Knowledge, Attitudes, Practices, and Certification Gaps among Travel Medicine Practitioners in Nigeria
by Olatunde OA1-3*, Iliodiba NN4, Alao AO5, Alawode OA6, Kajero AO7, Ibisola BA8, Nebe JN9, Oliyide OT3, Bakare OH3, Ayoola BT3
1Department of Family Medicine, Dalhousie University, Halifax, Canada
2Department of Family Medicine, UBC, Vancouver, Canada
3Society for Good Health, Sustainable Development and Environmental Awareness, Nigeria
4Nigerian Society of Travel Medicine, Lagos, Nigeria
5Lagoon Hospitals, Ikoyi, Lagos, Nigeria
6University College Hospital, Ibadan, Nigeria
7University of Lagos, Lagos, Nigeria
8Triverge Geriatrics Centre, Lagos, Nigeria
9Family Medicine Department, Lagos State University Teaching Hospital, Lagos, Nigeria
*Corresponding author: Olatunde OA, Department of Family Medicine, Dalhousie University, Halifax, Canada
Received Date: 06 April, 2026
Accepted Date: 17 April, 2026
Published Date: 22 April, 2026
Citation: Olatunde OA, Iliodiba NN, Alao AO, Alawode OA, Kajero AO, et al. (2026) Knowledge, Attitudes, Practices, and Certification Gaps among Travel Medicine Practitioners in Nigeria. J Community Med Public Health 10: 568. DOI: https://doi.org/10.29011/2577-2228.100568
Abstract
Background: International mobility exposes travellers to diverse health risks, including infectious diseases and psychological stressors, thereby necessitating the evolving field of travel medicine. In Nigeria, where emigration remains comparatively high, understanding practitioner readiness is both timely and policy relevant. Objectives: This study assessed the knowledge, attitudes, and practices of travel medicine practitioners in Nigeria. Methods: A cross-sectional survey of 89 medical practitioners was conducted using a semi-structured online questionnaire distributed via WhatsApp and email. Participants were recruited through convenience sampling, with prior ethical approval and informed consent obtained. Data were analysed using the R programming language. Results: The average age of the participants was 43.8 ± 8.43 years (mean ± standard deviation), with a preponderance of females (52.8%), and practicing traveling medicine for less than 5 years (50.6%). Although the study revealed that a preponderance of the participants (94.4%) did not have travel medicine certification. It was observed that 61.8% demonstrated excellent knowledge of key areas of travel medicine, a high positive attitude (94.4%), and high-quality practice (67.4%). Knowledge (B = 0.389, p = 0.045 and attitude (B = 0.645, p = 0.020) are significant predictors of high-quality practice. Conclusion: Practitioners showed strong knowledge and practice despite low certification, underscoring the need for structured training and certification to standardise and enhance travel medicine practice in Nigeria.
Keywords: Travel medicine; International travel health; Knowledge; Attitudes; Practices; Medical practitioners; Nigeria; Healthcare training; Certification; Logistic regression
Background
Travel medicine, as an interdisciplinary field encompassing preventive health, epidemiology, and infectious diseases, has gained prominence amid the surge in global mobility [1-3]. In Nigeria, a nation characterised by its vibrant economy and diverse population, international travel has escalated dramatically over the past decade, driven by business opportunities, educational pursuits, and pilgrimage activities [4]. Yet, as we delved into this area as researchers without prior expertise in tropical medicine, we were struck by the fragmented nature of travel health services here. Drawing on existing literature, it is evident that while Nigeria serves as a hub for outbound and inbound travellers, particularly to and from regions prone to endemic diseases such as yellow fever and malaria, the infrastructure for specialised travel medicine remains underdeveloped. This backdrop not only underscores the vulnerability of travellers but also prompts a critical reflection on how systemic gaps might exacerbate health risks, especially in a country grappling with resource constraints and uneven healthcare distribution.
Reflecting on the historical context, travel medicine in Nigeria has evolved sporadically, often reactive to outbreaks rather than proactive in prevention [5,6]. Early practices were largely confined to mandatory vaccinations, such as yellow fever immunisation, enforced at ports of entry under international health regulations [6]. Studies highlight that pre-travel consultations are infrequent among Nigerian travellers, with many relying on informal advice from peers or self-medication rather than professional guidance [7,8]. For instance, a cross-sectional survey at a major Nigerian airport found suboptimal compliance with travel vaccines, with only a minority of participants demonstrating comprehensive knowledge of risks such as cholera or plague [2,9]. This pattern, observed across sub-Saharan Africa, raises poignant questions about equity: why do travellers from lower socio-economic strata, who often embark on high-risk journeys for work or family, bear the brunt of inadequate preparation? As we pondered this, it seemed clear that the absence of widespread awareness campaigns contributes to a cycle of preventable illnesses, echoing broader challenges in public health education within the region.
Turning to the practitioners themselves, the landscape of travel medicine delivery in Nigeria appears marked by inconsistencies. Healthcare providers, primarily general physicians in primary care settings, are often the first point of contact for travel-related advice, yet evidence suggests varying levels of knowledge [10-12]. A recent study among Nigerian medical doctors indicated that while attitudes towards travel medicine were generally positive, knowledge gaps persisted, particularly in advising on region-specific risks such as meningococcal disease in the African meningitis belt [7,13]. Critically, this reflects a broader African context in which primary care physicians often exhibit suboptimal expertise in travel health due to limited training opportunities [12]. In a nation like Nigeria, where infectious diseases remain endemic, practitioners' practices might inadvertently mirror the travellers' own complacency, perpetuating a vulnerability that demands urgent introspection and reform.
Certification gaps further compound these issues, highlighting a structural deficit in professional development. Unlike in developed nations, where travel medicine specialists hold recognised credentials, such as those from the International Society of Travel Medicine, Nigeria lacks a robust framework for specialised certification [7, 14]. The emergence of the Nigerian Society of Travel Medicine offers promise, with certifications like the Certified Travel Medicine Practitioner of Nigeria (CTMPN), but uptake remains low, leaving many practitioners without formal accreditation [15,16]. This disparity not only affects the quality of advice, such as accurate malaria prophylaxis recommendations, but also erodes trust in healthcare systems. As researchers navigating this terrain, we found ourselves questioning whether these gaps stem from policy oversights or from resource-allocation priorities, especially when compared to the enforcement of mandatory yellow fever certification at borders. Such reflections underscore the need for targeted interventions to bridge these divides, ensuring that travel medicine evolves from a peripheral service to a cornerstone of preventive care.
In this context, the purpose of the present study is to address these observed deficiencies. Nigeria's position as a gateway to West Africa, coupled with rising outbound travel estimated at millions annually [17], amplifies the urgency of evaluating how well-equipped practitioners are to safeguard public health. Amidst global calls for strengthened health security post-pandemic, this research seeks to illuminate the interplay between knowledge, attitudes, and practices, while identifying certification issues that hinder effective service delivery. By doing so, it aims to contribute to evidence-based strategies that could enhance travel medicine standards, ultimately reducing the burden of travel-associated illnesses in a resource-limited setting.
Methods
This study adopted a cross-sectional design to capture a snapshot of the knowledge, attitudes, practices, and certification status among travel medicine practitioners in Nigeria at a single point in time. This design offered a practical and timely way to illuminate current realities in a field where systematic data remains scarce. The sample comprised 89 medical practitioners actively engaged in travel medicine across various parts of Nigeria. Participants were recruited through convenience sampling, a nonprobability approach that is pragmatic given the dispersed and relatively small population of such practitioners. This technique enabled access to willing respondents via professional networks, reflecting the real-world challenges of reaching specialised healthcare providers in a resource-constrained setting. Data were collected using an online semi-structured questionnaire, distributed through WhatsApp and email platforms. The instrument was designed to elicit both quantitative responses and nuanced insights into participants’ experiences. The digital mode proved particularly suitable amid Nigeria’s growing internet penetration among health professionals, though it inevitably excluded those with limited online access. All data were analysed using the R Programming Language. Descriptive statistics (means, standard deviations, frequencies, and percentages) summarised demographic variables and key outcome measures, while linear regression was employed for inferential analysis to identify significant predictors of high-quality practice. Ethical considerations were paramount throughout. Ethical approval was obtained from the Oyo State Health Research Ethics Review Committee. Participants provided informed consent after reading a clear explanation of the study and their rights, including voluntary participation and withdrawal.
Results
The scores for knowledge, attitude, and practice were grouped into three levels: low, average, and high. The results show that 94.4 percent of the participants (doctors) have an excellent attitude toward travel medicine, 4.5 percent have an average attitude, and 1.1 percent have a low attitude. The result also shows that 61.8 percent of the doctors scored high in travel medicine knowledge, 31.5 percent scored average, and only 6.7 percent scored low. In terms of practice, 67.4 percent of doctors scored high, 22.5 percent scored average, and 10.1 percent scored low (Figure 1).
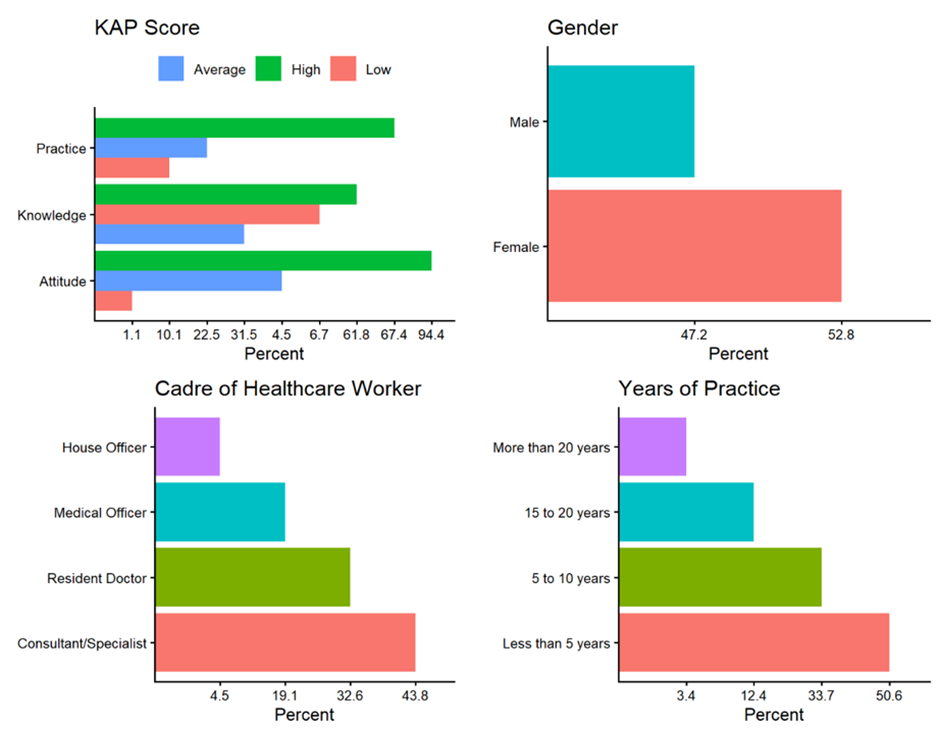
Figure 1: Summary of Demographic Variables and KAP Score.
Regarding demographics, female participants accounted for 52.8 percent, while males accounted for 47.2 percent. 43.8 percent of the respondents were consultants/specialists, resident doctors formed 32.6 percent of the respondents, medical officers formed 19.1 percent, and house officers were 4.5 percent. Regarding the years of practice in travel medicine, 50.6 percent had less than five years of experience, 33.7 percent had 5 to 10 years of experience, 12.4 percent had 15 to 20 years of experience, and 3.4 percent had more than 20 years of experience. The age distribution shows that 72.9 percent of respondents were between 30 and 49 years old, 24.7 percent were 50 years and older, and 2.4 percent were under 30 years old. 5.6 percent of the respondents had travel medicine certification, while 94.4 percent had no travel medicine certification (Table 1).
|
Term |
Estimate |
Std error |
Statistic |
p-value |
|
(Intercept) |
-2.39789 |
7.691121 |
-0.31177 |
0.756045 |
|
Age |
0.165497 |
0.085777 |
1.929395 |
0.057319 |
|
Knowledge |
0.38763 |
0.189948 |
2.040718 |
0.044662 |
|
Attitude |
0.644808 |
0.271549 |
2.374557 |
0.020028 |
|
Workers Cadre |
||||
|
Consultant/Specialist (reference) |
||||
|
House Officer |
9.387533 |
3.445544 |
2.724543 |
0.007945 |
|
Medical Officer |
2.398164 |
1.886283 |
1.27137 |
0.207375 |
|
Resident Doctor |
-0.81154 |
1.602516 |
-0.50641 |
0.613994 |
|
R-squared = 0.2159, Adjusted R-squared = 0.1556, F-statistic = 3.58, p-value = 0.003476 |
||||
Table 1: Regression Analysis of the effect of demographic variables, knowledge, and attitude on the practice of travel medicine.
Conversely, inferential analysis using linear regression statistics revealed that the model is statistically significant (F (6, 78) = 3.58, p = 0.003), indicating that the set of predictors collectively explains a meaningful portion of the variance in practice scores. However, the model explains only 21.6% of the variance in practice scores (R2 = 0.216), and the adjusted R2 of 0.156 suggests moderate explanatory power after adjusting for the number of predictors. A substantial portion of variance remains unexplained by the variables included in the model (Figure 2).
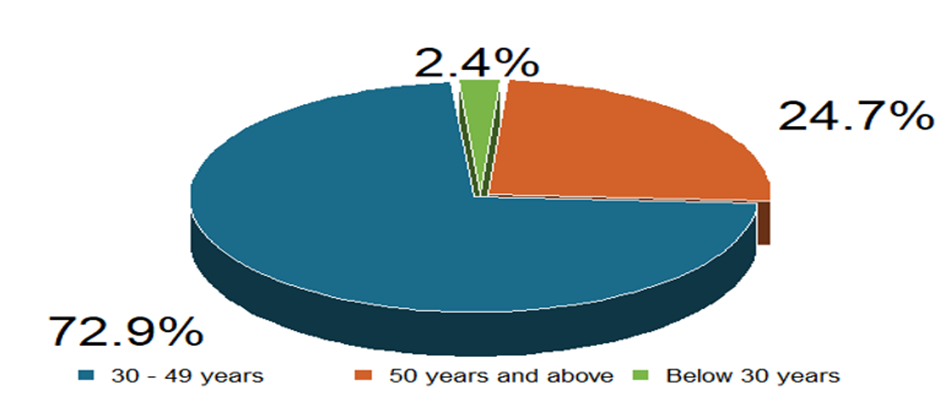
Figure 2: Summary of the Age Group of the Respondents.
The knowledge score estimate shows that for every one-unit increase in knowledge score, the practice score increases by 0.39 unit (β = 0.388, p = 0.044), holding other variables constant. This shows that there is a statistically significant positive relationship between knowledge and practice. The result also shows that for every one-unit increase in attitude score, the practice score increases by 0.645 (β = 0.645, p = 0.020). Attitude has the strongest and most significant effect among the continuous predictors, suggesting that a favourable attitude is a more potent driver of better practice than knowledge alone. The relationship between age and the practice of travel medicine is not statistically significant (β = 0.165, p = 0.057). The regression coefficient of 9.388 for house officers implies that, relative to Consultants/Specialists, House Officers have a 9.388 practice score more. The difference is statistically significant, as shown by the p-value of 0.008. The practice score of other doctors' cadre relative to consultants/specialists is not statistically significant (Figure 3).
Figure 3: Summary of the Travel Medicine Certification.
Discussion
Statement of Principal Findings
The attitudes of participants in this study were overwhelmingly positive, with 94.4% classified as having excellent (high) attitudes towards travel medicine, 4.5% average, and only 1.1% low. This finding indicates strong professional recognition of the importance of pre-travel health interventions in mitigating risks, such as vector-borne diseases and infections, even in a setting where the specialty remains relatively nascent. Such positivity may reflect intrinsic motivation among those already engaged in travel medicine practice, aligning with theoretical frameworks that link professional identity and perceived relevance to favourable dispositions. Critically, this high level of enthusiasm stands in notable contrast to several comparative studies targeting broader primary care populations.
Regarding knowledge, 61.8% of doctors scored high, 31.5% scored average, and 6.7% scored low, suggesting a generally competent understanding of core travel medicine concepts among this cohort. This performance converges with findings from certain regional studies but diverges sharply from others. For instance, in a cross-sectional study of primary healthcare physicians in Jeddah, Saudi Arabia, only 7.5% achieved adequate knowledge scores, with mean knowledge markedly lower [18]. Similarly, research among primary care physicians in Riyadh revealed suboptimal knowledge levels [21], while a study in Oman highlighted early-stage development of the field and called for intervention due to knowledge shortfalls [23]. In contrast, the present results show stronger knowledge, likely influenced by the study's focus on practitioners actively involved in travel medicine rather than general primary care physicians, as seen in the Gulf contexts where exposure to travel consultations is often sporadic.
Practice scores followed a similar encouraging pattern: 67.4% high, 22.5% average, and 10.1% low, suggesting that many participants effectively translate knowledge and attitudes into clinical practice, such as risk assessment and counseling. This convergence is evident when compared with the Nigerian context, where a parallel survey of travel medicine practitioners identified dedication amid challenges such as vaccine logistics and poor recognition, yet noted pockets of committed practice [19]. However, it diverges from findings in Saudi Arabia, where practice adequacy was as low as 4.0% in Jeddah [18] and sub-optimal in Riyadh [21], and from Oman, where only about 58% of primary care physicians reportedly provided pre-travel consultations [23]. Studies in India and Qatar among wider physician groups also documented more variable or limited practice integration [22, 24]. The tertiary or specialised sampling in the Indian tertiary hospital study yielded somewhat better alignment in select domains, yet overall gaps persisted outside dedicated groups [20].
The tri-level categorisation of KAP in this study reveals notable strengths in a self-selected group of Nigerian travel medicine practitioners, yet the patterns both converge with and diverge from the existing literature, revealing contextual influences. Studies conducted among general primary healthcare physicians in high-income Gulf settings or broader healthcare worker cohorts in India frequently report greater deficiencies, particularly in knowledge and practice, often attributed to limited formal training, infrequent exposure, and underdeveloped specialty recognition [18, 21-23]. In contrast, the more positive outcomes here, alongside local Nigerian findings [19], appear shaped by the convenience sampling of actively practicing individuals within an emerging professional network. This selection effect likely inflated performance relative to population-wide surveys, while studies of travellers themselves, such as in Thailand, shift focus away from practitioner KAP entirely [27]. Such contextual differences emphasize the impact of study population and setting on observed outcomes. Targeted recruitment stresses resilience and potential excellence in nascent fields, whereas broader samples expose systemic weaknesses. This reinforces the value of building upon existing positive foundations through expanded certification and training, while cautioning against over-generalisation beyond dedicated practitioners.
The regression results present a statistically significant model, albeit with modest explanatory power, indicating that while the included predictors (age, scores on knowledge and attitude, workers’ cadre: house officer, medical officer, and resident doctor) meaningfully shape travel medicine practice, a substantial proportion of behavioural variance remains unaccounted for. This pattern is not unusual within KAP-oriented studies, particularly in complex clinical domains where institutional, infrastructural, and behavioural factors interact. Comparable studies conducted in lower- and middle-income contexts, such as Bangladesh and Ethiopia, similarly report moderate model fits, stressing that practice is rarely determined by individual-level variables alone but is mediated by systemic constraints, professional exposure, and organisational support [33,34]. In contrast, more structured healthcare systems, such as those examined in European travel medicine research, tend to demonstrate stronger alignment between predictors and practice, reflecting more institutionalised training and clearer clinical pathways [28,29]. Thus, the relatively low R² observed here may be less a methodological weakness and more a reflection of contextual complexity within the Nigerian healthcare environment.
The positive and statistically significant effect of knowledge on practice reinforces a well-established theoretical assumption within KAP frameworks that cognitive competence underpins effective clinical behaviour. This finding aligns with evidence across diverse health domains, including COVID-19 response and immunisation practices, where higher knowledge levels consistently predict improved adherence to best practices [30,31]. However, the relatively modest coefficient suggests that knowledge alone is insufficient to drive optimal practice, a conclusion echoed in studies of healthcare-associated infections and pandemic preparedness, where structural and motivational factors often moderate this relationship [32]. In the specific context of travel medicine, these findings gain further significance given the documented gaps in pre-travel health practices among Nigerian travellers, which may partly reflect inconsistencies in provider knowledge translation [9].
More striking is the role of attitude, which emerges as the strongest predictor of practice. This finding both converges with and extends existing literature, particularly studies demonstrating that attitudinal orientation, such as perceived importance, risk sensitivity, and professional commitment, can exert a stronger influence on behaviour than knowledge alone [33,34]. In travel medicine, where proactive engagement and patient counselling are central, a positive attitude may translate into more diligent risk assessment and preventive guidance. This is consistent with findings among Nigerian travellers, where compliance with travel vaccines has been linked more closely to perception and willingness than mere awareness [37]. The implication is clear: strengthening practitioner attitudes through professional orientation and value-based training may yield greater improvements in practice than knowledge enhancement alone.
The significance of cadre; particularly the unexpectedly higher practice scores among house officers relative to consultants, introduces a more complex and somewhat counterintuitive dimension. While this finding diverges from conventional expectations that experience correlates with better practice, it may reflect generational differences in training exposure, recent curriculum updates, or greater familiarity with digital guidelines among younger practitioners. Similar patterns have been observed in studies examining emerging health domains, in which early-career professionals demonstrate greater compliance with updated protocols [32]. At the same time, the lack of significance among other cadres suggests inconsistency in role-based competence, reinforcing concerns about the absence of standardised training frameworks in travel medicine. This aligns with calls for structured certification and competency-based education, as highlighted in global travel health discourse [35,36]. Interestingly, these findings point to a critical need for harmonised professional development systems that bridge generational and experiential gaps, thereby ensuring more consistent and globally aligned travel medicine practice.
Strengths and Weaknesses of the Study
A key strength of this study lies in its empirical focus on an under-researched yet increasingly important domain within the Nigerian healthcare system. By integrating KAP variables within a single analytical framework, the study offers a nuanced understanding of how cognitive and behavioural factors interact to shape travel medicine practice. The use of regression analysis further strengthens the study by moving beyond descriptive insights to identify statistically significant predictors, thereby providing evidence with practical and policy relevance. Additionally, the inclusion of practitioners actively engaged in travel medicine enhances the contextual validity of the findings, while the use of standardised data analysis tools ensures methodological rigour and internal consistency.
However, a few limitations temper the interpretability and generalisability of the findings. The reliance on a cross-sectional design restricts causal inference, making it difficult to determine the directionality of observed relationships. The use of convenience sampling introduces potential selection bias, likely over-representing practitioners with prior interest or engagement in travel medicine, thereby potentially inflating knowledge and attitude scores. Furthermore, the relatively small sample size and the modest explanatory power of the regression model suggest that important contextual and institutional variables such as access to resources, organisational support, and formal training were not fully captured. These limitations point to the need for more robust study designs to better account for the complex determinants of practice in this field.
Strengths and Weaknesses in Relation to Other Studies
A key strength of this study, relative to the existing literature, lies in its analytical advancement beyond predominantly descriptive KAP studies. While several studies, such as those conducted in Saudi Arabia and Oman, largely report distributions of knowledge, attitudes, and practices without modelling their interrelationships [18,23], the present study employs regression analysis to identify statistically significant predictors of practice. This strengthens the explanatory value of the findings and aligns with more analytically rigorous approaches observed in studies on infectious diseases and public health behaviour, where multivariate techniques are used to unpack behavioural determinants [33,34]. Furthermore, by situating its analysis within the Nigerian context, the study complements evidence from both high- and middle-income settings, thereby reinforcing the cross-contextual relevance of the KAP framework while extending it to a relatively underexplored healthcare environment [9,28].
However, the study’s reliance on a relatively small, convenience-based sample contrasts with those of larger, more systematically designed studies, which often enhance representativeness and inferential robustness [29,30]. Additionally, unlike studies that explicitly incorporate structural and institutional variables such as training exposure, certification pathways, and organisational support, the current analysis captures these only indirectly, thereby limiting its capacity to fully explain practice variability. This may account for the modest explanatory power of the model and the somewhat divergent findings regarding professional cadre. In contrast, research emphasising structured training and competency frameworks in travel medicine highlights the critical role of institutionalisation in shaping consistent practice outcomes [35,36]. Consequently, while the study provides meaningful insights, its methodological constraints underscore the need for multilevel designs that better align with and build on existing international evidence.
Discussion of Important Differences in Results
An important point of divergence in the results lies in the relative strength of attitude over knowledge as a predictor of practice, as well as the unexpectedly higher performance among junior cadres, particularly house officers. While several studies report a more linear relationship in which knowledge predominantly drives practice [18,22], the present findings suggest a more behaviourally nuanced dynamic, in which attitudinal disposition exerts a stronger influence, consistent with evidence from broader public health contexts [33,34]. Additionally, unlike studies conducted in more structured healthcare systems where seniority often correlates with better practice due to experience and access to institutional training [29,36], this study reveals a reversal of that pattern, likely reflecting differences in recent training exposure, digital literacy, and the relatively under-institutionalised nature of travel medicine in Nigeria. This contrast underscores how contextual factors, particularly variations in training systems and professional development pathways, can significantly reshape expected KAP relationships.
Meaning of the Study
This study underscores that effective travel medicine practice is not solely a function of knowledge but is more powerfully shaped by attitudinal orientation and professional context, thereby reinforcing the behavioural foundations of the KAP framework. It highlights a critical gap between experiential competence and formal certification within Nigeria’s healthcare system, suggesting that without structured training and institutional support, practice remains uneven and potentially unsustainable. In this sense, the study contributes both theoretically by refining the understanding of KAP dynamics and practically by signalling the need for standardised capacity-building to align local practice with global travel health standards.
Unanswered Questions and Future Research
Important questions remain regarding the structural and institutional factors shaping travel medicine practice, particularly the roles of formal training, certification pathways, and health system capacity in influencing outcomes beyond individual knowledge and attitude. Future research should adopt longitudinal and multi-level designs to examine causal relationships and integrate organisational variables, while also exploring why junior practitioners outperform senior counterparts in this context. Comparative and cross-national studies would be especially valuable in clarifying how differing healthcare systems mediate the KAP relationship and in identifying scalable models for strengthening travel medicine practice in resource-constrained settings.
Limitations
This study is subject to some limitations that shape the interpretation and applicability of its findings. The cross-sectional design restricts causal inference, limiting conclusions to associations rather than directional effects within the KAP framework. The use of convenience sampling and a relatively small sample size introduces selection bias and constrains the generalisability of the results beyond the study population, particularly within a diverse healthcare system such as Nigeria’s. Furthermore, reliance on self-reported measures may inflate estimates of KAP due to social desirability bias. The modest explanatory power of the regression model also indicates that key structural and institutional variables, such as access to training, organisational supports, and resource availability, were not fully captured, thereby limiting the study’s utility for informing comprehensive policy or practice interventions without further contextual investigation.
Conclusion
This study demonstrates that travel medicine practitioners in Nigeria exhibit relatively strong knowledge, highly positive attitudes, and generally good practice, despite notably low levels of formal certification. Crucially, the findings reveal that while knowledge significantly predicts practice, attitude emerges as the more influential driver, underscoring the behavioural dimension of clinical competence within the KAP framework. The unexpected variation across professional cadres further suggests that recent training exposure and contextual factors may outweigh experience in shaping practice quality. These insights carry important implications for policy and professional development: strengthening structured training pathways, institutionalising certification, and embedding travel medicine within continuous professional education are essential steps towards standardising practice and aligning it with global benchmarks. Moving forward, more robust, multi-level and longitudinal research is needed to capture the systemic determinants of practice and to inform scalable interventions within resource-constrained healthcare settings.
What is Already Known on this Topic?
- Travel medicine practice is shaped by the interplay of knowledge, attitudes, and contextual healthcare factors.
- Gaps in formal training and certification remain a persistent challenge, particularly in low- and middle-income countries.
- Positive attitudes and adequate knowledge do not always translate into optimal clinical practice due to systemic constraints.
What this Study Adds:
- Provides empirical evidence from Nigeria highlighting strong practitioner attitudes despite low certification uptake.
- Demonstrates that attitude is a stronger predictor of practice than knowledge in this context.
- Reveals unexpected cadre-related differences, suggesting the influence of recent training and evolving professional dynamics.
References
- Enitan SS, Unata IM, Akele RY, Edafetanure-Ibeh OM, Dada MO, et al. (2024) The Role of Travel Medicine in Managing Future Pandemics: Lessons Learned from Global Infectious Disease Outbreaks. Intl J Trav Med Glob H 12: 10-21.
- Pennino F, Fiorilla C, Sorrentino M, Armonia U, Parisi A, et al. (2023) Investigating Awareness Regarding Travel-Related Infectious Disease Prevention in a Metropolitan Area. Trop Med Infect Dis 8: 476.
- Hu F, Wen J, Zheng D, Wang W (2023) Travel Medicine in Hospitality: An Interdisciplinary Perspective. Int J Contemp Hosp Manag 35: 3134-3153.
- Adesuyi OO, Edy-Ewoh U, Ojo AV, Akinola OH (2024) Tourism and Economic Growth in Nigeria and South Africa: A Comparative Analysis. J Econ Allied Res 9: 240-255.
- Kolawole O, Quigley A, Chughtai AA, MacIntyre CR (2026) Early Detection and Surveillance of Infectious Disease Outbreaks in Nigeria. J Med Syst 50: 1-11.
- Olumade TJ, Adesanya OA, Fred-Akintunwa IJ, Babalola DO, Oguzie JU, et al. (2020) Infectious Disease Outbreak Preparedness and Response in Nigeria: History, Limitations and Recommendations for Global Health Policy and Practice. AIMS Public Health 7: 736-750.
- Akodu BA, Ogwu FO, Abiola AHO (2019) Knowledge, Attitude and Compliance towards Travel Vaccines among Nigerian Travellers at an International Airport. Afr J Prm Health Care Fam Med 11: 2063.
- Feeney AJ, Goad JA, Flaherty GT (2024) Global Perspective of the Risks of Falsified and Counterfeit Medicines: A Critical Review of the Literature. Travel Med Infect Dis 61: 102758.
- Jegede OS, Ijitade G, Fatoye OA, Jegede TM, Aderinto N, et al. (2023) International Health Regulations and Pre-Travel Health Practices of International Travelers at Nigerian Airport: A Cross-Sectional Study. Trop Dis Travel Med Vaccines 9: 21.
- Simsek P, Kako M, Harada N, Abrahams J, Tayfur I (2024) Scoping Review of Exploring the Roles of Primary Care Providers to Increase Disaster Preparedness of Vulnerable Populations. Prog Disaster Sci 23: 100339.
- Al-Dahshan A, Ahmed S, Joudeh A, Kehyayan V (2025) Exploring primary care physicians' role in travel medicine: a scoping review of knowledge, practices, and training. Trop Dis Travel Med Vaccines 11: 4.
- Alghamdi AI, Alnamshan AZ, Kofi M, Alarfaj G, Alessa MF, et al. (2026) Knowledge, Attitude, and Practice of Travel Medicine among Primary Healthcare Physicians at Al Wizarat Primary Health Care Centers in Saudi Arabia. J Clin Pract Med Res 1: 159-167.
- Borrow R, Caugant DA, Ceyhan M, Christensen H, Dinleyici EC, et al. (2017) Meningococcal Disease in the Middle East and Africa: Findings and Updates from the Global Meningococcal Initiative. J Infect 75: 1-11.
- Deasy E, Seoighe A, Ryan C, Byrne S, Dalton K (2024) Pharmacy Stakeholders' Views and Experiences of the Credentialing of Advanced or Specialist Pharmacist Practice: A Mixed Methods Systematic Review. Explor Res Clin Soc Pharm 16: 100522.
- Olatunde O, Ilodiba N, Alawode O, Alao A, Kajero A, et al. (2025) Knowledge, Attitude, and Practice of Travel Medicine among Healthcare Practitioners in Nigeria: A Cross-Sectional Study. Intl J Travel Med Glob Health 13: 288-297.
- Hassan ZI, Afolaranmi TO (2015) The Knowledge and Uptake of Travel Vaccine among Medical Doctors in a Tertiary Health Institution in Plateau State, North Central Nigeria. Indian J Community Med 40: 177-182.
- Madubuko CC, Nwaka TFE (2024) The Alarming Exodus of Nigerian Professionals: The Devastating Consequences of Human Capital Flight and Migration on Nigeria's Economic Development. Am J Int Relat 9: 1-63.
- Alzahrani A, Alzaghabi F, Raza MS (2025) Knowledge, Attitudes, and Practices Regarding Travel Medicine among Primary Healthcare Physicians in Jeddah, Saudi Arabia: A Cross-Sectional Study. Cureus 17: e91836.
- Babalola IA, Alao AO, Adeniyi B (2026) Challenges and Prospects of Travel Medicine Practice in Nigeria: A Cross-Sectional Survey of Travel Medicine Practitioners. Cureus 18: e104901.
- Sadiq S, Bhagat V, Rani N (2024) Knowledge, Attitude and Practices Regarding Travel Medicine among Health Care Workers in a Tertiary Care Centre. Int J Basic Clin Pharmacol 13: 855-858.
- Sharahili AA, Al-Eanzi F, Ghzwany AA, Alazmi AM, Alhwsawi EA (2021) Knowledge, Attitude, and Practice of Travel Medicine Among Primary Health Care Physicians in Cluster-1, Riyadh City, Saudi Arabia: A Cross-Sectional Study. J Fam Med Prim Care 10: 2587-2593.
- Kumar A, Rajendran A, Usman M, Ahuja J, Samad S, et al. (2022) Development and Validation of a Questionnaire to Evaluate Knowledge, Attitude, and Practices Regarding Travel Medicine Among Physicians in an Apex Tertiary Hospital in Northern India. Trop Dis Travel Med Vaccines 8: 13.
- Kurup PJ, Al Abri SS, Al Ajmi F, Khamis HA, Singh J (2019) Knowledge, Attitude and Practice of Travel Medicine Among Primary Care Physicians in Oman: The Need for Intervention. East Mediterr Health J 25: 40-46.
- Al-Dahshan A, Selim N, Al-Kubaisi N, Mahfoud Z, Kehyayan V (2023) Scope and Predictors of Travel Medicine Practice Among Primary Care Physicians in Qatar. Prev Med Rep 35: 102337.
- Sadiq S, Bhagat V, Rani N (2024) Knowledge, Attitude and Practices Regarding Travel Medicine Among Health Care Workers in a Tertiary Care Centre. Int J Basic Clin Pharmacol 13: 855-858.
- Saleema A-R, Vijayan AP, Muhammed KJ, Mubeena TF (2026) A Study on Knowledge, Attitude and Practices (KAP) Towards Adult Immunizations Among Health Care Professionals. J Fam Med Prim Care 15: 89-104.
- Leowattana P, Luvira V, Tangpukdee N, Looareesuwan P, Siripoon T, et al. (2025) Knowledge, Attitudes, Practices and Vaccine Acceptance Towards Seasonal Influenza Vaccination Among International Travelers: A Cross-Sectional Survey in Thailand. Trav Med Infect Dis 66: 102863.
- Bogacka A, Wroczynska A, Grzybek M (2025) Polish Travellers on the Move: Knowledge of Travel Health and Associated Practices Among Polish Travellers Abroad. Trav Med Infect Dis 65: 102842.
- Baglivo F, De Angelis L, Vannini F, Agostini A, Todaro A, et al. (2025) Italian Medical Professionals' Practices, Attitudes, and Knowledge in Travel Medicine: Protocol for a National Survey. JMIR Res Protoc 14: e59511.
- Samy S, Lami F, Rashak HA, Al Nsour M, Eid A, et al. (2021) Public Health Workers’ Knowledge, Attitude and Practice Regarding COVID-19: The Impact of Field Epidemiology Training Program in the Eastern Mediterranean Region. J Public Health 43: 1-11.
- Rahiman SA, Vijayan A, Kutty JM, Mubeena TF (2026) A Study on Knowledge, Attitude and Practices (KAP) Towards Adult Immunizations Among Health Care Professionals. J Fam Med Prim Care 15: 89.
- Ketata N, Ben-Ayed H, Trigui M, Maamri H, Ben-Hmida M, et al. (2022) Knowledge, Attitudes, Practices, and Their Associated Factors Against the Growing Threat of COVID-19 Among Medical Students. Electron J Gen Med 19: em415.
- Patwary MM, Hossain MR, Sultana R, Dazhamyar AR, Parsa AD, et al. (2022) Knowledge, Attitudes and Practices of Healthcare Professionals Toward the Novel Coronavirus During the Early Stage of COVID-19 in a Lower-and-Middle Income Country, Bangladesh. Front Public Health 10: 988063.
- Shacho E, Ambelu A, Yilma D (2024) Knowledge, Attitude, and Practice of Healthcare Workers Towards Healthcare-Associated Infections in Jimma University Medical Center, Southwestern Ethiopia: Using Structural Equation Model. BMC Health Serv Res 24: 1611.
- Landry P (2017) The Certificate in Travel Health. J Trav Med 25.
- Hess KM, Seed SM, Clark EH, Lombardo T, Norman FF, et al. (2024) Multidisciplinary Travel Health Education: Current Status and Rationale for Standardized Competencies. J Trav Med 31: taae130.
- Akodu BA, Ogwu FO, Abiola A-HO (2019) Knowledge, Attitude and Compliance Towards Travel Vaccines Among Nigerian Travellers at an International Airport. Afr J Prm Health Care Fam Med 11: a2063.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.