Impact of COVID-19 Policies on the Post-Pandemic Resurgence of Dengue Fever in Southeast Asia and Latin America
by Jiayi Chen*
United World College South East Asia, Singapore
*Corresponding author: Jiayi Chen, United World College South East Asia, Singapore
Received Date: 03 April, 2026
Accepted Date: 13 April, 2026
Published Date: 16 April, 2026
Citation: Chen J (2026) Impact of COVID-19 Policies on the Post-Pandemic Resurgence of Dengue Fever in Southeast Asia and Latin America. J Community Med Public Health 10: 567. DOI: https://doi.org/10.29011/2577-2228.100567
Abstract
Dengue fever, one of the most widespread mosquito-borne diseases, declined markedly during the early COVID-19 pandemic. However, a sharp 2023 resurgence raised concerns regarding the long-term impact of pandemic-era policies. This study examines sustained policy effects on dengue transmission across seven high-burden countries in Southeast Asia and Latin America through the analysis of monthly dengue cases and COVID-19 policy indices (2020–2023). Based on Oxford COVID-19 Government Response Tracker (OxCGRT) data, nations were categorized as Strict COVID-Control (SCC: Singapore, China) or Less Strict COVID-Control (LSCC: Indonesia, Argentina, Brazil, Colombia, Mexico). Generalized linear models assessed lagged effects of policy sub-components. Overall, dengue cases declined by 41.3% (95% CI: 36.2–46.5; p < 0.001) in 2020 relative to pre-pandemic levels. In LSCC countries, public information and vaccination policies were significantly protective (β = −174,354; p < 0.001). In SCC countries, economic interventions showed mixed effects: debt relief reduced dengue risk (β = −0.783; p = 0.003), while income support increased it (β = 0.583; p = 0.003). COVID-19 policies exerted lasting, heterogeneous effects on dengue transmission. Strengthening communication, vector control, and vaccination in LSCC settings, and maintaining vigilance and integrated surveillance in SCC settings, are crucial for sustainable dengue preparedness.
Keywords: Dengue fever; Endemic disease control; Policy Studies; COVID-19
Introduction
Dengue fever remains one of the most significant vector-borne diseases globally, with an estimated 100–400 million infections annually, disproportionately affecting Southeast Asia and Latin America [1]. Prior to COVID-19, the case number of dengue had been increasing steadily, driven by rapid urbanization, climate variability, and ineffective or inconsistently implemented vector control strategies [2]. The onset of the COVID-19 pandemic profoundly disrupted the transmission dynamics of many infectious diseases, including influenza, respiratory syncytial virus [3], tuberculosis and malaria [4]. Previous studies documented sharp reductions in the case number of dengue during the early lockdown phases of the COVID-19 pandemic, primarily attributed to mobility restrictions and reduced human–mosquito contact [5,6].
However, the incidence of dengue underwent a significant resurgence following the relaxation of COVID-19 policies, with 2023 witnessing the highest documented case number since 2000. In certain countries, such as Argentina, Brazil, and Singapore [7]. While previous studies have described a short-term decline in dengue during COVID-19 [6], there remains limited evidence on how long-term policy stringency and the relaxation of these policies shaped post-pandemic resurgence across diverse governance contexts.
In the present study, we systematically evaluated the post-COVID burden associated with dengue fever across Southeast Asia and Latin America, two regions that account for the majority of global dengue cases and where COVID-19 policies were both diverse and stringently documented [1,8]. We selected seven countries—China, Singapore, Argentina, Brazil, Colombia, Mexico, and Indonesia—on the basis of their high baseline dengue case number (≥ 2,000 reported cases in 2020) and availability of complete policy data. To allow for meaningful comparison, countries were selected into two groups using standardized criteria: Strict COVID Control (SCC) countries, defined as those with national lockdowns exceeding 50 consecutive days and an Oxford Stringency Index >80 during 2020–2022 (China and Singapore), and Less Strict COVID Control (LSCC) countries, which met neither threshold (Argentina, Brazil, Colombia, Mexico, and Indonesia). We constructed non-Bayesian regression models linking dengue case number to COVID-19 policy indices, with particular focus on economic support measures (e.g., income support, debt relief) and health-related interventions (e.g., public information campaigns, vaccination policy, and protective measures). This framework enabled us to evaluate how distinct policy domains differentially influenced the resurgence of dengue, and whether deviations from predicted trends were associated with shifts in physiological risk profiles, public awareness, or environmental conditions. By performing this research, we aimed to clarify the long-term impacts of COVID-19 on the epidemiology of dengue and to propose innovative and sustainable approaches to strengthen epidemic preparedness in the post-pandemic era. Our work contributes to the existing literature by providing one of the first multi-country, post-pandemic evaluations of dengue, with implications for policy design regarding how future pandemics may reshape the trajectory of endemic diseases.
Methods
Study design and participants
In this study, we focused on seven countries, three from Asia and four from South America, with at least 2,000 reported dengue cases in 2020, according to the OpenDengue database (https://opendengue.org/data.html) [9]. Monthly dengue case number for each country were extracted from the OpenDengue database between January 2020 and December 2023. Dengue case counts included both suspected and laboratory-confirmed cases. While reporting quality may vary between countries, reporting practices were assumed to be consistent within each country over time.
COVID-19 policy data
Monthly COVID-19-related policy indicators were retrieved from the Oxford Coronavirus Government Response Tracker (OxCGRT), as described by Hale et al. [8]. The OxCGRT Stringency Index was used as the benchmark variable for policy severity. In subsequent analyses, disaggregated policy variables, specifically the economic support and health system measures, were also extracted to assess the contribution of specific policies.
Climate adjustment
Since climate is known to be a major driver of dengue seasonality [6], we incorporated country-level climate controls into our regression model. Monthly mean temperature and seasonal rainfall patterns were extracted from publicly accessible ERA5 datasets [10]. Where rainfall data were unavailable, a binary indicator for rainy versus dry season was applied. This adjustment aligned with that used in previous literature relating to the modeling of dengue [6].
Grouping method
Based on the stringency and duration of pandemic control policies, countries were selected into two groups. Countries were classified into the Strict COVID-Control (SCC) group if they met both of the following criteria: (1) national COVID-19 quarantine or lockdown measures extended for at least 50 consecutive days, and (2) a mean OxCGRT Stringency Index value > 80 for the 2020–2022 period. Using these criteria, China and Singapore were categorized as SCC countries. All other countries (Indonesia, Argentina, Brazil, Colombia, and Mexico) were categorized into the Less Strict COVID-Control (LSCC) group. This grouping method aligned with previous work [6,8,11] and facilitated the comparison of long-term trends in dengue transmission under different public health governance models.
Statistical analysis
We applied a generalized linear model (GLM) to investigate the association between COVID-19 policy measures and the monthly dengue case number. The primary equation is given in Eq. (1).
In Eq. (1), represents the monthly case number of dengue for country c at time t, represents the OxCGRT stringency index for the prior month; f(·) represents a natural cubixc spline function; represent covariates, including temperature, rainfall (or seasonal dummies), and monthly fixed effects; represents the climate data collected to offset the impact of confounding variables; and represents the model error term.
Models were fitted separately for SCC and LSCC groups to capture potential differences in policy-disease dynamics. All regressions incorporated a one-month lag to reflect typical mosquito development and disease incubation cycles, consistent with previous modeling frameworks [12].
Other than GLM, we also conducted Principal Component Analysis (PCA) and cluster analysis on the data for closer analysis. PCA was essential for identifying the key policy dimensions driving variation in dengue dynamics across countries, reducing complex, correlated variables into a few interpretable components that explained over 90% of total variance. Cluster analysis further complemented this by uncovering distinct dengue case patterns within each policy group, revealing how differing combinations of interventions corresponded to markedly different disease burdens.
Model estimates were computed using EViews version 13 software (IHS Markit, 2024).
Under-reporting considerations
We acknowledge that the under-reporting of dengue may have occurred during the COVID-19 pandemic due to healthcare system strain and testing disruptions. Previous studies, including Islam et al. [11], demonstrated that care-seeking behavior declined during the early phases of the pandemic. While this may have impacted absolute counts, we assumed that trends within each country were consistent over time, given that the same national surveillance infrastructure was applied across all months in the designated period.
Results
General Trends
The study’s empirical analysis began by quantifying the global disruption in dengue transmission, identifying an overall decline of 41.3% (95% CI: 36.2–46.5; p < 0.001) in 2020 relative to pre-pandemic baselines (5.2 million in 2019 [6]). Despite this initial reduction, the 2023 resurgence was characterized by record-high case numbers in several study areas, particularly in Brazil and Singapore. To analyze the drivers of this resurgence, countries were categorized into two cohorts based on the Oxford COVID-19 Government Response Tracker (OxCGRT) metrics. The Strict COVID-Control (SCC) group, consisting of China and Singapore, was established through a mean Stringency Index exceeding 80 and the implementation of national lockdowns lasting over 50 consecutive days between 2020 and 2022. Conversely, Indonesia, Argentina, Brazil, Colombia, and Mexico were classified as Less Strict COVID-Control (LSCC) countries, as they did not meet both of these pre-defined stringency and duration thresholds (Figure 1).
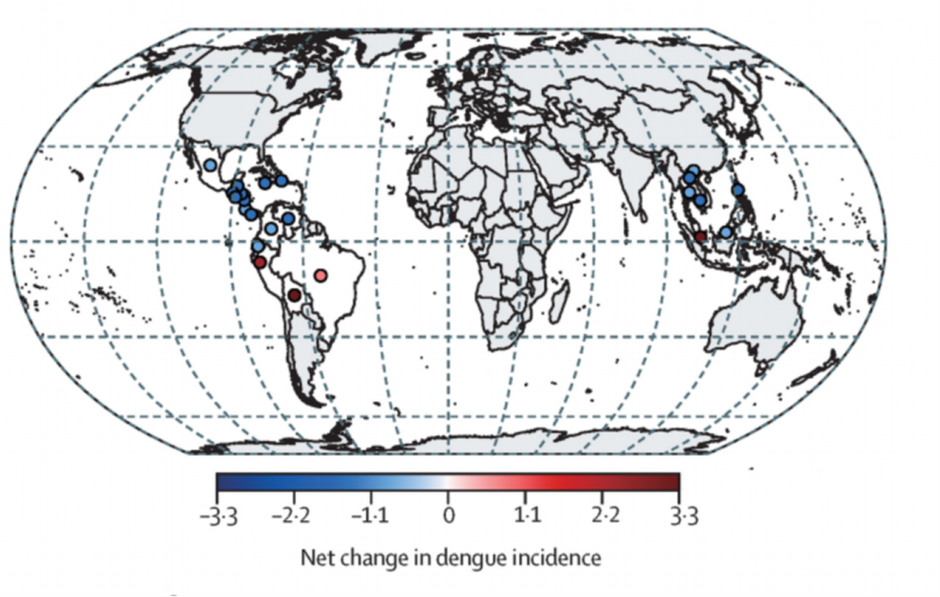
Figure 1: Changes in the global incidence of dengue during the COVID-19 pandemic [6].
Policy Impacts in SCC Countries
The epidemiological dynamics within the SCC countries were more heavily influenced by the duality of economic support measures rather than public health communication. Generalized linear models indicated a complex relationship with economic aid: while income support (E1) was positively associated with increased dengue risk (coefficient = 0.583; p = 0.003), debt relief (E2) demonstrated a significant negative association (coefficient = −0.783; p = 0.003). This divergence suggests that while direct income support may have inadvertently increased exposure risk, potentially by facilitating higher residential density during lockdown periods, debt relief appeared to mitigate risk through different behavioral or socioeconomic pathways. Principal Component Analysis confirmed that these economic variables, alongside policies dedicated to the protection of elderly populations (H8), shaped the vast majority of the variance in SCC disease patterns. Despite these fluctuations, the overall burden remained significantly lower than in LSCC settings, with the highest-incidence cluster averaging only 2,907 cases per month (Figure 2).
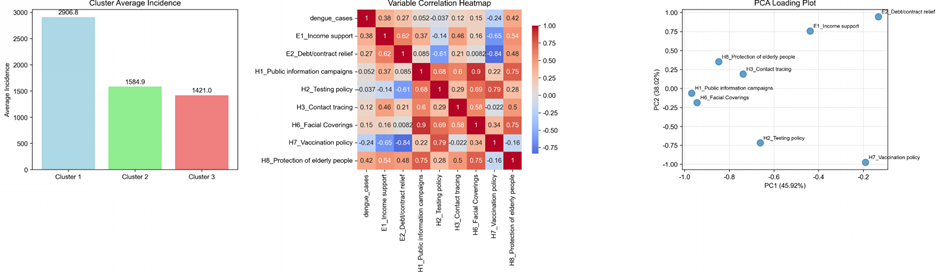
Figure 2: Correlation analysis for covariates in Strict COVID Control (SCC) countries.
Policy Impacts in LSCC Countries
In the LSCC group, health-related policy interventions emerged as the most potent drivers of reduced dengue incidence. Statistical modeling demonstrated that public information campaigns (H1) had the most significant protective effect, yielding a substantial negative association with case numbers characterized by a coefficient of −174,354 (p < 0.001). This finding was further reinforced by the Principal Component Analysis, which identified health communication and vaccination policy (H7) as the primary variables driving the first component of variance for this group. Furthermore, both vaccination policies and facial covering mandates (H6; p = 0.022) served as significant mitigating factors. In contrast to these health system measures, economic interventions in LSCC countries played a negligible role; income support (E1) showed only a marginally positive association with case numbers (p = 0.095), suggesting that financial aid did not substantially alter the epidemiological trajectory in these higher-burden regions. The scale of transmission in these settings was underscored by cluster analysis, which identified a high-burden pattern averaging 880,880.5 cases per month (Figure 3).
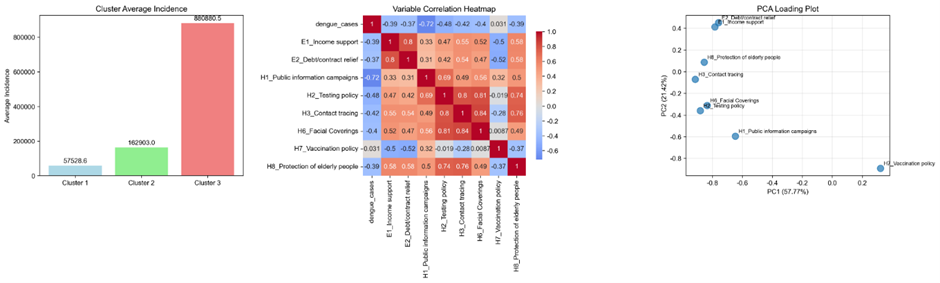
Figure 3: Correlation analysis for Less Strict COVID Control (LSCC) countries.
Multivariate Validation and Model Robustness
Principal Component Analysis confirmed the divergent nature of these policy environments, identifying that three components captured over 90% of the variance across both groups. These findings are supported by a generalized linear model framework that incorporated a one-month lag to reflect mosquito development and disease incubation cycles. The models exhibited high statistical power (≥ 0.85) and large effect sizes (Cohen’s f² ≥ 0.60), with significance levels maintained at p ≤ 0.05. Model diagnostics indicated robust performance, as residuals in SCC models passed all standard checks for homoskedasticity and autocorrelation, while the LSCC models remained stable overall despite exhibiting mild heteroskedasticity.
Discussion
The empirical evidence presented in this study reveals a complex socioeconomic paradox, particularly regarding the role of government support measures within Strict COVID-Control (SCC) frameworks. A primary finding is the divergent influence of income support and debt relief on dengue transmission. While direct income support was positively associated with increased dengue risk, debt relief functioned as a significant protective factor. This phenomenon is likely attributable to shifts in human-vector contact patterns; in jurisdictions like Singapore and China, robust income support likely facilitated high compliance with stay-at-home mandates. In these contexts, income support often involved direct cash transfers which, while alleviating financial strain, may have inadvertently increased residential density by encouraging populations to remain in domestic environments. Because Aedes aegypti is a highly anthropophilic vector that thrives in indoor, peri domestic environments, prolonged residential confinement may have intensified exposure to mosquito biting. This interpretation aligns with previous modelling studies which documented that mobility restrictions significantly reshaped the transmission dynamics of various infectious diseases during early lockdown phases.
Furthermore, the analysis suggests the presence of substantial institutional legacies from COVID-19 health policies in Less Strict COVID-Control (LSCC) nations. Public information campaigns and vaccination policies emerged as the most robust predictors of attenuated dengue transmission in these settings. This indicates that the public health infrastructure mobilized during the pandemic, including digital communication networks and centralized surveillance systems, may have conferred secondary benefits by enhancing community health literacy and promoting early medical-seeking behavior. In endemic regions such as Brazil and Indonesia, the heightened public sensitivity to febrile symptoms likely provided a transient defense against dengue resurgence. These findings align with recent scholarship suggesting that the strengthening of diagnostic and surveillance systems during the pandemic can be leveraged to improve the management of other endemic febrile illnesses. This argues for the strategic integration of pandemic preparedness frameworks with existing vector-borne disease control programs, as the institutional gains from one crisis can be utilized to fortify defenses against another.
One of the more unexpected results was the significant negative association between facial covering mandates and dengue incidence in LSCC settings. Although surgical or fabric masks offer no direct biological protection against the Aedes mosquito, this variable likely serves as a proxy for a broader suite of behavioral adaptations. Masking mandates often coincided with reduced social clustering and restricted occupancy of high-traffic public areas, such as transport hubs and urban plazas, which are recognized foci for dengue transmission. This "proxy effect" underscores a fundamental challenge in policy-based epidemiological modeling: a single regulatory index often encapsulates a complex array of unobserved behavioral shifts. Consequently, future research should incorporate high-resolution mobility and land-use data to further disentangle whether these protective effects are a result of specific policies or general risk-aversion behaviors that characterized the pandemic era.
While the statistical models employed demonstrate high robustness, several limitations warrant consideration. Most notably, the primary focus on policy indices at a national level may obscure critical sub-national variations in policy implementation and disease burden, particularly in geographically vast countries like Brazil. Furthermore, while our framework explicitly incorporated country-level climate controls, including monthly mean temperature and seasonal rainfall patterns derived from ERA5 datasets, to offset the impact of environmental confounding variables, localized microclimates and urban heat islands continue to be primary drivers of vector abundance that are difficult to capture at a macro scale. Additionally, the potential for under-reporting during periods of healthcare system strain remains a factor, as care-seeking behavior and diagnostic capacity fluctuated significantly during the pandemic peaks. Acknowledging these constraints does not diminish the validity of the identified policy-disease links; rather, it highlights the necessity for future iterations of this research to synthesize meteorological offsets with more granular, sub-national policy trackers to offer a truly comprehensive understanding of the post-pandemic dengue landscape.
Conclusion
This multi-country analysis demonstrated that COVID-19 control policies exerted collateral impact on the case number of dengue, with effects mediated by governance strictness and public awareness. In LSCC countries, health communication and vaccination policy proved most protective, while in SCC countries, economic measures shaped the resurgence of dengue. To prevent the post-pandemic resurgence of endemic diseases, LSCC countries should institutionalize scalable information and vaccination campaigns, while SCC countries should strengthen localized and data-driven interventions. Future work should integrate fine-grained climate and mobility data. This study contributes to post-pandemic epidemiology by offering one of the first comparative assessments of COVID-19 policy spill overs on dengue, providing evidence-based guidance for epidemic preparedness.
Acknowledgements
Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability
Data will be made available on request.
Highlights
- Dengue cases fell 41% during early COVID-19 lockdowns across seven countries.
- Pandemic policies left lasting, uneven effects on post-COVID dengue resurgence.
- Public awareness and vaccination efforts lowered dengue risk in less strict settings.
- Economic measures showed mixed effect on dengue risk in strict control countries.
- Integrating communication and vector control is key for future pandemic resilience.
References
- World Health Organization (2025) Dengue and severe dengue: Key facts.
- Wilke ABB, Beier JC, Benelli G (2019) Complexity of the relationship between global warming and urbanization – an obscure future for predicting increases in vector-borne infectious diseases. Curr Opin Insect Sci 35: 1-9.
- Groves HE, Piché-Renaud PP, Peci A, Farrar DS, Buckrell S, et al. (2021) The impact of the COVID-19 pandemic on influenza, respiratory syncytial virus, and other seasonal respiratory virus circulation in Canada: A population-based study. Lancet Reg Health Am 1: 100015.
- Hogan AB, Jewell BL, Sherrard-Smith E, Vesga JF, Watson OJ, et al. (2020) Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob Health 8: e1132-e1141.
- Araújo JLB, Bomfim R, Sampaio Filho CIN, Cavalcanti LPG, Lima Neto AS, et al. (2024) The impact of COVID-19 mobility restrictions on dengue transmission in urban areas. PLoS Negl Trop Dis 18: e0012644.
- Chen Y, Li N, Lourenço J, Wang L, Cazelles B, et al. (2022) Measuring the effects of COVID-19-related disruption on dengue transmission in southeast Asia and Latin America: A statistical modelling study. Lancet Infect Dis 22: 657-667.
- Weng SL, Hung FY, Li ST, Liou BH, Yeung CY, et al. (2025) Dengue Epidemiology in 7 Southeast Asian Countries: 24-Year, Retrospective, Multicountry Ecological Study. Interact J Med Res 14: e70491.
- Hale T, Angrist N, Goldszmidt R, Kira B, Petherick A, et al. (2021) A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav 5: 529-538.
- OpenDengue (2024) Global dengue case data. The Dengue Mapping and Modelling Group.
- Hersbach H, Bell B, Berrisford P, Biavati G, Horányi A, et al. (2023) ERA5 hourly data on single levels from 1940 to present. Copernicus Climate Change Service (C3S) Climate Data Store (CDS).
- Islam S, Haque CE, Hossain S, Hanesiak J (2021) Climate Variability, Dengue Vector Abundance and Dengue Fever Cases in Dhaka, Bangladesh: A Time-Series Study. Atmosphere 12: 905.
- Brauner JM, Mindermann S, Sharma M, Johnston D, Salvatier J, et al. (2021) Inferring the effectiveness of government interventions against COVID-19. Science 371: eabd9338.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.