Immediate Postoperative Arm Loading After Triceps Tendon Reconstruction in A Wheelchair-Bound Patient: A Case Report
by Markus Klingenberg*
Beta Klinik, Joseph-Schumpeter-Allee 15, 53227 Bonn, Germany
*Corresponding author: Markus Klingenberg, Beta Klinik, Joseph-Schumpeter-Allee 15, 53227 Bonn, Germany
Received Date: 26 December2024
Accepted Date: 30 December 2024
Published Date: 02 January 2025
Citation: Klingenberg M (2024) Immediate Postoperative Arm Loading After Triceps Tendon Reconstruction in A Wheelchair-Bound Patient: A Case Report. J Surg 9: 11222 https://doi.org/10.29011/2575-9760.011222
Abstract
Rupture of the triceps tendon is one of the rarest tendon ruptures. They account for less than 1% of all tendon and muscle injuries, with an estimated incidence of around 1.1 per 100,000 person-years in the general population. The most common causes are eccentric loads, such as a fall on the outstretched arm or strength training. A (sub)total rupture usually requires surgical repair in order to prevent permanent loss of strength and ensure the affected arm remains functional. Various surgical techniques with good biomechanical and clinical results are currently available. What they all have in common is the recommendation to immobilise the operated arm with a splint for six weeks after surgery. The permitted range of motion is usually gradually increased during this time. In this case report, the subtotal triceps tendon rupture of a 78-year-old wheelchair user was surgically treated using a modified anchoring technique in such a way that the arm could be loaded immediately after the operation. It was possible to prevent the patient from needing care due to immobilisation. The arm could be moved freely at all times. This case report describes the modified surgical technique using suture tapes and several bioresorbable anchors. In combination with intraoperative orthobiological support and an optimised post-treatment regimen, direct weight-bearing with free movement of the operated arm in everyday life was made possible. This post-operative treatment differs significantly from the regimens described in the literature. The patient was symptom-free throughout post-operatively.
Introduction
A 78-year-old male patient (DOB 06/11/1946), who is paraplegic following an accident in his youth, experienced extremely severe, locking pain in his left elbow during a typical everyday movement, pushing up from his wheelchair. In the days before, the patient himself had noticed pain-free swelling in the elbow area. Previous illnesses included arterial hypertension, which was well controlled with medication, and osteoarthritis of both hand and finger joints on both sides. The initial clinical examination revealed a pronounced haematoma on the left and a proximally thickened muscle belly of the triceps brachii muscle. A dent was palpable directly on the olecranon in the area of the triceps insertion. The strength of the left arm in extension was significantly reduced in various arm positions, but not completely eliminated. The loss of strength was most pronounced during the extension test against resistance in the overhead position.
Ultrasound revealed a largely ruptured and retracted triceps tendon. In addition, there was pronounced olecranon bursitis with multiple calcifications. MRI imaging of the elbow was performed to confirm the diagnosis. This confirmed the suspicion of a triceps rupture. The caput lateral and the caput longum were completely ruptured and retracted proximally. The medial caput still showed continuity, albeit very thin.
The therapeutic options were discussed in great detail. In order to avoid long-term nursing support, I urgently recommended that the patient undergo surgical reconstruction of the tendon. The patient did not agree to the usual six-week follow-up treatment after tendon reconstruction of the triceps with limited mobility and resilience. The challenge was therefore to choose a surgical technique and postoperative treatment that would allow immediate weight-bearing on the operated arm and allow for a temporary need for care. An operation date could be scheduled 12 days after the tendon rupture.
Materials & Methods
The operation was performed in the prone position with endotracheal intubation. The upper arm was positioned in 90 degree abduction with the forearm hanging down. A curved incision was made over the olecranon. An effusion of the olecranon bursitis was discharged. A sample was sent for microbiological examination for germs. The result was without pathological findings over time. Several small calcifications were removed. The ruptured tendon was examined. A haematoma located in the organisation was drained. As shown on the preoperative MRI image in Figure 1, a small part of the triceps tendon, the medial caput, was still present. Two calcified concretions were removed via a longitudinal incision of the medial caput. The ruptured parts of the tendon and the tendon insertion at the olecranon were debrided. A tissue sample was sent for histological examination. The ruptured reinforcement of the retracted triceps tendon was carried out transversely to the course of the tendon in healthy tissue, approx. 5 cm away from the rupture. Suture tape (Arthrex) and a long straight needle are used (Figures 2,3). The degenerated tendon (caput mediale) is reinforced in the same way with a labral tape (Arthex). In addition, a further suture tape is used as a U-suture proximal to the reinforcement of the ruptured tendon parts for additional securing (Figure 4).
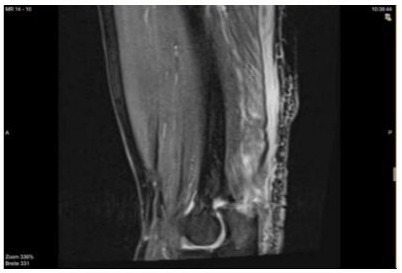
Figure 1: MRI pre-operative.

Figure 2: The post-traumatic ultrasound shows the ruptured and retracted triceps tendon.

Figure 3: Rupture of the triceps tendon.
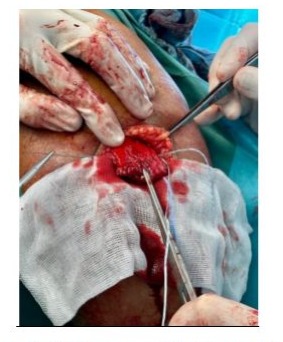
Figure 4: Reinforcement of the triceps tendon.
Knotless, absorbable Swivelock anchors (Arthrex) are used to secure the tendon parts. The securing labral tape of the caput mediale is fixed crossed in the olcranon with two 3.5 mm bioresorbable Swivelock anchors at 90 degrees to the course of the tendon. The elbow is held in approx. 70° flexion. Next, with the elbow in extension, the suture tape from step one is fixed further distally with two 4.75 mm Swivelock anchors (Arthrex) placed in parallel at a distance of approx. 1 cm. Finally, the securing suture tape of the U-suture is fixed further distally in the ulna with a third 4.75 mm Swivelock anchor. At the end of the fixation, the triceps tendon covered the anatomical attachment to the olecranon. After completion of the fixation, the surgical site is irrigated (Figures 5,6). To support healing, the patient’s own thrombin and autologous conditioned plasma (ACP) are injected into the ruptured tendon in the attachment area on the olecranon. Blood was taken from the patient during the operation for this purpose. ACP syringes (Arthrex), a thrombinator (Arthrex) and a Hettrich centrifuge were used. The wound was closed with the elbow bent at 90 degrees using the back-stitch technique. Steri Strips were also used and the elbow was wrapped with padding. A drain was not inserted as the operation was performed without a tourniquet.

Figure 5: Final reconstruction of the triceps tendon.
The inpatient stay lasted three days. The patient was able to carefully put weight on the arm from the first day after the operation. The patient felt pain on the day of the operation itself and on the first day after the operation. Afterwards, the pain level on the visual analogue scale (VAS) was 0-1 at rest and during exercise. The muscles of the shoulder-neck region and the upper arm were moderately activated and trained with EMS training and Kaatsu (blood flow restriction) on the second day after the operation. Care was taken to ensure a high fluid intake orally and with 1,000 ml Ringer i.v. during the first two days after the operation. A ten-minute induction therapy (BTL, programme: post-operative healing) was carried out three times post-operatively
Results and Discussion
The healing process after surgical fixation of the triceps tendon was unremarkable. The stitches were removed in two stages after 10 and 14 days. Healing of the wound directly at the olecranon took a few days longer. The microbiological findings of the olecranon bursitis were without pathological findings. The histological examination of the ruptured parts of the tendon showed a degeneration of the tendon with accompanying calcifications that had probably been present for some time. The operated arm could be used continuously in everyday life. This applies in particular to locomotion in a wheelchair and moving between the wheelchair and bed or toilet. The mobility of the arm in extension/flexion was 0-0-125° throughout and thus corresponded to the healthy opposite side.
At the beginning of the third week after the operation, the arm was mobilised several times a week with low resistance using a hand ergometer. Kaatsu training (blood flow restriction training) was carried out using the arm’s own weight. Regular ultrasound checks in the first three weeks still showed increased fluid in the attachment area of the triceps tendon. No loosening of the Swivelock anchors on ultrasound. Supplementary dumbbell training was introduced from the seventh week after the operation. Three months after surgical reconstruction of the triceps tendon, the triceps tendon appeared continuous and free of irritation on ultrasound. The weight-bearing capacity of the operated arm in everyday life was restored without restriction. The literature on the surgical treatment of a triceps tendon rupture is limited. Surgical treatment is indicated for complete ruptures and partial lesions with a relevant strength deficit. Men are affected twice as often as women. General risk factors include the use of cortisone, anabolic steroids, internal diseases such as chronic renal failure, hyperparathyroidism, type 1 diabetes, Marfan syndrome, rheumatoid diseases and osteoenesis imperfecta [1-3].
Prompt treatment within the first three weeks is recommended. Various surgical methods are described [2]. Transosseous and anchor-based fixations are described most frequently. In their review of 560 patients, [4] describe an overall complication rate of 14.9% for all repair techniques. Fixation with suture anchors led to fewer complications (7.7%) than fixation using transosseous sutures (15.2%). There were more reruptures (4.3% to 2.1%) and reoperations (3.6% to 1.3%) with transosseous sutures than with the suture anchor technique [4]. When using anchors, attention should be paid to the size and drilling direction to avoid transosseous injury to the joint. Postoperative complications include secondary olecranon bursitis and a persistent flexion deficit of up to 20%. The re-rupture rate is low at 6% and is usually associated with retrauma. [5] Overall, good postoperative results are described. Up to 89% of patients were able to return to their pre-traumatic activity level [1]. To date, there have only been a few studies investigating the use of PRP in triceps pathologies [6].
The post-treatment recommendations vary considerably. What they have in common is an average duration of immobilisation or restriction of mobility over a period of six weeks. [7] In some cases, flexion is limited to 20° flexion; in others, flexion is limited to 90° flexion. [8] Due to these generally restrictive post-treatment regimens, there are currently no relevant studies available that describe the accompanying orthobiological and physical therapy measures described here. I have successfully used the surgical technique described here for rupture of a triceps tendon in conjunction with an optimised post-treatment regimen three times in the last 18 months. Two of the patients were able to take relative weight off their operated arm because, unlike in the case described here, they were not in a wheelchair and did not require walking aids.
Conclusions
In the individual case described, rupture-remote multiple reinforcement transverse to the fibre course of the triceps tendon together with distal fixation of the tendon with knotless anchors enables sufficient stability for immediate postoperative weightbearing of the operated arm. Temporary dependency of the patient could be avoided. An optimised post-treatment regimen and close patient management are essential components of this therapeutic approach. Typically for a case report, no general standard of care can be derived from the procedure described here. Of interest is the fundamental possibility of immediate postoperative weight-bearing after reconstruction of a torn triceps tendon. The possibilities of supportive orthobiological concomitant therapy with regenerative therapy approaches such as PRP, SVF and the optimisation of physiotherapeutic follow-up treatment should be investigated in further studies.
References
- Dunn JC, Kusnezov N, Fares A (2017) Triceps tendon ruptures: a systematic review. Hand 12: 431-438.
- Freislederer F, Papillo D, Glanzmann M, Scheibel M (2020) Distale Bizepssehnen- und Trizepssehnenrupturen. Z Orthop Unfall 158: 663682.
- Yeh PC, Dodds SD, Smart LR, Mazzocca AD, Sethi PM (2010) Distal triceps rupture. J Am Acad Orthop Surg 18: 31-40.
- Alnaji O, Erdogan S, Shanmugaraj A (2022) The surgical management of distal triceps tendon ruptures: a systematic review. Journal of shoulder and elbow surgery 31: 217-224.
- Donaldson O, Vannet N, Gosens T, Kulkarni R (2014) Tendinopathies around the elbow part 2: medial elbow, distal biceps and triceps tendinopathies. Shoulder Elbow 6: 47-56.
- Kwapisz A, Prabhakar S, Compagnoni R, Sibilska A, Randelli P (2018) Platelet-rich plasma for elbow pathologies: a descriptive review of current literature. Curr Rev Musculoskelet Med 11: 598-606.
- Ritsch M, Regauer M, Schoch C (2022) Operative Therapie der distalen Trizepssehnenruptur. Oper Orthop Traumatol 2022.
- Lacheta L, Scheiderer B, Imhoff AB, Siebenlist S (2018) Trizepssehnenruptur und -insuffizienz. OUP 7: 325-329.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.