Intravenous Anesthesia for Total Body Irradiation in a Child without Oxygen Support: Case Report
by Anna Lúcia Calaça Rivoli1, Luiz Eduardo Imbelloni2*, Sylvio Valença de Lemos Neto3, Patrícia L Procópio Lara4, Ana Cristina Pinho5, Pedro Henrique Souza Kelly6, Renata Pra7, Norma Sueli Pinheiro Módolo8, Geraldo Borges de Morais Filho9
1Anesthesiologist at the National Cancer Institute (INCA), Brazil
2National Cancer Institute (INCA), Senior Researcher, Rio de Janeiro, RJ, Brazil
3INCA Anesthesiologist, Responsible for the CET-SBA of the National Cancer Institute, Rio de Janeiro, RJ, Brazil
4Anesthesiologist at the National Cancer Institute (INCA), Brazil
5INCA Anesthesiologist, Co-Responsible for the CET-SBA of the National Cancer Institute, Rio de Janeiro, RJ, Brazil
6Anesthesiologist Resident of CET-SBA of the National Cancer Institute, Rio de Janeiro, RJ, Brazil
7Anesthesiologist at the National Cancer Institute – HC2 (INCA), Brazil
8Professor of the Department of Surgical Specialties and Anesthesiology at Faculty of Medicine of Botucatu - Unesp, Botucatu, SP, Brazil
9Master in Labour Economics, UFPB, João Pessoa-PB. Statistician of the Complexo Hospitalar Mangabeira, João Pessoa-PB, Brazil
*Corresponding author: Luiz Eduardo Imbelloni, National Cancer Institute (INCA), Senior Researcher, Av. Epitácio Pessoa, 2356/203, Lagoa, 22411-072- Rio de Janeiro, RJ - Brazil
Received Date: 20 March, 2024
Accepted Date: 27 March, 2024
Published Date: 29 March, 2024
Citation: Rivoli ALC, Imbelloni LE, de Lemos Neto SV, Lara PLP, Pinho AC, et al. (2024) Intravenous Anesthesia for Total Body Irradiation in a Child without Oxygen Support: Case Report. J Community Med Public Health 8: 425. https://doi.org/10.29011/25772228.100425
Abstract
Background: Total body irradiation twice daily for three consecutive days followed by chemotherapy for conditioning pediatric patients with acute lymphoid leukemia before bone marrow transplantation is superior to chemo conditioning alone. In children, this procedure must be performed with anesthesia, which can be inhaled or intravenous. Case report: The patient was a four-year-old child, weighing 18 kg, with a diagnosis of B-cell acute lymphoblastic leukemia and planned for stem cell transplantation. Parents’ consent form was signed to perform repeated anesthesia (twice/day) for three consecutive days. After monitoring and review of the venoclysis, it was intravenous sedation was performed for the procedure with administration of midazolam 3 mg, ketamine 10 mg (0.5 mg/kg) and dexmethedomidine (0.5 mg/kg). During the procedure, oxygen saturation remained between 94-100%, and at the end, the patient was under observation but without the need for hemodynamic and ventilatory support. Conclusion: Every year the number of procedures performed by interventional radiology in children with cancer increases, thus new anesthetic techniques are used, such as in this case the use of intravenous medication without the need for intubation or laryngeal mask airway, and without the use of supplemental oxygen, without hypoxemia or cardiorespiratory complications occur.
Keywords: Anesthesia; Children; Total body irradiation; Risks; Sedation
Introduction
In recent years, the complexity of patients undergoing interventional radiology has increased, thus also increasing the demand for anesthetic support with all types of anesthesia [1]. Total Body Irradiation (TBI) is a type or radiation therapy is a treatment that delivers small doses of irradiation to your entire body. TBI is used in several types of cancer, such as leukemias, lymphomas, multiple myeloma, and some solid tumors [2]. The TBI treatment is usually delivered twice a day for three to four consecutive days [3]. In pediatric patients, anesthesia or sedation is required to conduct this very crucial treatment effectively.
Most of the articles consulted on the various search sites addressed the form of TBI, and few articles on the anesthetic technique most used in children, and few case reports. However, the provision of sedation and analgesia for children undergoing TBI is now routine and the standard of care. Many pediatric patients may require anxiolysis to have CT or MRI imaging, ultrasound, or echocardiography to ensure adequate imaging is obtained and minimize patient stress [4]. Due to children’s wide age differences and developmental levels, sedation of infants and children is associated with unique challenges for anesthesiologists.
Pediatric procedural sedation refers to techniques and medications used to minimize anxiety and pain associated with unpleasant procedures. The objective of this case report is a 4-year-old child, submitted to two TBI procedures per day, on three consecutive days, using intravenous drugs, without intubation or laryngeal mask airway and without oxygen supply.
Case Report
We recently created a protocol to study the use of radiotherapy in children, having been registered in Plataforma Brazil (CAAE: 95207426.8.0000.5274) and was approved by the Ethics Committee at National Cancer Institute (INCA) with number 8.146.313. A preoperative anesthesia assessment was done, and the informed consent form was signed by one of the children’s parents.
Male patient, requesting together with his parents not to use a mask, as he was panicking, 4 years old, 18 kg, diagnosed with type B acute lymphoblastic leukemia. Eligible for treatment with allogeneic bone marrow transplant, the donor being the father, underwent preparation consisting of TBI carried out by the Clinac CS Linear Accelerator device, Varian Medical Systems (Figure 1), and high doses of chemotherapy with vincristine sulfate (1.5 mg/ kg), daunorubicin (30 mg/m2), asparaginase (5,000 IU/m2). The TBI program consisted of six sessions, twice a day with a 6-hour break between them and lasting one hour, under anesthesia. As part of the routine for performing TBI, the six procedures were performed by different anesthetists, but with the same protocol.

Figure 1: Clinac CS Linear Accelerator device, Varian brand.
For the first treatment session of each day, nothing per oral period was six hours for solid and semi-solid food. In the second treatment session of each day, clear liquid was allowed up to two hours prior to the second anesthesia induction of the day. Standard monitoring for pediatric TBI patients, including electrocardiogram, and oxygen saturation. The anesthetic technique performed was intravenous after revision of the venous access Broviac®/ Hickman® central venous line semi-implantable double lumen 7 French, with the following drugs and doses: midazolam 3 mg (0.15 mg/kg), ketamine 10 mg (0.5 mg/kg), dexmedetomidine (0.5 mg/ kg), and if necessary, propofol (10 mg). In one session in the morning and two in the evening, supplementation with propofol 10mg was necessary, so he could leave his mother and be taken to the TBI room. The monitoring control used was through the closedcircuit camera in the radiotherapy room. There were no changes in heart rate (Figure 2), no respiratory problems and oxygen saturation ranged from 94 to 100% in all sessions (Figure 3). In one session in the morning and another in the evening, midazolam needed to be reversed with flumazenil. In the other children anesthetized in the morning, flumazenil was not used to reverse midazolam, at the mother’s request, as the child would undergo the second treatment at night, and would remain drowsy, which was woken up by the anesthetist (Table 1).
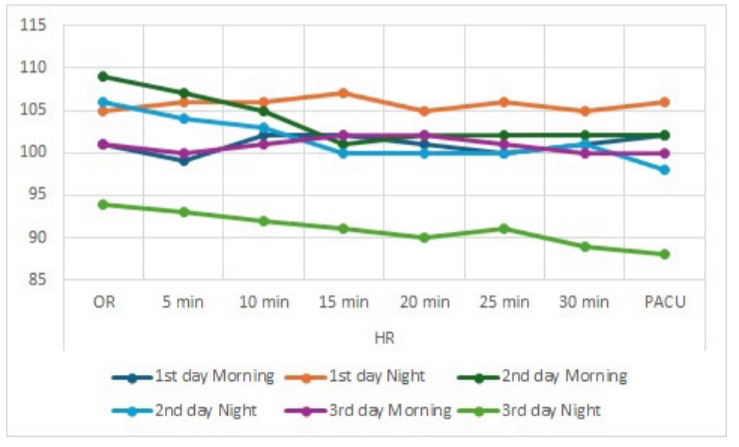
Figure 2: Heart rate from arrival in the operating room to PACU.
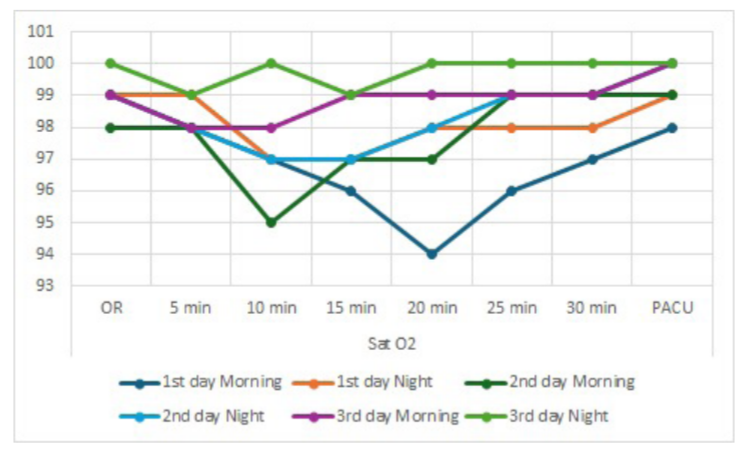
Figure 3: Oxygen saturation from arrival in the operating room to PACU.
Table 1: Medications and doses used in the six TBI sessions.
|
Sessions |
Time (h) |
MDZ mg |
KETA mg |
DEX mg |
PRO mg |
FLU mg |
SO2 |
|
1st |
In the morning |
3 |
10 |
10 |
No |
No |
98 to 96 |
|
2nd |
At night |
3 |
10 |
10 |
10 |
0.2 |
99 to 97 |
|
3rd |
In the morning |
3 |
10 |
10 |
No |
0.1 |
99 to 94 |
|
4th |
At night |
3 |
10 |
10 |
No |
No |
100 to 98 |
|
5th |
In the morning |
3 |
10 |
10 |
10 |
No |
99 to 98 |
|
6th |
At night |
3 |
10 |
10 |
10 |
No |
100 to 99 |
|
MDZ: Midazolam, KET: Ketamine, DEX: Dexmethedomidine, PRO: Propofol, Flu: Flumazenil, SO2: Maximum and minimum saturation values without oxygen enrichment. At the end of the procedure, the child was sent to the Post-Anesthetic Care Unit (PACU), without oxygen enrichment, maintaining saturation ranging from 98-100%, without hemodynamic and ventilatory support, any adverse effects. |
|||||||
Discussion
TBI, due to its immunosuppressive properties, has been an important measure in the treatment of a series of diseases malignant, in chemo resistant diseases, and penetration into places such as the central nervous system and the testicles, well described since 1975 [5,6]. The TBI technique was performed twice a day (morning and evening), on three consecutive days, under intravenous sedation with midazolam, ketamine, dexmedetomidine, and occasionally propofol to refer the child to the TBI location. The technique allowed the non-use of oxygen support (catheter or mask) and saturation ranged from 94% to 100%.
The goal of sedation is to provide the necessary to perform a procedure whether it is painful, such as burn debridement or fracture reduction, or nonpainful, such as diagnostic imaging studies, including TBI [7]. Pharmacological agents used for sedation in children can be of different types, and can be administered through multiple routes, including oral, intranasal, rectal, intramuscular, intravenous, and inhalational [7]. In the present report, the child was anesthetized intravenously with three main medications (midazolam, ketamine, dexmedetomidine). Propofol was added three times to facilitate transportation from the room to the OR. Midazolam had to be reversed twice.
a2-Agonists, such as clonidine and dexmedetomidine are useful adjuvants for sedation since they reduce anesthetic requirements with very little respiratory depression and no deleterious effects on natural sleep when compared to opioids and benzodiazepines [8]. The use of a dose three times higher than the recommended dose of midazolam resulted in the need to use its antagonists in two sessions, one in the morning and one in the evening, helping with rapid awakening in these sessions.
With the aim of verifying the effect of repeated general anesthesia (sevoflurane 5-8% in 50% of O2-N2O, fentanyl, atracurium) on behavior and emotions in thirty-five children aged 1½-5 years old, compared to healthy children, showed that there is a risk for subsequent behavioral and emotional disturbances [9]. In a recent study with 25 children undergoing sedation and anesthesia during radiotherapy treatment was required mainly in young children [10]. Sevoflurane as monotherapy without venous access turned out to have no severe complications; however, sevoflurane MAC increases above 1.5 were associated with the onset of complications. The awakening was quick (6 minutes) as well as the discharge for residence (19 minutes). Unfortunately, this study did not evaluate behavioral and emotional disturbances.
In a Letter to the Editor in 1978, the authors suggested that in TBI the majority British anesthetists used general anesthesia, showing its benefits but the authors of the letter did not believe it was routinely necessary [11]. In a recent case report, a threeyear-old child, after standard monitoring, was anesthetized with sevoflurane 8% with 100% oxygen and a laryngeal mask of size 2 was inserted, and maintenance with sevoflurane to a level of 2% with 100% oxygen, with the average duration of each treatment period was about 20-25 minutes, without complications [12]. This case report is completely different from ours, since we only used midazolam, dexmedetomidine, and ketamine without the aid of intubation or laryngeal mask airway, without the need of supplemental oxygen via a catheter or mask, and oxygen saturation varying from 94 to 100%, without cardiorespiratory changes, and other side effects.
A retrospective study carried out from 2014 to 2016, demonstrated that general anesthesia with propofol provided by a dedicated anesthesia team for pediatric radiation therapy yields few adverse events, in this remote, out-of-the-operating room venue [13]. Propofol (10 mg) was needed three times, once in the morning and twice in the evening, only to facilitate transportation from the room to the TBI location.
Twenty-six children, ranging from 2 months to 4 years old for TBI or Total Lymphoid-Tissue Irradiation (TLI), were anesthetized with diphenhydramine (0.5 mg/kg), atropine, ketamine 2 mg/kg through a catheter, showed that the technique with ketamine effectively would circumvent most of the logistic problems inherent to nuclear magnetic resonance [14]. Modernly, in this case we replace atropine, diphenhydramine, with midazolam and dexmedetomidine, without complications.
The combination of ketamine with propofol and dexmedetomidine has gained popularity for sedation and general anesthesia in different populations. A recent systematic review and meta-analysis showed that the association of ketamine with dexmetedomine (ketadex) was associated with lower pain scores, hypoxic events and airway obstruction, and emergence agitation [15]. In this same review, the authors believe that ketofol had greater clinical satisfaction, which can be attributed to the shorter recovery time and lower incidence of nausea and vomiting [15].
Conclusion
Every year the number of procedures performed by interventional radiology increases, and in the same way the anesthesia for these procedures has been challenging, and in hospitals for children with cancer it is also exciting to learn these new anesthesia techniques, offering a high level of care and improving the quality and humanism of these children with cancer. The a-2 agonist drugs have established a place in the modern anesthetic armamentarium because of their ability to produce a calming effect without causing respiratory depression, and by promoting cardiovascular stability while reducing anesthetic requirements, and a very much appreciated anti-sialagogue effect. Ketamine produces sedative, analgesic, and amnestic effects, without remarkable ventilatory impairment the time to onset of sedation is short, and recovery from sedation occurs quickly. The combination of midazolam, dexmedetomidine, and ketamine provided sufficient sedation for the duration of TBI, without the need for oxygen support, with saturation varying from 94 to 100%, and without side effects. In PACU, all six times the saturation was between 98 and 100%.
References
- Amin A, Lane JS (2018) The future of anesthesia for interventional radiology. Curr Opin Anesthesiol 31: 469-472.
- Wills C, Cherian S, Yousef J, Wang K, Mackley HB (2016) Total body irradiation: A practical review. Appl Rad Oncol 5: 11-17.
- Aschan J (2007) Risk assessment in haematopoietic stem cell transplantation: conditioning. Best Pract Res Clin Haematol 20: 295310.
- Callahan MJ, Cravero JP (2022) Should I irradiate with computed tomography or sedate for magnetic resonance imaging? Pediatr Radiol 52: 340-344.
- Thomas E, Storb R, Clift RA, Fefer A, Johnson FL, et al. (1975) Bonemarrow transplantation (first of two parts). N Engl J Med 292: 832-843.
- Thomas ED, Storb R, Clift RA, Fefer A, Johnson FL, et al. (1975) Bone-marrow transplantation (second of two parts). N Engl J Med 292: 895-902.
- Barnes S, Yaster M, Kudchadkar SR (2016) Pediatric sedation management. Pediatr Rev 37: 203-212.
- Giovannitti JA, Thoms SM, Crawford JJ (2015) Alpha-2 adrenergic receptor agonists: A review of current clinical applications. Anesth Prog 62: 31-39.
- Bakri MH, Ismail EA, Ali MS, Elsedfy TA, Sayed TA, et al. (2015) Behavioral and emotional effects of repeated general anesthesia in young children. Saudi J Anesth 9: 161-166.
- Imbelloni LE, Baroni D, Lara PLP, Lemos Neto SV, Pinho AC, et al. (2023) Prospective general inhalation anesthesia for pediatric patients undergoing radiotherapy. Pilot project with 25 children without venous access. Mathews J Anesth 4: 11.
- Whitwam JG, Morgan M, Owen JR, Goolden AW, Spiers AS, et al. (1978) General anaesthesia for high-dose total body irradiation. Lancet 1: 128-129.
- Butt MN, Shamim N, Faraz A (2024) Anesthetic challenges for a pediatric leukemia patient undergoing total body irradiation (TBI). A case report. Cureus 16: e53535.
- Khurmi N, Patel P, Koushik S, Daniels T, Kraus M (2018) Anesthesia practice in pediatric radiation oncology: Mayo Clinic Arizona’s Experience 2014-2016. Pediatr Drugs 20: 89-95.
- Lo JN, Buckley JJ, Kim TH, Lopez R (1984) Anesthesia for high-dose total body irradiation in children. Anesthesiology 61: 101-103.
- Elsaeidy AS, Ahmad AHM, Kohaf NA, Aboutaleb A, Kumar D, et al. (2024) Efficacy and Safety of Ketamine-Dexmedetomidine Versus Ketamine-Propofol Combination for Periprocedural Sedation: A Systematic Review and Meta-analysis. Curr Pain Headache Rep 28: 211-227.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.