Incidental Finding of a Left Intrathoracic Kidney Associated with Bochdalek Hernia in a Six-Month-Old Child: A Case Report
by Muhammad Afzal*, Amnah Fallatah, Huda Albugrain, Jasim Ahmed Alsayegh, Abdullah Moeid Alzahrani, Ghulam Ali Ansari
Pediatric Surgery Department, Maternity and Children’s Hospital, Dammam, Eastern Province, Kingdom of Saudi Arabia
*Corresponding author: Muhammad Afzal, Maternity and Children’s Hospital, Dammam, Eastern Province, Kingdom of Saudi Arabia
Received Date: 10 July 2025
Accepted Date: 17 July 2025
Published Date: 18 July 2025
Citation: Afzal M, Fallatah A, Albugrain H, Alsayegh JA, Alzahrani AM, et al. (2025). Incidental Finding of a Left Intrathoracic Kidney Associated with Bochdalek Hernia in a Six-Month-Old Child: A Case Report. Ann Case Report. 10: 2345. https://doi.org/10.29011/2574-7754.102345
Abstract
Background
Congenital diaphragmatic hernia (CDH) is a rare developmental anomaly characterized by translocation of abdominal viscera into the thoracic cavity. The most common form, accounting for 80-90% of cases, is a left-sided Bochdalek hernia (BH). In approximately 5% of renal ectopia cases, the kidney herniates into the thoracic cavity, and its association with BH is extremely rare, occurring in only 0.25% of cases.
Case Presentation
A 6-month-old infant was referred to our hospital for a case of left BH. The chest radiograph revealed the presence of BH along with opaque areas, which were later confirmed as the spleen and an Intrathoracic kidney (ITK) by contrast-enhanced CT. During surgery, the abdominal contents, including the transverse colon, a significant portion of the small intestine, and the spleen, were retrieved from the thoracic cavity, while the kidney was kept in situ. The diaphragmatic defect was repaired, leaving a small window on the medial side of the defect to accommodate the renal vessels and ureter. At the three-month follow-up, Doppler ultrasound, and at the six-month follow-up, CT urography showed a normally sized, functional intrathoracic kidney with normal renal vessels, ureter, and renal enhancement.
Conclusion
The coexistence of ITK and CDH is extremely rare; thus, a high index of suspicion about this association should be maintained when evaluating such cases. Contrast-enhanced CT is the most effective imaging modality for diagnosing ITK, planning surgery, and conducting follow-up. An ITK in an extra-pleural position, with elongated renal vessels and ureter, can be safely left in situ.
Keywords: Bochdalek Hernia; Children; CT urography; Intrathoracic kidney
Introduction
Congenital diaphragmatic hernia (CDH) is a rare developmental anomaly characterized by the migration of abdominal organs into the thoracic cavity through an abnormal opening in the diaphragm [1]. CDH occurs in approximately 1 in 2000 to 4000 live births worldwide each year [2]. A congenital defect in the posterolateral aspect of the diaphragm was first described in 1848 by Czech anatomist Vincent Alexander Bochdalek, after whom the condition is named, Bochdalek hernia (BH). BH is the most common type of CDH, representing approximately 80-90% of cases, with the majority occurring on the left side [3,4]. The small bowel, spleen, stomach, colon, and the left lobe of the liver are the organs that are mostly herniated through the diaphragmatic defect into the thoracic cavity. Ectopic kidneys are most commonly found in the pelvis, iliac region, abdomen, or thorax. The pelvis is the most common site, while the thorax is the least common, comprising about 5% of all cases [4-6]. The association of an ITK with a BH is even rarer, with a reported incidence of only 0.25% [1,4,7,8]. To date, approximately 200 cases have been documented globally, with more than 40 cases occurring in children [5]. Herein, we present the case of a 6-month-old boy with an ectopic thoracic kidney associated with a BH. This case report aims to highlight the rare presentation of an ectopic kidney with BH and underscores the need to maintain a high index of suspicious for their potential co-occurrence.
Case Report
A 6-month-old male infant, born at term, was referred from another hospital with a preliminary diagnosis of a left-sided congenital diaphragmatic hernia. Three days following the administration of routine immunizations per the national immunization schedule, the patient developed nonspecific symptoms including fever, cough, reduced activity, and poor oral intake. The initial evaluation was conducted at the private hospital, where X-ray chest demonstrated radiological features suggestive of a left-sided congenital diaphragmatic hernia. He was subsequently referred to our institution for further evaluation and specialized management.
On physical examination, the patient was tachypneic, with a respiratory rate of up to 85 breaths per minute, and febrile, with a temperature of 38.2°C. Auscultation exhibited decreased air entry on the left side of the chest. Abdominal examination showed an excavated abdomen. He was kept nil per os (NPO), a nasogastric tube was inserted, and intravenous (I/V) fluid, Augmentin, along with Paracetamol, were administered. Baseline laboratory investigations, including coagulation profile, serum electrolytes, renal function tests, and liver function tests, were within normal limits. However, the complete blood count (CBC) revealed a total leukocyte count at the upper limit of normal (10 × 10⁹/L), with a neutrophil predominance of 75%. A Chest radiograph revealed an obscured left diaphragmatic contour with multiple lucent and opacified areas overlying the left lung‘s lower zone, a mediastinal shift to the right, and a paucity of abdominal gas shadows, findings consistent with CDH (Figure 1). Computed tomography (CT) of the chest with oral and I/V contrast demonstrated a posterolateral defect in the diaphragm and herniation of the intestine, the spleen, and the left kidney into the left hemithorax. The intrathoracic kidney was mildly rotated but normal in size, with preserved corticomedullary differentiation, normal contrast excretion, and no evidence of hydronephrosis. The contralateral kidney was normally positioned, with no structural or functional abnormalities. (Figure 2a). Following stabilization of the patient's condition, the family was counselled, and informed written consent was obtained for surgical intervention. The diaphragmatic defect was accessed via an abdominal approach. Intraoperative findings revealed a 4 cm posterolateral diaphragmatic defect with a hernial sac containing the transverse colon, a significant portion of the small intestine, the spleen, and the left kidney, all of which had herniated into the thoracic cavity. All herniated organs, except the kidney, were successfully reduced into the abdominal cavity. The intrathoracic kidney with its vascular pedicle and ureter was identified as traversing through the defect into the thorax. The kidney was covered by peritoneum and located within the thorax, but outside the pleural cavity (extra-pleural). Moreover, the kidney was located high in the thorax and demonstrated elongated renal vessels originating from their usual anatomical locations, along with a long ureter (Figure 3). Given these findings, the kidney was left in situ. The sac was excised, and the diaphragmatic defect was repaired using interrupted non-absorbable sutures, with a small medial vent left to accommodate the renal vessels and ureter. The patient experienced an uncomplicated recovery after surgery and was transferred to the pediatric intensive care unit, where he was managed on mechanical ventilation for two days. Postoperative renal Doppler ultrasound demonstrated a left intrathoracic kidney of average size, with no evidence of backpressure changes. The renal parenchyma exhibited a preserved echogenic pattern and maintained corticomedullary differentiation. Baseline laboratory investigations, including renal function tests, were within normal limits. He was successfully weaned off ventilator support after 48 hours and subsequently transferred to the pediatric surgical ward on the third postoperative day. Oral feeding was initiated on the fourth postoperative day and gradually advanced to full feeds over the following days. The patient was discharged on the eighth postoperative day in satisfactory condition.
At the three-month follow-up, renal function tests remained within normal limits, and Doppler ultrasound demonstrated no significant changes (Figure 2b). At six months, CT urography revealed a normally sized intrathoracic kidney with rotation of the lower pole, located in the posterior mediastinum. The renal vasculature was patent, with a normally draining renal vein, normal renal enhancement, and a normal ureter. There was no evidence of hydronephrosis or hydroureter (Figure 2c). The patient is still under annual follow-up by a pediatric surgeon, a nephrologist, and an urologist.
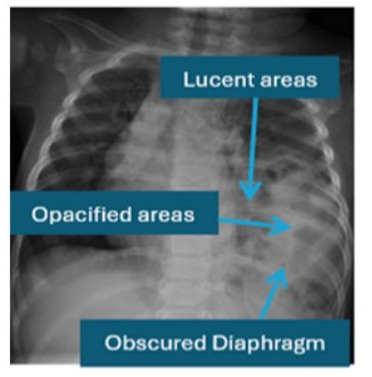
Figure 1: Chest radiograph show findings suggestive of CDH.
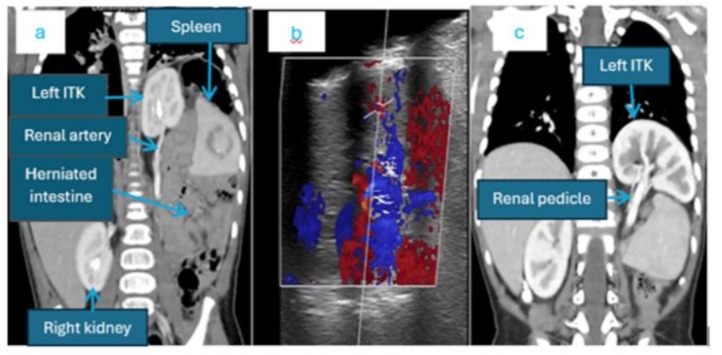
Figure 2: (a) Preoperative Contrast-enhanced CT demonstrating a left BH containing intestine, spleen, and a normal sized functioning kidney, with an elongated renal pedicle. (b) Postoperative Doppler ultrasound showing normal renal artery and renal vein blood flow. (c). Postoperative contrast enhanced CT showing the kidney with normal contrast excretion.
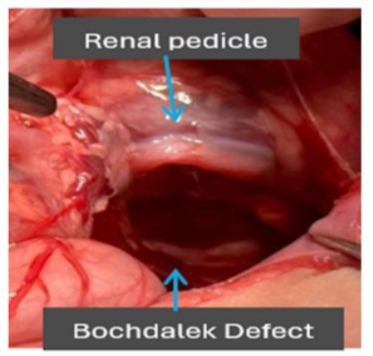
Figure 3: Shows Bochdalek defect and the renal pedicle traversing into the thoracic activity.
Discussion
BH is a congenital developmental defect resulting from the incomplete fusion of the pleuroperitoneal folds, typically occurring around 8 weeks of gestation [8,9]. It is characterized by a posterolateral diaphragmatic defect, typically allowing the herniation of abdominal viscera into the thoracic cavity [5,6]. It represents the most common form of congenital diaphragmatic hernia, predominantly (80-90%) occurring on the left side [2,10].
Bochdalek hernia (BH) can be identified prenatally by ultrasound or in the neonatal period by chest radiograph, while definitive diagnosis and detailed anatomical assessment are best achieved with computed tomography (CT) or magnetic resonance imaging (MRI) [9]. In most cases, abdominal organs such as the small intestine, spleen, stomach, colon, the left lobe of the liver and, exceptionally rare, and the kidney herniate into the thoracic cavity through the diaphragmatic defect. Clinical symptoms typically manifest during the neonatal period [10].
Renal ectopia (or ectopic kidney) is a developmental anomaly characterized by the kidney's abnormal position outside its typical anatomical location in the retroperitoneal renal fossa.
Ectopic kidneys are most common in the pelvic or lower lumbar regions and typically result from accelerated renal ascent during fetal development [10,11]. The ITK constitutes the rarest form of ectopic kidney, comprising approximately 5% of all reported cases, and its coexistence with a Bochdalek hernia is even exceedingly rare, with an estimated incidence of merely 0.25% [9,10]. Between 1985 and 2022, only 39 cases of pediatric intrathoracic ectopic kidney have been reported in the literature, reflecting the rarity of this condition [6]. As in our case, it is more frequently identified on the left side and has a higher incidence in males than in females [1,5,8,10].
ITK can be classified into four subtypes based on the diaphragmatic integrity: (1) real or true ITK with an intact diaphragm, (2) ITK with eventration of the diaphragm, (3) ITK with a traumatic diaphragmatic hernia, and (4) ITK with congenital diaphragmatic hernia [4,7,8,11]. According to this classification, our case is recognized as subtype 4.
The precise pathophysiology of ITK is still not well understood. Under normal embryological development, the kidneys ascend to the level of the first lumbar vertebra (L1) by the eighth week of gestation, coinciding with the closure of the pleuroperitoneal canal. The ITK associated with Bochdalek hernia is thought to be due to delayed closure of the diaphragm, permitting excessive cranial migration of the kidney. Alternatively, delayed mesonephric involution may lead to a prolonged renal ascent, accompanied by the elongation of the ureter [1,4,6].
Although ITKs usually develop well and function efficiently, they can rarely present with structural anomalies, such as an elongated ureter, a high origin of renal vessels, and medial deviation of the lower renal pole [1,6,10]. In our case, the ITK was accompanied by a relatively longer ureter, renal vessels, and deviation of the lower pole. However, the kidney was normal in size, exhibited a preserved echogenic pattern, and demonstrated instant excretion of contrast into the pelvicalyceal system on CT urography (Figure 2a). Similar characteristics of ITK have also been reported in other studies [5,6,10].
An isolated ITK is mostly diagnosed incidentally, while in congenital diaphragmatic hernia, there should be a high index of suspicion for the Intrathoracic location of the kidney. A chest radiograph is an initial tool for suspected diaphragmatic hernia, which may reveal an obscured left diaphragmatic contour, with multiple lucent areas suggestive of a diaphragmatic defect with herniation of intestine in the thoracic cavity. In addition, an opacified area on chest radiograph may raise suspicion of spleen, kidney, or herniation of both, warranting further evaluation, typically starting with ultrasound and confirmed by contrast-enhanced CT scan. In the index case, the initial chest radiograph findings were indicative of diaphragmatic hernia, while opaque areas raised suspicious of solid organ herniation. This was subsequently confirmed to be the spleen and kidney, initially through chest ultrasound and later by contrast-enhanced CT scan. Although chest radiograph may display ITK as a paravertebral lesion in the posterior mediastinum, and ultrasound secondarily aids in the diagnosis, CT urography is the best modality to establish the diagnosis [3]. It provides detailed information, including the abnormal position of the kidney, its size, shape, volume, as well as the course of the ureter and renal vessels. Additionally, it defines the extent of the diaphragmatic defect and other associated contents of the BH.
A conservative strategy is the preferred method of managing ITK, especially for the isolated subtype of ITK. Numerous studies support this approach. This strategy is justified by the fact that, despite the ectopic location of the kidney, its function typically remains preserved [10]. Similarly, when an ITK is associated with a BH, most clinicians recommend repairing the diaphragmatic defect without manipulating the ITK [7]. In such cases, relocation of the ITK into the abdominal cavity along with nephropexy is recommended only when the ectopic kidney is located within the pleural cavity, rather than in an extra-pleural position, as it is prone to be mobile [10]. In our case, we did not manipulate the ITK, due to its extra-pleural position, with relatively long renal vessels, and the ureter (Figure 2a). In such a case, mobilizing the kidney carries the risk of vascular or ureteral injury. Moreover, after relocation of the Kidney in the abdomen, it could result in ureteral folding or kinking of the renal vessels, thereby endangering renal perfusion and function. Hence, in such cases, repositioning the ITK to the abdominal cavity is not advisable [4].
Conclusion
ITK associated with BH is an exceptionally rare pathology. Its identification can be easily overlooked unless the clinician maintains a high index of suspicion for its co-occurrence with BH. Failure to identify ITK before surgery may pose significant risks to the renal vessels and ureter during surgical repair of the diaphragmatic defect. Contrast-enhanced CT is the best imaging modality as it not only confirms the ectopic location of the kidney but also delineates the origin of the ureter and the renal vessels, which is critical for formulating the surgical plan. Relocation of the intrathoracic kidney (ITK) into the abdominal cavity is not recommended if it has an extra-pleural fixed position and relatively long renal vessels and ureter.
Conflict of Interest
The Authors declare no conflict of interest.
References
- Zahid A, Nawaz F A, Duvuru R. (2022). Congenital Diaphragmatic Hernia with Kidney and Spleen Herniation in the United Arab Emirates: A Case Report. Cureus. 14: e26732.
- Pindoria N, Makanjuola J, Botha A, Nair R, Thurairaja R. (2018). ‘‘What Goes Up Must Come Down’’: Laparoscopic retrieval of a migrated intrathoracic kidney and repair of recurrent symptomatic diaphragmatic hernia, Journal of Endourology Case Reports. 4: 129-132.
- Naseri M, Ghalibafan, Alamdaran SA. (2021). Ectopic Intrathoracic Kidney Associated with Ipsilateral Ectopic Spleen and Diaphragmatic Hernia in a Pediatric Patient: A Case Report, Tanaffos. 20: 291-293.
- Saraç M, Bakal U, Tartar T, Canpolat S, Kara A. (2018). Bochdalek hernia and intrathoracic ectopic kidney: Presentation of two case reports and review of the literature. Niger J Clin Pract. 21: 681-686.
- Ji Z, Zhao Z, Xi H, Ren H. (2024). Laparoscopic repair of intrathoracic kidney associated with giant congenital diaphragmatic hernia: an infant case report and literature review. Front. Pediatr. 12: 1499644.
- Al Eraky M, Hassan L, Abou Zaid A. (2022). Congenital Intrathoracic Ectopic Kidney in Association with Bochdalek Hernia. Cureus. 14: e22674.
- Guo R, Dong C, Zhai Y, Zhao H, Lv L. (2024). Case Report: Thoracoscopic treatment of infradiaphragmatic pulmonary sequestration and intrathoracic kidney associated with congenital diaphragmatic hernia. Front. Pediatr. 12: 1442347.
- Mizzi C, Farrugia D, Choudhry MS. (2020). Congenital Diaphragmatic Hernia with Intrathoracic Renal Ectopia: Thoracoscopic Approach for a Complete Anatomical Repair. Eur J Pediatr Surg Rep. 8: e74-e76.
- Manasa P, Shah I, Sundaran P S. (2024). Left-Sided Intra-thoracic Ectopic Kidney with Symptomatic Bochdalek Hernia: A Case Report. Cureus. 16: e65452.
- Park J. (2020). Right intrathoracic ectopic kidney and pulmonary sequestration associated with right sided congenital diaphragmatic hernia. Journal of Pediatric Surgery Case Reports 61: 101600.
- Orlandi G, Toscano P, Gabrielli O, Di Lella E, Lettieri A. (2023). Prenatal Diagnosis of an Intrathoracic Left Kidney Associated with Congenital Diaphragmatic Hernia: Case Report and Systematic Review. J. Clin. Med. 12: 3608.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.