Hypertriglyceridemia and Hypercholesterolemia in Newly Diagnosed Type 1 Diabetes
by Lucija Oršulić1*, Katarina Brzica2, Sara Šabašov3, Ivana Unić2
1Split-Dalmatia County Health Center, Kavanjinova 2, 21000 Split, Croatia
2University Hospital of Split, Department of Paediatrics, Spinčićeva 1, 21000 Split, Croatia
3University of Split, School of Medicine, Šoltanska 2, 21000 Split, Croatia
*Corresponding author: Lucija Oršulić, Split-Dalmatia County Health Center, Kavanjinova 2, 21000 Split, Croatia
Received Date: 02 December 2024
Accepted Date: 06 December 2024
Published Date: 09 December 2024
Citation: Orsulic L, Brzica K, Sabasov S, Unic I (2024) Hypertriglyceridemia and Hypercholesterolemia in Newly Diagnosed Type 1 Diabetes. Ann Case Report. 9: 2104. https://doi.org/10.29011/2574-7754.102104
Abstract
Diabetes mellitus type 1 (DMT1) is one of the most common chronic diseases in children and diabetic ketoacidosis (DKA) occurs in 33.33% of newly diagnosed cases. Due to the lack of insulin, lipolysis occurs, which causes mild to moderate increase in the level of serum lipids.
We present a 9-year-old girl who was admitted to the University Hospital of Split in May 2023 due to newly discovered DMT1 presented with nocturia, polydipsia and polyphagia. She was healthy until now, her mother has Hashimoto's thyroiditis, her mother's father has type 2 diabetes. When admitted, she was of proportionally normal height and weight, slightly dehydrated with a discrete diffuse popular rash. In the initial laboratory findings, ketoacidosis (pH 7.32, HCO3- 13.1 mmol/L), ketonaemia (5.4 mmol/L) were observed, so parenteral rehydration and insulin administration were started. A few hours after the start of the treatment, from laboratory results we distinguish high HbA1c (17.1%, n<6) and extremely high values of total cholesterol (15.4, n<4.7 mmol/L), triglycerides (120.3, n<1.7 mmol/L), HDL-cholesterol (0.1 mmol/L) and LDL-cholesterol (2.64 mmol/L). It took 24 hours from the start of treatment until the complete normalization of glycemia, cholesterol levels, regression of the described skin changes that resemble the eruptive xanthomatosis. Triglyceride level normalized in the following days.
Hypertriglyceridemia and hypercholesterolemia are present in 50% of patients with DKA, while extremely high values are rare. Therapy with insulin analogs is usually sufficient, but other medications can also be used. Our patient’s symptoms were successfully resolved with parenteral rehydration and insulin therapy.
Keywords: Diabetes Mellitus; Hypertriglyceridemia; Hypercholesterolemia; Diabetic Ketoacidosis; Eruptive Xanthomatosis.
Introduction
Diabetes is one of the most common chronic diseases in children. About 100 new patients are diagnosed in Croatia annually and its frequency is increasing in Croatia as well as in the world, although the cause of this phenomenon is not yet fully known [1]. In diabetes mellitus type 1, lack of insulin is the trigger that initiates a whole series of pathophysiological processes, and in patients, it often presents with the classical signs and symptoms of polyuria, polydipsia, polyphagia, weight loss, and even 33.33% of patients with newly diagnosed DMT1 manifest with the clinical picture of DKA [2]. Due to the lack of insulin, glucose cannot enter the cell, and the energy deficit is compensated by increased lipolysis. In rare cases, lipolysis can cause an extreme increase in serum lipid values, as in the case of our patient [3,4].
Case Report
A nine-year-old girl was admitted to the University Hospital of Split, Department of Paediatrics due to suspected diabetes. Heteroanamnesis revealed that 4-5 days before admission to the University Hospital, she was urinating and drinking more than usual, but she did not lose weight. Also, in the same period, she became more tired and sleepy than before, and for the last ten days, she has also been irritable. Two weeks before admission, she had an acute digestive disorder in the form of several watery stools for 2-3 days, but the conditions regressed on their own. Anamnestically, she states that she has had nocturia for the past twenty days, 7-8 times per night. She has not been seriously ill so far. She has normal psychomotor development, plays sports, tolerates physical exertion well, and is an excellent student. The family history reveals that the mother suffers from Hashimoto's thyroiditis, the father is overweight and has arterial hypertension and the maternal grandfather suffers from diabetes after recently recovering from SARS-CoV-2 infection. Other autoimmune diseases and hyperlipidemia are not present among family members. On admission, she was in good general condition, contactable, eupnoic, eucardiac, with an audible low, systolic murmur of an innocent character, of proportionally normal height (HSDS -1) and weight (BMI-SDS -0.12), cold and moist palms, mildly dehydrated with a discrete, diffuse popular rash over the body. Immediately upon admission, a diagnostic work-up was started. Immeasurably high glycemia and ketonemia (5.4 mmol/L) were identified, and mild ketoacidosis was observed in the acid-base status (pH 7.32, HCO3 13.1 mmol/L). Under the working diagnosis of DKA as part of the newly discovered DMT1, parenteral rehydration and subcutaneous insulin administration were introduced. A milky-white lipemic serum was observed (Figure 1) during blood sampling for laboratory results. A few hours after admission, other laboratory results arrived, among which we distinguish the high value of glycosylated hemoglobin HbA1c (17.1%, n < 6) and extremely high values of total cholesterol (15.4, n < 4.7 mmol/L), triglycerides (120.3, n < 1.7 mmol/L), HDL-cholesterol (0.1 mmol/L) and LDL-cholesterol (2.64 mmol/L). Although we initially decided on subcutaneous insulin administration because the girl was in good general condition, she was only in mild DKA, when the aforementioned biochemical laboratory results arrived, subcutaneous insulin substitution was replaced by parenteral. During the first nine hours of rehydration and insulin therapy, there was a gradual normalisation of glycemia and a significant reduction of all serum lipids, and it took 24 hours from the start of treatment until the complete normalization of glycemia, cholesterol levels, regression of the described skin changes that resemble the eruptive xanthomatosis, while the triglyceride level normalized in the following days of hospitalization. By checking laboratory results before hospital discharge, cholesterol (4.9 mmol/L) and triglycerides (0.8 mmol/L) were within the reference values (Graph 1). We also checked amylase and lipase levels due to the risk of developing pancreatitis, and clinical and laboratory results were unremarkable. During the hospitalization, a more extensive endocrinological work-up was performed due to the possible existence of accompanying autoimmune diseases that are often associated with diabetes, and there were slightly elevated autoimmune markers for autoimmune thyroiditis and celiac disease. The patient will be monitored on an outpatient basis, and further treatment will be planned depending on the follow-up findings and the clinical picture. Only mild inhomogeneity of the thyroid gland was observed on ultrasound, and there were no signs of fatty liver on the abdominal ultrasound despite high cholesterol and triglyceride values. Given that a low level of vitamin D was observed, oral supplementation was introduced. Due to the initial laboratory results of the lipid profile and the clinically audible systolic murmur, a cardiological workup was performed, which resulted in unremarkable results just as the results of the ophthalmological examination. During the stay, the girl's parents went through an educational program called the "Little School on Diabetes" to acquire theoretical knowledge and practical skills, to be able to properly administer prescribed diabetes therapy, as well as to recognize symptoms and conditions that would indicate possible complications of diabetes disease. Also, in order to confirm the working diagnosis of DMT1, a blood sample was sent to the Reference Centre to determine the level of IA-2, ICA, anti-GAD.

Figure 1: Venous blood sample in which serum lipemia was observed.
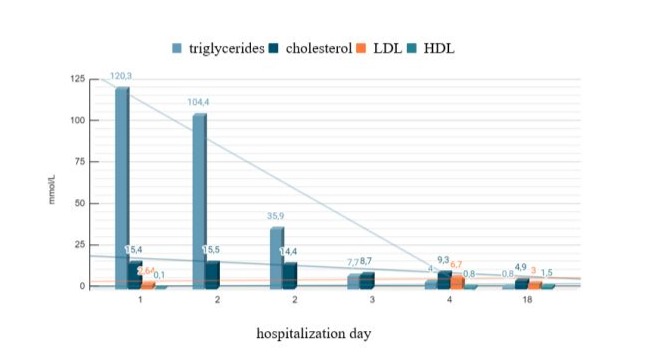
Graph 1: Lipid profile during hospitalization.
Discussion
This case report describes extremely rare complications of DMT1 and DKA which are hypertriglyceridemia and hypercholesterolemia. Accordingly, the available professional medical literature is relatively scarce with data from larger studies or systematic reviews, especially in the pediatric population. Given that the girl was in good general condition upon admission, and the anamnestic and heteroanamnestic data did not indicate extreme values in the received laboratory results, after studying the available literature and respecting the known pathophysiological mechanisms of DMT1, we decided to continue the therapy with insulin analogs, but parenterally instead of subcutaneously which turned out to be an excellent choice. According to information from the cases described so far, in addition to insulin therapy, other modalities such as fenofibrate, statins, niacin, omega-fatty acids, and plasmapheresis can also be used [5,6]. In our case, insulin therapy gave a quick and successful result, so there was no need for another therapy. In a patient with this clinical picture, it is important to take a detailed anamnesis of the possible existence of dyslipidemia among family members because there is a possibility of genetic dyslipidemia and a predisposition to it [3]. Although our patient had extremely high triglyceride and cholesterol values, pancreatitis did not occur, unlike some other cases described in the literature [3]. Likewise, during DKA with extreme hypertriglyceridemia, artifactual pseudohyponatremia can occur, which was not recorded in our case [6]. The described skin changes clinically correspond to eruptive xanthomatosis, which regressed as lipid profile values improved. This phenomenon has been described in several cases and was mostly of a benign nature [7,8]. It is interesting that in the available medical literature, there has been found only one other case of extremely elevated triglycerides in which, as in our case, pancreatitis did not occur. However, in this case, the aggravating circumstance was a diet with a very high content of saturated fatty acids [9]. Given that the presented patient had regular lifestyle habits, a balanced diet, relatively short disease symptoms, without a particularly burdensome family history of hyperlipidemia, the initial laboratory results were more than surprising, but due to early recognition and a good therapeutic response, there was a rapid normalisation of laboratory results.
Conclusion
Moderate and mild hypertriglyceridemia and hypercholesterolemia are present in 50% of patients with DKA, while extremely high values are very rare. According to a systematic review (PubMed/Medline), therapy with insulin analogs is usually sufficient to lower the level of serum lipids, but fenofibrate, statins, niacin, omega-fatty acids and plasmapheresis can also be used. In conclusion, we presented a 9-year-old girl with newly discovered DMT1 in a state of mild DKA with extreme hypertriglyceridemia and hypercholesterolemia, which were successfully and quickly resolved with parenteral rehydration and insulin therapy. By educating the girl and her family, a fundamental step was taken in the prevention of new complications of the underlying disease, which will be further monitored on an outpatient basis in accordance with the monitoring protocol of DMT1 and possible associated diseases.
Ethical Guidelines: We confirm that all the ethical guidelines and principles have been fully adhered to in the preparation of this case report.
Conflict of Interest: All authors declare that they have no conflicts of interest.
References
- Duško Mardešić (2016). Pedijatrija. 8th ed. Školska knjiga, 633–645.
- Stipancic, G, Sepec, M.P, Sabolic, L.L.G, Radica, A, Skrabic, V, et al (2011). Clinical characteristics at presentation of type 1 diabetes mellitus in children younger than 15 years in Croatia. Journal of Pediatric Endocrinology and Metabolism, 24.
- Zaher, F.Z, Boubagura, I, Rafi, S, Elmghari, G. and Elansari, N. (2019). Diabetic Ketoacidosis Revealing a Severe Hypertriglyceridemia and Acute Pancreatitis in Type 1 Diabetes Mellitus. Case Reports in Endocrinology, 2019:1–4.
- Ruiz Rebollo, M.L, García, C, Berrocal de la Fuente, C.A. and Toribio Calvo, B. (2023). The enigmatic triad, a clinical challenge. Revista Espanola De Enfermedades Digestivas, [online] 115:276–277.
- Hartz, J.C, de Ferranti, S. and Gidding, S. (2018). Hypertriglyceridemia in Diabetes Mellitus: Implications for Pediatric Care. Journal of the Endocrine Society, [online] 2:497–512.
- Ibrahim R, Salih M, Elmokdad C. and Sidhu, A. (2020). Diabetic Ketoacidosis, Very Severe Hypertriglyceridemia, and Pseudohyponatremia Successfully Managed with Insulin Infusion. Cureus, [online] 12:e9306.
- Zhao C. and Li H. (2023). Eruptive xanthoma associated with hypertriglyeridaemia and diabetes. 52:371–373.
- Lee, S.Y. and Sheth, C.A. (2019). Eruptive xanthoma associated with severe hypertriglyceridemia and poorly controlled type 1 diabetes mellitus. Journal of Community Hospital Internal Medicine Perspectives, [online] 9:344–346.
- Vitale, R.J. and Laffel, L.M.B. (2023). New-Onset Type 1 Diabetes in a Child with Diabetic Ketoacidosis and Severe Hypertriglyceridemia Without Pancreatitis. JCEM case reports, [online] 1: 046.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.