice and Associated Factors of Home-Based Management of Diarrhoea among Caregivers at Ola During Childrens’ Hospital: a Call to Action?
by Akhigbe Irene Eseohe*, Jones Cheryl Olabisi, Sandy Solomon Fallah Foa
Ola During Children Hospital, University of Sierra Leone Teaching Hospital Complex, Freetown, Sierra Leone.
*Corresponding author: Akhigbe Irene Eseohe, Consultant Paediatrician and Neonatologist, Ola During Children Hospital, University of Sierra Leone Teaching Hospital Complex, Freetown, Sierra Leone.
Received Date: 11 October 2025
Accepted Date: 18 October 2025
Published Date: 20 October 2025
Citation: Akhigbe IE, Jones CO, Sandy SFF (2025) Knowledge, Practice and Associated Factors of Home-Based Management of Diarrhoea among Caregivers at Ola During Childrens’ Hospital: a Call to Action?. Arch Pediatr 10: 336. https://doi.org/10.29011/2575-825X.100336
Abstract
Background: Globally, diarrhoeal disease is the second leading cause of death among children under five, accounting for approximately 1.5 million deaths each year. These diarrhoea-related deaths could have been prevented by simple home management using oral rehydration therapy. This study was therefore done to assess caregivers’ knowledge, attitude, and practice (KAP) toward diarrhoea prevention and home-based management, which invariably impacts the burden of childhood diarrhoea diseases. Methods: Institutional based cross-sectional study was conducted at the pediatrics general wards of Ola During Children’s hospital. Data was collected using a structured questionnaire and was entered and analysed using the Statistical Package for Social Sciences (SPSS) version 25.0 for IBM. Results: A total of 110 caregivers participated in the study. From the total 110 caregivers, 81 (73.6%) caregivers had good knowledge about the prevention and home-based management of under-5 diarrheal diseases. The majority had a positive attitude (89; 80.9) and a similar proportion demonstrated good care practices (93; 84.5%). Educational status (p = 0.002), employment (p = 0.041) and urban residence (p = 0.019) were significantly associated with good practice of home management of diarrhoea among children under five years old. Conclusion: Caregivers demonstrated good overall knowledge, attitude, and practice regarding diarrhoea home management. Nonetheless, gaps remain in understanding home-based care in the management of childhood diarrhoea illnesses. Socio-economic factors particularly education and urban living were key determinants of positive health behaviors.
Keywords: Knowledge; Attitude; Practice; Caregivers; Prevention; Home-based management; Diarrhea; Under-five children
Introduction
Diarrhoea, a common illness marked by frequent loose or watery stools occurring three or more times daily [1], remains a major public health issue-especially in low- and middle-income countries-due to its adverse effects on the survival, growth, and development of infants and young children [2,3]. Globally, diarrhoeal disease is the second leading cause of death among children under five, accounting for approximately 1.5 million deaths each year, with sub-Saharan Africa bearing the highest burden [4-6] In Sierra Leone, diarrhoea ranks among the top causes of childhood mortality, responsible for an estimated 64.38 deaths per 100,000 children under five [7]. These fatalities often result from fluid and electrolyte loss, leading rapidly to dehydration [8,9]. Additionally, each diarrhoeal episode can cause a daily weight loss of 20–40 g, contributing to significant growth deficits in early childhood [10].While diarrhoeal diseases can be mitigated through both primary and secondary prevention, effective homebased management especially through the prompt use of oral rehydration solutions (ORS) or appropriate home available fluids is essential for reducing mortality [11]. The World Health Organization (WHO) and UNICEF recognize the contribution of home-based diarrhoea management in improving child survival, and advocates for caregivers’ empowerment through education and awareness creation on proper diarrhoea prevention and management practices [12,13]. This study was therefore done to assess caregivers’ knowledge, attitude, and practice (KAP) toward diarrhoea prevention and home-based management, which invariably impacts the burden of childhood diarrhoea diseases.
Materials and Methods
Study Design and Participants
This descriptive cross-sectional study was conducted among caregivers of children admitted to the general paediatric wards at ODCH between May and June 2024. Participants were selected using a non-probability convenience sampling method. Eligible participants were primary caregivers responsible for healthcare decisions regarding the child. Individuals with physical impairments affecting communication were excluded.
Study Setting
ODCH is a government tertiary paediatric hospital in the Freetown, Sierra Leone, serving as part of the University of Sierra Leone Teaching Hospitals Complex. The hospital, located in a densely populated urban area, has 164 inpatient beds and dedicated units for neonatal care, emergency, high dependency, intensive care, oncology, therapeutic feeding and general paediatrics.
Measurement and data collection procedure
Data was collected using a structured questionnaire by three trained data collectors who are medical interns with bachelor degree in medicine and surgery through face to face interview. The data collectors were responsible for the completeness and consistency of data at the site. The questionnaire comprised of four (4) sections. The first part contains questions about the socio-demographic characteristics of caregivers. The second part consisted of eight questions to assess the knowledge of the participants. The third and fourth parts consist of eight and nine questions to assess the attitude and practice of the study participants respectively. Knowledge, attitude, and practice levels were categorized based on mean scores.
Operational definition of terms
Diarrhoea: the passage of three or more loose or liquid stools per day [1].
Dehydration: the loss of water from the body, as a result of diarrhea [12]
Rehydration: The correction of dehydration with oral rehydration salts (ORS) or home prepared solution [12].
Oral Rehydration Therapy (ORT): The administration of fluid by mouth to prevent or correct the dehydration that is a consequence of diarrhea. It is a mixture of clean water, salt and sugar [12].
Good knowledge: study participant who correctly answered the mean score and above of the knowledge questions, was considered as having good knowledge [13].
Poor knowledge: study participant who correctly answered below the mean score of the knowledge questions, was considered as having poor knowledge [13].
Positive Attitude: study participant who correctly answered the mean score and above of the attitude questions, was considered as having a positive attitude [14].
Negative Attitude: study participant who correctly answered below the mean score of the attitude questions, was considered as having negative attitude [14].
Good practice: study participant who correctly answered the mean score and above of the practice questions, was considered as having good practice [15].
Poor Practice: study participant who correctly answered below the mean score of the practice questions, was considered as having poor practice [15].
Ethical considerations
Permission for the study was obtained from the management and the research committee of Ola During Children’s hospital. Written informed consent (by signature or thumbprint) was obtained from those who volunteered.
Data Analysis
Data was entered into the Statistical Package for Social Sciences (SPSS) version 25.0 for IBM electronic spreadsheet. Frequencies and percentages were used to describe descriptive data and the results were presented using tables and figure. The association between socio-demographic factors and caregivers’ knowledge, attitude and practice towards the prevention and home-based management of diarrhea, were evaluated using chi square or Fisher’s exact test as appropriate. Multivariate analysis with logistic regression was carried out, to look for independent association. The level of significance was set at p <0.05 in all the statistical analyses.
Results
A total of 110 caregivers have participated in the study with a response rate of 100%. So, 110 respondents’ data were included in the analysis process.
Socio-demographic characteristics of the caregivers
In this study, the majority of caregivers (34; 30.9%) were in the age of 25–29 years with the mean age of 27.99 [SD ± 5.2] years. Almost all caregivers were females (105; 95.5%) and 69 (62.7%) of them were Muslims. Eighty-three (75.5%) of the participants have had a formal education with 75 (68.2%) having at least secondary level of education. The majority of the caregivers 91 (82.7%) were employed and more than half of them were urban residents (Table 1). Concerning partner’s socio-demographic status, 90 (81.8%) of the caregivers reported that their partners have at least secondary level of education; 107(97.3%) of them were employed and over twothirds earn above 1000 Leones monthly income (Table 1a,b).
|
Variables |
Frequency (n=110) |
Percentage |
|
Caregiver |
||
|
Mother |
100 |
90.8 |
|
Father |
5 |
4.6 |
|
Others |
5 |
4.6 |
|
Age (years) |
||
|
<20 |
7 |
6.4 |
|
20-24 |
27 |
|
|
25-29 |
34 |
|
|
30-34 |
24 |
|
|
≥35 |
18 |
|
|
Sex |
||
|
Female |
105 |
95.5 |
|
Male |
5 |
4.5 |
|
Religion |
||
|
Muslim |
69 |
62.7 |
|
Christianity |
41 |
37.3 |
|
Tribe |
||
|
Temne |
50 |
45.5 |
|
Mende |
16 |
14.5 |
|
Limba |
13 |
11.8 |
|
Fullah |
11 |
10.0 |
|
Soso |
8 |
7.3 |
|
Madingo |
7 |
6.4 |
|
Creole |
5 |
4.5 |
|
Marital status |
||
|
Single |
25 |
22.7 |
|
Married |
85 |
77.3 |
|
Educational status |
||
|
No formal education |
27 |
24.5 |
|
Primary |
8 |
7.3 |
|
Secondary |
64 |
58.2 |
|
Tertiary |
11 |
10.0 |
|
Place of Residence |
||
|
Urban |
70 |
63.6 |
|
Rural |
40 |
36.4 |
|
Occupation |
||
|
Unemployed |
19 |
17.3 |
|
Government employee |
6 |
5.5 |
|
Private employee |
7 |
6.4 |
|
Merchant |
68 |
61.8 |
|
Student |
10 |
9.1 |
|
Monthly income (Leones) |
||
|
<500 |
35 |
31.8 |
|
500-1000 |
31 |
28.2 |
|
>1000 |
44 |
40.0 |
Table Ia: Socio-demographic characteristics of the caregivers
|
Variables |
Frequency (n=110) |
Percentage |
|
Partner’s Age (years) |
||
|
20-24 |
6 |
5.5 |
|
25-29 |
10 |
9.1 |
|
30-34 |
36 |
32.7 |
|
≥35 |
58 |
52.7 |
|
Partner’s Educational status |
||
|
No formal education |
18 |
16.4 |
|
Primary |
2 |
1.8 |
|
Secondary |
60 |
54.5 |
|
Tertiary |
30 |
27.3 |
|
Partner’s occupation |
||
|
Unemployed |
3 |
2.7 |
|
Government employee |
24 |
21.8 |
|
Private employee |
40 |
36.4 |
|
Merchant |
43 |
39.1 |
|
Partner’s Monthly income (Leones) |
||
|
<500 |
6 |
5.5 |
|
500-1000 |
16 |
14.5 |
|
>1000 |
88 |
80.5 |
Table 1b: Socio-demographic characteristics of the caregivers
Caregivers’ knowledge about diarrhea prevention and management among under-five children
More than half of the caregivers (62; 56.3%), defined diarrhea as the passing of loose stool 3 or more times per day, while, 20 (18.2) caregivers described the presence of blood in the stool as diarrhoea. Nearly all respondents (109; 99.1%) thought diarrhea to be a serious illness among children, and the use of contaminated water (94.5%), hand washing without soap before preparing food (82.7%), and use of unclean infant feeding bottles (82.7%), were the common causes of diarrhea stated.
Most caregivers knew that breastfeeding should be continued during diarrhea episodes (94; 85.5%) and agreed to the use of oral rehydration solution (ORS) to treat diarrhea (72; 65.4%); but they did not believe diarrhea can be managed at home (96; 87.3%). Weakness or lethargy (105; 95.5%) was the most identified danger sign of under-five diarrheal disease, followed by repeated vomiting (76; 69.1%) and poor feeding (76; 69.1%). Only a few respondents acknowledge the presence of reduced urine output (7; 6.4) and marked thirst for water (7; 6.4%), as danger signs for diarrhoea (Table 2).
|
Variables |
Frequency |
Percentage |
|
What do you understand by diarrhoea? |
||
|
Frequent passing of watery stool (3 or more times) |
62 |
56.3 |
|
Frequent passing of non- watery stool |
9 |
8.2 |
|
Blood in stools |
20 |
18.2 |
|
Greenish stools |
13 |
11.8 |
|
Mucus in stool |
6 |
5.5 |
|
Do you think diarrhoea is a serious child illness? |
||
|
Yes |
109 |
99.1 |
|
No |
1 |
0.9 |
|
What do you think are the causes of diarrhoea?* |
||
|
Hand washing without soap before preparing food |
91 |
82.7 |
|
Contaminated water |
104 |
94.5 |
|
Teething |
33 |
30.0 |
|
Open disposal of faeces |
82 |
74.5 |
|
Use of unclean infant feeding bottles |
91 |
82.7 |
|
Intestinal parasites |
18 |
16.4 |
|
Is it necessary to stop breastfeeding during diarrhoea episode? |
||
|
Yes |
16 |
14.5 |
|
No |
94 |
85.5 |
|
Is diarrhoea manageable at home? |
||
|
Yes |
14 |
12.7 |
|
No |
96 |
87.3 |
|
Use of Oral Rehydration Solution (ORS) |
||
|
Diarrhoea prevention |
24 |
21.8 |
|
Diarrhoea treatment |
72 |
65.4 |
|
No idea |
8 |
7.3 |
|
Others |
6 |
5.5 |
|
Diarrhoea can be prevented by:* |
||
|
Giving a child clean water |
101 |
91.8 |
|
Exclusive breastfeeding for at least 6months |
77 |
70.0 |
|
Handwashing with soap before meal preparation |
100 |
90.9 |
|
Vitamin A supplementation |
6 |
5.5 |
|
Vaccination (Measles and Rota) |
24 |
21.8 |
|
Improved water supply and sanitation |
101 |
91.8 |
|
Praying |
4 |
3.6 |
|
Danger signs of diarrhea* |
||
|
Becoming weak or lethargic |
105 |
95.5 |
|
Frequent passing of diarrhea |
58 |
52.7 |
|
Repeated vomiting |
76 |
69.1 |
|
Fever and blood in stool |
70 |
63.6 |
|
Marked thirst for water |
7 |
6.4 |
|
Poor feeding |
76 |
69.1 |
|
Reduced urine output |
7 |
6.4 |
Table 2 : Caregivers’ knowledge about diarrhea prevention and management among under-five children *Multiple responses were allowed.
Caregivers’ attitudes toward prevention and home-based management of under-five diarrhea
A total of 107 (97.3%) respondents acknowledged that diarrhoea is a serious disease that can lead to death, 83 (75.5%) agreed that infants who are bottle fed are more likely to contract diarrhoea than infants who are directly breastfed, 105 (95.5%) agreed that it is important to handwash before preparing meals for their children, while 82 (74.6%) agreed that exclusive breastfeeding for at least the first 6 months of life is important in preventing diarrhoea. The majority (93; 84.6) agreed that oral rehydration fluids can be prepared at home, while 85 (77.3%) agreed that giving oral rehydration treatment is necessary during diarrhoea. More than half (56; 50.8%) were unsure about the importance of vaccination for diarrhoea prevention; 94 (85.5%) rightly disagreed to the statement; open disposal of faeces does not affect the occurrence of diarrhoea (Table 3).
|
Variables |
SA n(%) |
A n(%) |
Un n(%) |
D n(%) |
SD n(%) |
|
Diarrhoea is a serious disease and can lead to death |
103(93.7) |
4(3.6) |
2(1.8) |
1(0.9) |
0(0.0) |
|
Infants who are bottle fed are more likely to contract diarrhoea than infants who are directly breastfed |
39(35.5) |
44(40.0) |
19(17.3) |
5(4.5) |
3(2.7) |
|
It is important to handwash with water and soap before preparing meals for your child |
84(76.4) |
21(19.1) |
3(2.7) |
1(0.9) |
1(0.9) |
|
Exclusive breastfeeding for at least the first 6 months of life is important in preventing diarrhoea |
43(39.1) |
39(35.5) |
23(20.9) |
2(1.8) |
3(2.7) |
|
Oral rehydration fluid can be prepared at home |
33(30.1) |
60(54.5) |
12(10.9) |
4(3.6) |
1(0.9) |
|
Giving oral rehydration is necessary during diarrhoea |
41(37.3) |
44(40.0) |
18(16.4) |
5(4.5) |
2(1.8) |
|
Vaccination is not necessary for preventing diarrhea |
6(5.5) |
8(7.3) |
56(50.8) |
17(15.5) |
23(20.9) |
|
Open disposal of faeces does not affect the occurrence of diarrhea |
5(4.5) |
3(2.7) |
8(7.3) |
23(20.9) |
71(64.6) |
Table 3: Caregivers’ attitudes toward prevention and home-based management of under-five diarrhea; SA, Strongly agree; A, Agree; Un, Undecided; D, Disagree; SD, Strongly disagree.
Practices of caregivers towards the prevention and home management of diarrhea among under-five children
From the total respondents, the majority (62; 56.4%) practised exclusive breastfeeding. Although there was no special place for hand washing in their houses (91; 82.7%), most caregivers (87; 79.1%) still washed their hands with water and soap, especially after attending to their child who had defecated (103; 93.6). Less than half 25 (22.7%) disposed their child’s faeces in the toilet, 72 (65.5%) disposed child’s faeces in the dustbin outside their houses, while 13 (11.8%) simply rinsed faeces into the gutter while washing (Table 4).
Most of the caregivers (69; 62.7%) sought help from healthcare providers during the time of diarrheal diseases, which informed the common use of ORS (92; 83.6%); and about a quarter (31; 28.2%) prepared salt and sugar solution (ORT) at home when ORS was unavailable. Additional treatment given to their children during diarrhea illness was mostly Zinc tablets (76; 69.1%) (Table 4).
|
Variables |
Frequency |
Percentage |
|
Duration of breastfeeding? |
||
|
Less than six months |
48 |
43.6 |
|
Six months or more |
62 |
56.4 |
|
Does your house have a special place for hand washing? |
||
|
Yes |
19 |
17.3 |
|
No |
91 |
82.7 |
|
When is hand washing practiced?* |
||
|
Before food preparation |
88 |
80.0 |
|
Before feeding children |
95 |
86.4 |
|
After defecation |
84 |
76.4 |
|
After attending to child who has defecated |
103 |
93.6 |
|
What do you wash your hands with? |
||
|
Water |
14 |
12.7 |
|
Water and ash |
9 |
8.2 |
|
Water and soap |
87 |
79.1 |
|
Where do you dispose your child’s faeces? |
||
|
Toilet |
25 |
22.7 |
|
Dust bin |
72 |
65.5 |
|
Rinsed into gutter |
13 |
11.8 |
|
Help sought during diarrhoea episode was from:* |
||
|
Friends/Neighbours/Relatives |
30 |
27.0 |
|
Healthcare provider |
69 |
62.7 |
|
Read instructions |
15 |
13.5 |
|
Others |
5 |
4.5 |
|
Used ORS during diarrhoea episode |
||
|
Yes |
92 |
83.6 |
|
No |
18 |
16.4 |
|
Prepared salt and sugar solution (ORT) at home when ORS was unavailable |
||
|
Yes |
31 |
28.2 |
|
No |
79 |
71.8 |
|
Other treatment given during diarrhoea episode:* |
||
|
Zinc |
76 |
69.1 |
|
Vitamin A |
6 |
5.5 |
|
Traditional medicine |
41 |
37.3 |
Table 4: Practices of caregivers towards the prevention and home management of diarrhoea among under-five children; *Multiple responses were allowed.
The overall level of knowledge, attitude, and practice of caregivers in the prevention and home-based management of diarrhea among under-five children
Overall, 81 (73.6%) caregivers had good knowledge about the prevention and home-based management of under-5 diarrheal diseases, while 29 (26.4%) had poor knowledge (Figure 1). The majority had a positive attitude (89; 80.9) and a similar proportion demonstrated good care practices (93; 84.5%).
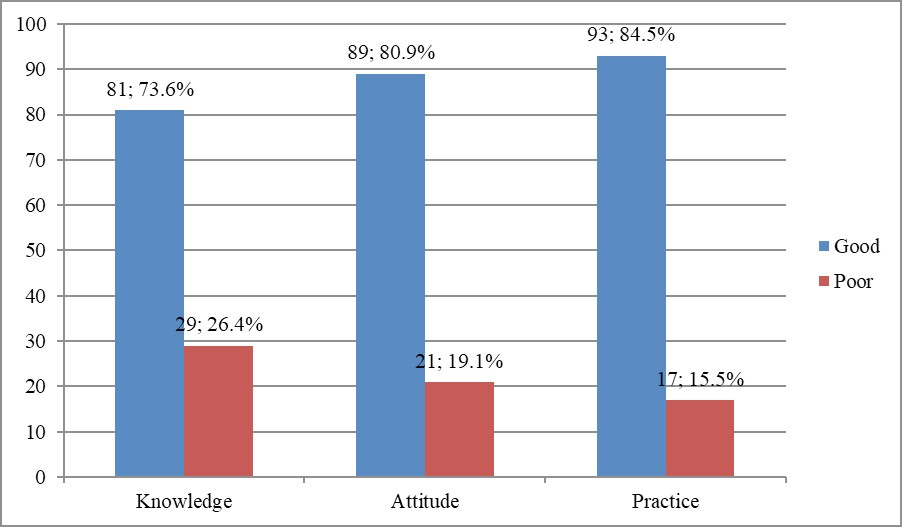
Figure 1: The overall level of knowledge, attitude, and practice of caregivers in prevention and home-based management of diarrhea among under-five children.
Factors Associated with Knowledge, Attitude, and Practice towards Diarrhoea Prevention and Home-based Management
Younger age, lower educational status and residence within rural settings, were consistently among the socio-economic factors of caregivers, which were significantly associated with poorer knowledge, attitude and practice regarding the prevention and home-based management of under-5 diarrheal diseases. Other socio-demographic characteristics that demonstrated variable levels of significant were monthly income and occupation of caregivers, as well as the age and educational status of their partners (Table 5).
|
Variable |
Knowledge |
Attitude |
Practice |
||||||
|
Good |
Poor |
p |
Positive |
Negative |
p |
Good |
Poor |
p |
|
|
Age (years) |
|||||||||
|
<20 |
3 |
4 |
0.041 |
2 |
5 |
<0.001 |
3 |
4 |
0.001 |
|
20-24 |
17 |
10 |
18 |
9 |
19 |
8 |
|||
|
25-29 |
27 |
7 |
30 |
4 |
32 |
2 |
|||
|
30-34 |
20 |
4 |
22 |
2 |
23 |
1 |
|||
|
≥35 |
14 |
4 |
17 |
1 |
16 |
2 |
|||
|
Sex |
|||||||||
|
Male |
3 |
2 |
0.479 |
3 |
2 |
0.223 |
3 |
2 |
0.120 |
|
Female |
78 |
27 |
86 |
19 |
90 |
15 |
|||
|
Religion |
|||||||||
|
Christianity |
29 |
12 |
0.594 |
34 |
7 |
0.678 |
33 |
8 |
0.364 |
|
Muslim |
52 |
17 |
55 |
14 |
60 |
9 |
|||
|
Tribe |
|||||||||
|
Temne |
36 |
14 |
0.946 |
41 |
9 |
0.738 |
44 |
6 |
0.454 |
|
Mende |
13 |
16 |
13 |
3 |
15 |
1 |
|||
|
Limba |
9 |
13 |
12 |
1 |
11 |
2 |
|||
|
Fullah |
8 |
3 |
7 |
4 |
8 |
3 |
|||
|
Soso |
6 |
8 |
6 |
2 |
5 |
3 |
|||
|
Madingo |
6 |
1 |
6 |
1 |
6 |
1 |
|||
|
Creole |
3 |
2 |
4 |
1 |
4 |
1 |
|||
|
Marital status |
|||||||||
|
Married |
62 |
23 |
0.093 |
71 |
14 |
0.197 |
74 |
11 |
0.179 |
|
Single |
19 |
6 |
18 |
7 |
19 |
6 |
|||
|
Educational status |
|||||||||
|
No formal education |
12 |
15 |
<0.001 |
16 |
11 |
<0.001 |
17 |
10 |
<0.001 |
|
Primary |
1 |
7 |
3 |
5 |
4 |
4 |
|||
|
Secondary |
57 |
7 |
59 |
5 |
61 |
3 |
|||
|
Tertiary |
11 |
0 |
11 |
0 |
11 |
0 |
|||
|
Residence |
|||||||||
|
Urban |
65 |
5 |
<0.001 |
67 |
22 |
<0.001 |
68 |
2 |
<0.001 |
|
Rural |
16 |
24 |
3 |
18 |
25 |
15 |
|||
|
Occupation |
|||||||||
|
Unemployed |
11 |
8 |
0.257 |
12 |
7 |
0.031 |
12 |
7 |
0.017 |
|
Government |
6 |
0 |
6 |
0 |
6 |
0 |
|||
|
Private |
6 |
1 |
7 |
0 |
7 |
0 |
|||
|
Merchant |
50 |
18 |
58 |
10 |
61 |
7 |
|||
|
Student |
8 |
2 |
6 |
4 |
7 |
3 |
|||
|
Income (Le) |
|||||||||
|
<500 |
23 |
12 |
0.381 |
24 |
11 |
0.043 |
25 |
10 |
0.029 |
|
500-1000 |
23 |
8 |
25 |
6 |
29 |
2 |
|||
|
>1000 |
35 |
9 |
40 |
4 |
39 |
5 |
|||
|
Partner’s age (years) |
|||||||||
|
20-24 |
4 |
2 |
0.731 |
4 |
2 |
0.127 |
4 |
2 |
0.042 |
|
25-29 |
6 |
4 |
6 |
4 |
6 |
4 |
|||
|
30-34 |
27 |
9 |
28 |
8 |
30 |
6 |
|||
|
≥35 |
44 |
14 |
51 |
7 |
53 |
5 |
|||
|
Partner’s educational status |
|||||||||
|
No formal education |
12 |
6 |
0.014 |
14 |
4 |
0.360 |
14 |
4 |
0.369 |
|
Primary |
0 |
2 |
1 |
1 |
2 |
0 |
|||
|
Secondary |
42 |
18 |
47 |
13 |
49 |
11 |
|||
|
Tertiary |
27 |
3 |
27 |
3 |
28 |
2 |
|||
|
Partner’s occupation |
|||||||||
|
Unemployed |
2 |
1 |
0.660 |
2 |
1 |
0.441 |
2 |
1 |
0.292 |
|
Government |
20 |
4 |
22 |
2 |
23 |
1 |
|||
|
Private |
29 |
11 |
32 |
8 |
32 |
8 |
|||
|
Merchant |
30 |
13 |
33 |
10 |
36 |
7 |
|||
|
Partner’s income (Le) |
|||||||||
|
<500 |
4 |
2 |
0.198 |
4 |
2 |
0.500 |
5 |
1 |
0.510 |
|
500-1000 |
9 |
7 |
12 |
4 |
12 |
4 |
|||
|
>1000 |
68 |
20 |
73 |
15 |
76 |
12 |
Table 5: Factors Associated with Knowledge, Attitude, and Practice towards Diarrhoea Prevention and Home-based Management; Le = Leones
Multivariate Analysis
In multivariate analysis, caregivers who resided in urban areas and had more than six years of education, were more likely to have good knowledge [(OR= 4.365, p = <0.001) and (OR = 2.133, p = 0.006) respectively], positive attitude [(OR= 2.735, p = 0.007) and (OR = 2.535, p = 0.013) respectively] and good practices [(OR= 2.383, p = 0.019) and (OR = 3.153, p = 0.002) respectively] about the prevention and home-based management of under-5 diarrheal diseases, as compared to those who resided among rural communities and had acquired six years of education or less.
Older caregiver were 3.0 times more likely to have positive attitude towards diarrhea prevention and home-based management, than younger caregivers were (OR = 3.092, p = 0.003).
Respondents who were employed and had older partners, [(OR= 2.070, p = 0.041) and (OR = 2.029, p = 0.045)] respectively, were more likely to have good practice towards diarrhoea prevention and home-based management, than caregivers who were unemployed or had younger partners (Table 6).
|
Variables |
Good |
Knowledge |
Positive |
Attitude |
Good |
Practice |
|||
|
Odds Ratio |
95% CI |
p |
Odds Ratio |
95% CI |
p |
Odds Ratio |
95% CI |
p |
|
|
Age |
0.039 |
0.099-1.021 |
0.196 |
3.092 |
1.152-9.031 |
0.003 |
1.043 |
0.105-1.019 |
0.169 |
|
Residence |
4.365 |
1.186-5.545 |
<0.001 |
2.735 |
3.063-12.394 |
0.007 |
2.383 |
1.031-9.341 |
0.019 |
|
Educational status |
2.133 |
2.227-8.040 |
0.006 |
2.535 |
2.191-7.023 |
0.013 |
3.153 |
2.201-10.046 |
0.002 |
|
Occupation |
0.518 |
0.089-4.052 |
0.606 |
1.224 |
0.086-1.020 |
0.224 |
2.070 |
4.103-13.002 |
0.041 |
|
Income |
1.073 |
0.048-1.600 |
0.286 |
0.467 |
0.103-4.064 |
0.641 |
0.133 |
0.072-0.082 |
0.894 |
|
Partner’s Age |
0.471 |
0.128-2.079 |
0.639 |
2.376 |
0.017-1.189 |
0.190 |
2.029 |
0.002-0.154 |
0.045 |
|
Partner’s educational status |
0.030 |
0.048-2.108 |
0.446 |
1.328 |
0.025-2.126 |
0.187 |
1.294 |
0.024-1.117 |
0.198 |
Table 6: Multivariate Analysis.
Discussion
This study evaluated caregivers’ knowledge, attitudes, and practices (KAP) regarding the prevention and home-based management of diarrhoeal diseases among children under five, at a tertiary paediatric hospital in Freetown, Sierra Leone. The findings revealed that the majority of participants demonstrated good knowledge (73.6%), positive attitudes (80.9%), and appropriate practices (84.5%) toward diarrhoea prevention and management at home
The high level of knowledge observed among caregivers aligns with findings from similar studies in Nigeria-59.2% [14]. and Ethiopia 65.2% [15], indicating growing awareness of diarrhoea management among caregivers in sub-Saharan Africa. However, lower knowledge levels have been reported in other regions of Ethiopia 37.5% [16] and in Iran-28.8% [17]. Such variations may be attributed to methodological differences, socio-cultural and educational disparities, differences in healthcare access, and exposure to public health interventions. The urban setting of Freetown likely contributed to the higher awareness observed in this study, as caregivers in urban areas often have better access to healthcare facilities and health information. Most caregivers accurately defined diarrhoea as the passage of three or more loose or watery stools per day and correctly identified common causes, including poor hygiene and contaminated water. These results are consistent with previous studies [18- 20,16]. However, a substantial proportion of caregivers did not recognise that diarrhoea can be effectively managed at home. This misconception likely account for the limited experience in preparing home-based rehydration solutions when commercial oral rehydration salts (ORS) were unavailable, a finding also reported in other studies [15,14].
Hand hygiene remains a key preventive measure against diarrhoeal diseases. Evidence suggests that washing hands with soap— particularly after defecation, after cleaning a child, and before food preparation—significantly reduces the risk of diarrhoea [21]. Handwashing with water alone is considerably less effective because soap helps remove pathogens by breaking down grease and dirt and encourages longer washing duration [22]. In the present study, nearly all respondents (95.5%) recognised the importance of using soap during handwashing, and this was reflected in their reported practices. These findings are comparable to studies from Nigeria [14], Sudan [23], and India [24], though they contrast with lower rates of proper handwashing practices reported in Ethiopia [16] and Bangladesh [25]. The strong hygiene practices observed here may be linked to caregivers’ proactive health-seeking behaviors and regular interaction with healthcare providers.
Exclusive breastfeeding (EBF) is defined as the practice of feeding an infant only breast milk, without the introduction of any other foods or liquids, for the first six months of life. However, the definition permits the administration of oral rehydration solution (ORS), as well as vitamins, minerals, and medicinal drops or syrup [26]. According to Bryce et al, infants who are not exclusively breastfed have a sevenfold higher risk of mortality from common childhood illnesses, such as diarrhoea, compared with those who are exclusively breastfed [27]. This increased risk is attributed to the nutritional inadequacy of breast milk substitutes and their potential for contamination, which predisposes infants to diarrhoea diseases.
In the present study, more than half of the respondents (62; 56.4%) practiced exclusive breastfeeding, a finding consistent with previous studies conducted in India [24] and Sierra Leone [28], which reported EBF rates of 56% and 66% respectively. In contrast, a considerably lower rate of 2% was reported in a study conducted in a rural community in Nigeria [29]. Possible explanations for the low EBF rates observed includes prevalent misconceptions regarding the sufficiency of breast milk to meet infants’ nutritional requirements and limited access to accurate health information on the benefits and practices of exclusive breastfeeding.Sociodemographic factors such as younger age, lower educational attainment, unemployment, and rural residence were significantly associated with poorer KAP outcomes. These associations mirror findings from other studies [30,14]. Women’s health literacy and educational level play a crucial role in shaping family health behaviors [31]. Educated mothers are more likely to recognize disease symptoms early, implement preventive measures, and adopt effective home management strategies. As women are the primary caregivers in Sierra Leone, enhancing female education and empowerment remains essential to improving child health outcomes and reducing diarrhoea-related morbidity and mortality.
Conclusion
Caregivers demonstrated good overall knowledge, attitudes, and practices regarding diarrhoea management. Nonetheless, gaps remain in understanding home-based care and alternative ORS preparation. Targeted community-based health education is recommended to strengthen caregiver capacity, especially in rural settings.
Limitations
As a hospital-based study, findings may not be generalizable to community populations. Future research should include householdlevel assessments to better understand community practices.
Acknowledgments
The authors acknowledge our research assistants and all staff of the general paediatric wards, Ola During Children’s Hospital for the invaluable support during data collection. We are also grateful to the management of Ola During Children’s Hospital.
Funding
There was no special funding for the study.
Disclosure
The authors declare that they have no competing interests for this work.
References
- Olopha OO, Egbewale B (2017) Awareness and knowledge of diarrhoeal home management among mothers of under-five in Ibadan Nigeria Univ J Public Health 5:40-45.
- Motarjemi Y, Kaferstein F, Moy G, Quevedo F (1993). Contaminated weaning food: a major risk factor for diarrhoea and associated malnutrition. Bull World Health Organ 71: 79-92.
- Seifu BL, Legesse BT, Yehuala TZ, Kase BF, Asmare ZA, et al. (2014). Factors associated with the co-utilisation of oral rehydration solution and zinc for treating diarrhoea among under-five children in 35 subSaharan Africa countries: a generalised linear mixed effect modeling with robust error variance. BMC Public Health.24: 1329.
- Wardlaw T, Salama P, Brocklehurst C, Chopra M, Mason E (2010) Diarrhoea: why children are still dying and what can be done. Lancet 375: 870-872.
- Walker CLF, Aryee MJ, Boschi-Pinto C, Black RE (2012) Estimating diarrhea mortality among young children in low and middle income countries. PLoS One 7: e29151.
- World Health Organisation (2017) Diarrhoeal disease.
- World Health Organisation (2021). Global health estimates: Leading causes of death.
- Moore SR, Lima NL, Soares AM, Oriá RB, Pinkerton RC, et al. (2010) Prolonged episodes of acute diarrhoea reduce growth and increase the risk of persistent diarrhoea in children. Gastroenterology139: 1156-1164.
- Troeger C, Colombara DV, Rao PC, Khalil IA, Brown A, et al. (2018) Global disability-adjusted life-year estimates of long-term health burden and undernutrition attributable to diarrhoeal diseases in children younger than five years. Lancet Glob Health 6 :e255-269.
- Patwari AK (1999) Diarrhoea and malnutrition interaction. Indian J Pediatr 66: S124–S134.
- Munos MK, Walker CL, Black RE (2010) The effect of oral rehydration solution and recommended home fluids on diarrhoea mortality. Int J Epidemiol39: i75-87.
- World Health Organisation (2017). Diarrhoeal disease.
- UNICEF DATA (2018). Diarrhoea.
- Momoh FE, Olufela OE, Adejimi AA, Roberts AA, Oluwole ES, et al. (2022) Mothers’ knowledge, attitude and home management of diarrhoea among children under five years old in Lagos, Nigeria. Afr J Prm Health Care Fam Med 14: a3119.
- Workie HM, Sharifabdilahi AS, Addis EM (2018) Mothers’ knowledge, attitude and practice towards the prevention and home-based management of diarrheal disease among under-five children in Diredawa, Eastern Ethiopia, 2016: a cross-sectional study. BMC Pediatrics. 18: 358.
- Merga N, Alemayehu T (2015) Knowledge, perception, and management skills of mothers with under-five children about diarrhoeal disease in indigenous and resettlement communities in Assosa District, Western Ethiopia. J Health Popul Nutr33: 20-30.
- Ghasemi AA, Talebian A, Masoudi Alavi N, Moosavi G (2013) Knowledge of mothers in management of diarrhea in under-five children, in Kashan, Iran. Nurs Midwifery Stud 1: 158-162.
- Ellis AA, Winch P, Daou Z, Gilroy KE, Swedberg E (2007) Home management of childhood diarrhoea in southern Mali--implications for the introduction of zinc treatment. Soc Sci Med 64: 701-712.
- Saurabh S, Shidam UG, Sinnakirouchenan M, Subair M, Hou LG, (2014). Knowledge and practice regarding oral rehydration therapy for acute diarrhoea among mothers of under-five children in an urban area of Puducherry India. Natl J Community Med 5:100-104.
- Mumtaz Y, Zafar M, Mumtaz Z (2014) Knowledge attitude and practices of mothers about diarrhea in children under 5 years. J Dow Uni Health Sci 8: 3-6.
- Olubunmi OO, Bolaji E (2017) Awareness and knowledge of diarrhoeal home management among mothers of underfive in Ibadan, Nigeria. Univers J Public Health.5: 40-45.
- UNICEF (2010) Launch of hand washing campaign in Abuja.
- Panom PDK, Ying-Chun D (2018) Mothers knowledge attitude and practice on preventing diarrhoea in Juba, South Sudan. S Sudan Med J 11: 60-64.
- Suganya V, Bibitha B, Revathi D, Ramya K, Indira S, (2017) Knowledge on home management of diarrhoea among mothers of under five children. Int J Appl Res 3: 376-380.
- Rabbi SE, Dey NC (2013). Exploring the gap between hand washing knowledge and practices in Bangladesh: a cross-sectional comparative study. BMC Public Health.13:89.
- UNICEF (2018) National Nutrition and Health Survey (NNHS). Report on the Nutrition and Health Situation of Nigeria.
- Bryce J, Arifeen S el, Pariyo G, Lanata CF, Gwatkin D, et al. (2003) Reducing child mortality: can public health deliver? Lancet 362: 159164.
- Bell NVT, Ikhurionan PE, Akhigbe IE, Mustapha AM, Ofovwe GE (2022) Knowledge, Attitude and Practices of Breastfeeding among mothers of children six months to three years seen at a tertiary children hospital in Freetown. Niger J Paediatr 49 : 109 -116.
- Ogbeyi GO, Onyemocho A, Ogbonna C (2016) Assessment of caregivers knowledge of diarrhoea and practice of home management of diarrhoea disease among under two children in Opialu, a rural community in Benue State, Nigeria. Glob J Med Public Health 5: 3-13.
- Bogale KD, Nega TA, Tesfaye DA (2017) Knowledge, practice, and associated factors of home-based management of diarrhea among caregivers of children attending under-five clinic in Fagita Lekoma District, Awi Zone, Amhara Regional State, Northwest Ethiopia. Nurs Res Pract 91: 555-562.
- Lee SD, Tsai T, Tsai Y, Kuo KN (2012) Health literacy and women’s health-related behaviors in Taiwan. Health Educ Behav 39: 210-218.
- World Health Organization (2013) Diarrhoeal disease Fact sheet.
- Desta BK, Assimamaw NT, Ashenafi TD (2016) Knowledge, practice, and associated factors of home-based Management of Diarrhea among caregivers of children attending under-five Clinic in Fagita Lekoma District, Awi zone, Amhara regional state, Northwest Ethiopia,Nurs Res Pract 2017: 8084548.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.