Fixation of a Spiral Femoral Shaft Fracture with Wedge Fragments (AO/OTA 32 B3.1) In an Adult Patient with Duchenne Dystrophy Using a Rigid Humerus Nail and Cable Cerclage
by Eren Demir, Charlotte Arand, Erik Wegner, Erol Gercek, Sven-Oliver Dietz*
Department of Orthopaedics and Traumatology, University Medical Center, Mainz, Germany
*Corresponding author: Sven-Oliver Dietz, Department of Orthopaedics and Traumatology, University Medical Center, Mainz, Germany
Received Date: 24 October 2024
Accepted Date: 28 October 2024
Published Date: 30 October 2024
Citation: Demir E, Arand C, Wegner E, Gercek E, Dietz SO (2024) Fixation of a Spiral Femoral Shaft Fracture with Wedge Fragments (AO/OTA 32 B3.1) In an Adult Patient with Duchenne Dystrophy Using a Rigid Humerus Nail and Cable Cerclage. Ann Case Report. 9: 2037. https://doi.org/10.29011/2574-7754.102037
Abstract
A 21-year-old male patient with Duchenne Dystrophy suffered an AO/OTA 32 B3.1 fracture of his left femur. Despite the femur`s anatomy, the fracture`s morphology and the patient`s weight (53.2kg) the osteosynthesis was performed using a rigid humerus nail. The fracture healed uneventfully after 12 weeks. The use of a rigid humeral nail is a suitable procedure for the treatment of type B femoral shaft fractures in patients with muscular dystrophy. This procedure should especially be considered if these patients have a body weight of more than 50 kilograms and in multifragmentary fractures.
Keywords: Femoral Fracture; Duchenne Dystrophy; Fracture Treatment; Nail Osteosynthesis.
Introduction
Patients with Duchenne Dystrophy develop osteoporosis due to increasing muscular weakness and loss of function [1]. These patients have a higher risk for fractures [2]. Even though femoral fractures are common in patients with Duchenne Dystrophy only few authors reported of fracture management in these patients [35]. Huber et al. and Brown et al. reported of fracture management of distal or femoral shaft fractures respectively using flexible intramedullary nails [4,5]. Biber et al. report of a series of 3 patients with distal supracondylar fractures treated by retrograde nailing using proximal humerus nails [3]. In this case report, we present an antegrade nail osteosynthesis of a proximal femoral shaft fracture using a rigid proximal humerus nail.
Case Presentation
We report of a 21-year-old male patient with a body weight of 53.2 kilograms who slid of his toilet chair hearing a crack in his left femur. The patient was sitting in a wheelchair for about 8 hours a day and studying at university. He was diagnosed a proximal femoral shaft fracture (AO/OTA 32 B3.1) in our emergency department (Figure 1a,b). The femoral shaft diameter was 10.2mm, the medullary canal 9.0mm. Due to the relevant dislocation of the fracture fragments, the shortening of the upper leg, the poor fracture localization for splinting and the massive pain, we saw an indication for urgent operative stabilization and the patient was immediately transferred to our OR. Despite the tiny intramedullary canal, we aimed for the highest possible stability to enable wheelchair transfer and the ability to sit for several hours. Due to the wedge fragments, flexible nailing of the fracture seemed not to be an adequate stabilization. The available rigid femoral nails had diameters of minimum 9.0mm. Considering the poor bone quality and thin cortical is, reaming of the medullary canal was not an option. As proximal humerus nails were used in femoral shaft fractures in children and adolescents before [6,7] we decided upon an 8.2mmx300mm T2 Proximal Humerus Nail (Stryker Howmedica, Mahwah, USA).
The patient was placed on a radiolucent table in supine position without traction. The operation was performed under spinal anesthesia. The dislocated proximal wedge fragment measured 7 x 1cm. We decided to fix this by means of a cable cerclage (Cable System, DePuySynthes, Oberdorf, Switzerland) in a minimal invasive technique without stripping the periosteum. A non-displaced wedge fragment was also fixed by means of a cable cerclage. Special attention was paid to bringing the nail in the exact longitudinal axis of the femoral shaft.Intraoperative fluoroscopy showed anatomic reduction and stable fixation (Figure 2a, b).
The length of hospital stay was 5 days. Bed-wheelchair transfers were possible from the first post-operative day. All wounds healed uneventfully.
Results
Ten days after surgery the patient resumed his studies at university. Due to the Corona pandemic all courses were held online. Nevertheless, he was able to sit in his wheelchair for at least 8 hours a day. After 12 weeks the fracture had healed (Figure 3a-d). The patient could be mobilized into a standing position.
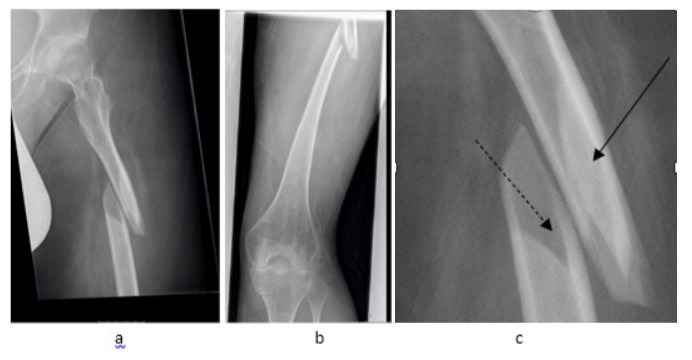
Figure 1a, b: Proximal femur fracture AO 32 B3.1 (composed X-ray, Figure. 1a). The detail view (Figure. 1b) depicts the displaced (solid line) and none displaced (broken line) wedge fragments.

Figure 2a and b: Postoperative x-rays of the left femur showing anatomical alignment in a.p. (Figure. 2a) and lateral (Figure 2b) views.

Figure 3a-d: Follow-up composed X-rays after 12 weeks. All cortices are bound by callus formation in a.p. (Figure. 3a,b) and lateral (Figure. 3c,d) views.
Discussion
Femoral fractures are frequent in patients with Duchenne Dystrophy. Nevertheless, recommendations for the treatment of these fractures are rare.Brown et al. [4] reported of intramedullary osteosyntheses with flexible nails in patients suffering from muscular dystrophies. In contrast to our patients theirs’s patient had a very low BMI (17.4) and the fracture was a simple spiral fracture (AO 32 A1). Two reasons held us from using flexible nails in our patient. Flexible nails are used for the stabilization of diaphyseal long bone fractures in children, but not for adults. The results of intramedullary nailing with flexible implants for femoral fractures in patients with a body weight of 50 kilograms or more are poor. In a mini-review Andreacchio et al. found a complication rate of 51.7% in these patients [8]. Moreover, elastic nailing cannot guarantee reliable fixation of unstable femoral shaft fractures with additional wedge fragments. Deakin et al. found malunions in all type B and C fractures of the femoral shaft treated by this technique [9]. On the other hand, rigid nailing of bones with poor bone quality includes risks. If the nail is not perfectly inserted into the axis of the femoral canal, there is a high risk of intraoperative fracture of the femoral shaft. This is particularly true when there is a mismatch between the curvature of the nail with the femur [10].
Proximal humerus nails have previously been used in pediatric and adolescent patients for the treatment of femoral pathologies [6,11]. Gordon et al. described femoral lengthening in nine children over a humeral intramedullary nail. The authors witnessed two operative fractures and one fracture after removal of the distal locking pin. Furthermore, two infections occurred. The infections were all due to the half-pins used for femoral lengthening and not to the humeral nail. One operative fracture was due to the half pins, another occurred after removal of the distal locking screw. One fracture developed through the distal locking site resulting in loss of reduction and nail replacement [11]. In a further paper of the same group, 15 children with femoral shaft fractures were treated by humeral nails [6]. No complications were found in these patients. Since our patient suffered from a femoral fracture, we were confident, that a rigid humeral nail might be a safe procedure. The additional cable cerclage was performed to restore the medullary canal before the nailing procedure was started. The callus bridge, which is clearly visible at 3 months, proves the vitality of the periosteum of the wedge fragment at the fracture site.
To our knowledge, this is the first report of the treatment of a femoral shaft fracture with wedge fragment treated with a rigid humeral nail in a patient with Duchenne Dystrophy. According to our findings and the sparse literature, we could show that the use of a rigid humeral nail is a suitable procedure for the treatment of type B femoral shaft fractures in patients with muscular dystrophy. This procedure should especially be considered if these patients have a body weight of more than 50 kilograms. Even though it is only a report of one case, our experience might help surgeons being faced with this rare pathology.
Ethical considerations: All personal identifiers have been removed from the case report’s figures and special care has been taken in the data contained in description of the case so that the patient cannot be identified. The patient was informed and agreed that data concerning his case is submitted for publication.
Conflict of interests: None.
References
- Apkon, S.D, Alman, B, Birnkrant, D.J, Fitch, R, Lark, R, et al (2018) Orthopedic and Surgical Management of the Patient with Duchenne Muscular Dystrophy. Pediatrics 142:S82–S89.
- King, W.M, Kissel, J.T, Visy, D, Goel, P.K, Matkovic, V (2014) Skeletal health in Duchenne dystrophy: Bone-size and subcranial dual-energy X-ray absorptiometry analyses. Muscle & Nerve 49: 512–519.
- Biber, R, Stedtfeld, H, Bail, H.J (2014) The Targon PH ® nail for distal femoral fracture fixation in disabled children. A report of three cases. Orthopaedics & Traumatology: Surgery & Research 100: 699–702.
- Brown, M.J, Song, K, Vollmar, M, Shelby, M, Leshikar, H (2019) Flexible Femoral Nailing of an Awake Adult Muscular Dystrophy. JAAOS Glob Res Rev 3: e19.00013.
- Huber, H, André, G, Rumeau, F, Journeau, P, Haumont, T, et al (2012) Flexible intramedullary nailing for distal femoral fractures in patients with myopathies. Journal of Children’s Orthopaedics 6, 119–123.
- Gordon, J.E, Khanna, N, Luhmann, S.J, Dobbs, M.B, Ortman, M.R, et al (2004) Intramedullary Nailing of Femoral Fractures in Children Through the Lateral Aspect of the Greater Trochanter Using a. J Orthop Trauma 18, 416–422.
- Keeler, K.A, Dart, B, Luhmann, S.J, Schoenecker, P.L, Ortman, M.R, et al (2009) Antegrade Intramedullary Nailing of Pediatric Femoral Fractures Using an Interlocking Pediatric Femoral Nail and a Lateral Trochanteric Entry Point. J Pediatr Orthop 29, 345–351.
- Andreacchio, A, Alberghina, F, Marengo, L, Canavese, F (2019) Pediatric tibia and femur fractures in patients weighing more than 50 kg (110 lb): mini review on current treatment options and outcome. MUSCULOSKELETAL SURGERY 103: 23–30.
- Deakin, D.E, Winter, H, Jain, P, Bache, C.E (2010) Malunion following flexible intramedullary nails for tibial and femoral fractures in adolescents. Journal of Children’s Orthopaedics 4: 571–577.
- Bong, M.R, Kummer, F.J, Koval, K.J, Egol, K.A (2007) Intramedullary nailing of the lower extremity: biomechanics and biology. The Journal of the American Academy of Orthopaedic Surgeons 15: 97–106.
- Gordon J.E, Goldfarb C.A, Luhmann S.J, Lyons D, Schoenecker P.L, (2002) Femoral Lengthening Over a Humeral Intramedullary Nail in preadolescent children. The Journal of Bone and Joint Surgery 84-A: 930–937.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.