FDG PET/CT in Detection of Involvement of the Heart and Adrenal Gland in a Patient Diagnosed with Testicular Diffuse Large B-Cell Lymphoma
by Efrah Ahmed Ibrahim*
Nuclear Medicine Resident Physician, Department of Nuclear Medicine, Uludag University Hospital, Bursa, Türkiye
*Corresponding author: Efrah Ahmed Ibrahim, Nuclear Medicine Resident Physician, Department of Nuclear Medicine, Uludag University Hospital, Bursa, Türkiye
Received Date: 19 December, 2024
Accepted Date: 30 December, 2024
Published Date: 06 January, 2025
Citation: Ibrahim EA (2025) FDG PET/CT in Detection of Involvement of the Heart and Adrenal Gland in a Patient Diagnosed with Testicular Diffuse Large B-Cell Lymphoma. J Nucl Med Radiol Imaging 4: 111. https://doi.org/10.29011/JNMRI-111.100011
Abstract
Diffuse Large B-Cell Lymphoma (DLBCL) is an aggressive subtype of Non-Hodgkin Lymphoma (NHL) that affects B-lymphocytes. Metastasis in testicular lymphoma frequently involves the contralateral testis, brain, lung, peritoneum, omentum, and bone. Rarely, cardiac metastases or bilateral adrenal gland involvement are reported, often remaining unrecognized until autopsy. This case study highlights the progression of DLBCL beyond the initial diagnosis of left testicular lymphoma. FDG-PET/CT, the gold standard imaging modality in lymphoma management, plays a pivotal role in staging and treatment planning. This report underscores its utility in identifying multifocal disease, cardiac involvement, and pulmonary manifestations that would otherwise be missed with CT alone. This case provides crucial insights into the activity status of DLBCL.
Keywords: Cardiac metastases; FDG-PET; DLBCL; Adrenal gland involvement.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most prevalent form of NHL globally, accounting for approximately 22% of newly diagnosed B-cell NHL cases in the United States, with over 18,000 cases annually [1]. This aggressive malignancy often metastasizes to the contralateral testis, brain, lung, peritoneum, omentum, and bone [1]. Cardiac metastases and bilateral adrenal gland involvement are exceedingly rare and underreported in the literature, with most cases diagnosed post-mortem. Secondary cardiac lymphomas are far more common than primary cardiac lymphomas, representing 5-20%
of disseminated lymphoma cases [2]. DLBCL accounts for 80% of cardiac lymphomas [2]. Retrospective studies highlight its prevalence among histologic subtypes, yet antemortem diagnosis remains challenging due to nonspecific clinical presentations.
Adrenal gland involvement, particularly extranodal, is reported in less than 1% of all NHL cases [9]. Most patients present with nonspecific symptoms such as B-symptoms, fatigue, or pain. Bilateral involvement occurs in approximately 70% of cases, with adrenal insufficiency observed in a significant proportion. Previous case reports have described testicular lymphoma with bilateral adrenal metastases but combined cardiac and adrenal gland involvement remains exceedingly rare.
Case Presentation
Patient Background
A 65-year-old male presented with a history of left testicular enlargement persisting for 2-3 years. The patient underwent a right orchiectomy after prostate surgery, with pathology revealing DLBCL of the non-germinal center B-cell phenotype. The procedure was conducted at Bandirma State Hospital, and pathology was processed at Ege University.
Clinical Presentation
At initial presentation, the patient exhibited systemic symptoms, including fever, chills, weight loss (from 90 kg to 75 kg in one month), night sweats, nausea, vomiting, and intermittent diarrhoea. No significant findings were noted on respiratory or abdominal examinations. Laboratory tests revealed anaemia (Hb 10.9 g/dL), mild renal dysfunction (creatinine 1.49 mg/dL), and elevated liver enzymes (AST 200 U/L, ALT 488 U/L).
Imaging Studies
Contrast-enhanced CT identified significant bilateral adrenal masses and hypermetabolic lesions consistent with metastasis.
FDG-PET/CT Procedure
The FDG-PET/CT study was conducted following a fasting period of six hours. Blood glucose levels were measured and confirmed to be below 120 mg/dL prior to the injection of 12.6 mCi (468 MBq) of F-18 FDG. Approximately 68 minutes post-injection, imaging was performed using a low-dose CT scan for attenuation correction, followed by PET data acquisition at two minutes per bed position. Imaging covered the skull base to the mid-thigh level.
FDG-PET/CT findings included (Figure 1):
- Head and Neck: No abnormal FDG uptake observed in lymph nodes.
- Thoracic Region: A hypermetabolic lymph node in the anterior pericardial region (SUVmax: 5.0).
- Cardiac lesions localized to the bilateral atrium, atrial septum, inferior vena cava, and left ventricle (largest lesion: 2.5 cm; SUVmax: 16.7).
- Scattered pulmonary lesions, with the largest measuring 17x11 mm (SUVmax: 16.3).
- Abdominal Region: Bilateral adrenal masses (right: 138x81 mm, left: 107x80 mm; SUVmax: 21.5).
- Hepatic metastases in the caudate lobe and segment 7, with the largest lesion measuring 72x59 mm (SUVmax: 17.6).
- Pelvic Region: No free fluid or pelvic lymphadenopathy observed.
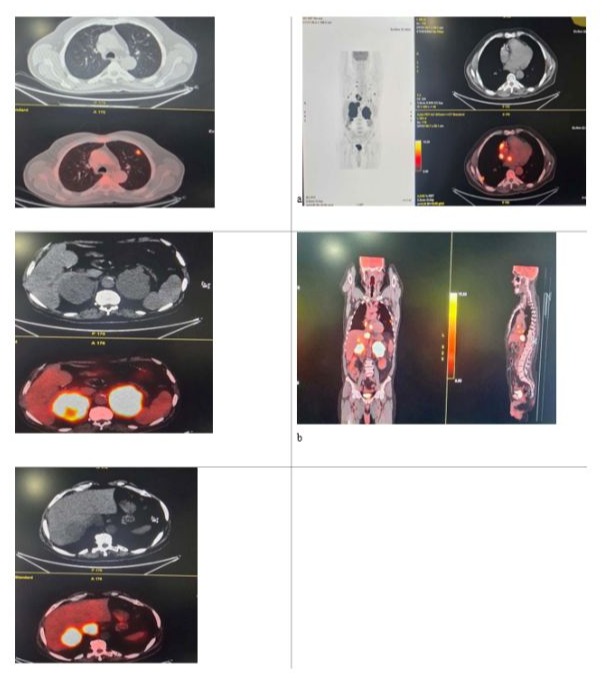
Figure 1: FDG -PET/CT Study. (a left) Maximum intensity projection showing intensely FDG-avid s tissue masses in both lungs, bilateral atrium, abdominal lymph nodes bilateral adrenal glands. (b) Sagittal fused PET/CT image showing the same findings as in (a) (a right) trans axial fused PET/CT image showing intensely FDG-av lesions in the right atrium and intra-atrial septum. (c) Parenchymal nodule in the left lung. (d) Massive lesions in both adrenal glands. (e) Focused uptake at the junction of the inferior vena cava and right atrium.
Additional Findings
Subsequent investigations were conducted following the FDG-PET/CT scan. The patient developed sudden bradycardia, with a heart rate ranging between 40 and 60 beats per minute, accompanied by syncope. A cardiology consultation was requested, and Transthoracic Echocardiography (TTE) was performed. The findings included normal left ventricular dimensions and wall movements, with an ejection fraction of 55%. Mild mitral regurgitation (grade 1) and tricuspid regurgitation (grade 1) were observed. Lesions identified in the right atrium and ventricle were evaluated, with differential diagnoses including interatrial lipomatous hypertrophy, metastases, and lymphoma. Additional lesions in the inferior vena cava raised the possibility of thrombus or lymphoma. No pericardial effusion was observed. The patient was started on the first cycle of Cyclophosphamide, Doxorubicin, Rituximab and Prednisolone.
Differential Diagnosis
Nodular lesions of the adrenal glands may result from:
- Metastatic Disease: Commonly from solid tumours such as lung, breast, or renal cancers, melanoma, and rarely, colon tumours.
- Primary Malignant Adrenal Disease: Includes lymphoma, pheochromocytoma, adrenocortical carcinoma, or neuroblastoma.
- Benign Conditions: Non-functioning or functioning adenomas, adrenal macronodular hyperplasia, or congenital adrenal hyperplasia.
- Infiltrative Causes: Amyloidosis.
- Infectious Causes: Tuberculosis, histoplasmosis, or cryptococcosis.
- Haemorrhagic Causes: Adrenal haemorrhage or infarction.
Discussion
Primary testicular lymphoma is a rare subtype of NHL, accounting for 1-2% of cases. The median age of affected patients aligns with this case (64 years). FDG-PET/CT offers superior sensitivity in detecting nodal and extra nodal lymphoma manifestations, as highlighted here. Unlike cardiac-specific PET imaging, conventional FDG-PET/CT reveals myocardial FDG uptake variations, necessitating further evaluation to avoid misdiagnoses.
Mechanisms of Extranodal Involvement
The adrenal glands and heart are rare sites of involvement in DLBCL. Adrenal involvement occurs in less than 1% of all NHL cases, often as part of systemic disease. Lymphatic dissemination, direct invasion, and hematogenous spread are the primary pathways for extranodal involvement. Cardiac metastases, on the other hand, may result from hematogenous dissemination or lymphatic spread.
Significance of PET/CT Imaging
FDG PET/CT plays a critical role in staging, treatment planning, and response evaluation in DLBCL [7]. It is particularly effective for identifying sites of extranodal involvement that might be missed by conventional imaging techniques. In this patient, PET/CT successfully highlighted hypermetabolic activity in the heart, lungs, liver, and adrenal glands, demonstrating the disease’s systemic extent. It is very rare to find adrenal and cardiac involvement in the same patient [8]. To our knowledge, this is the fourth case that has been reported:
- Case 1: A patient with malignant lymphoma infiltrating the right ventricle, tricuspid valve, interventricular septum, and left adrenal gland showed significant improvement with CHOP chemotherapy but later succumbed due to treatment refusal.
- Case 2: Another individual with cardiac lymphoma affecting the right atrium and right ventricle, along with bilateral adrenal gland involvement, achieved partial remission post-CHOP but deteriorated due to advanced progression.
- Case 3: Lucchini, et al. reported secondary cardiac lymphoma presenting as sick sinus syndrome. PET/CT imaging was instrumental in early detection and management.
Clinical Implications and Future Considerations
Given the rarity and complexity of combined adrenal and cardiac involvement in DLBCL, early and accurate detection is essential for optimizing patient outcomes. Multimodal imaging approaches, including PET/CT, echocardiography, and potentially cardiac MRI, are recommended for comprehensive assessment. Advanced imaging not only aids in accurate staging but also in monitoring therapeutic response, especially in patients undergoing chemotherapy regimens like CHOP. Additionally, further research into the molecular mechanisms underlying extranodal dissemination may provide insights into targeted therapies for these rare cases.
This report demonstrates the diagnostic superiority of combined PET/CT imaging, which provided critical information for staging and guiding treatment in this patient. The findings are consistent with existing literature emphasizing the rarity and clinical complexity of cardiac and adrenal gland involvement.
Conclusion
This case underscores the pivotal role of FDG-PET/CT in the comprehensive staging of DLBCL. It highlights the importance of recognizing rare extranodal manifestations, such as cardiac and adrenal involvement, to inform timely and effective treatment strategies. Early detection via advanced imaging modalities is crucial for improving patient outcomes.
Declarations
Disclosure Statement: The authors declare that they have no relevant financial or non-financial conflicts of interest that could directly or indirectly influence the content of this manuscript. No other potential conflicts of interest relevant to this article exist.
References
- Lymphoma Research Foundation. Understanding Lymphoma.
- Al-Mehisen R, Al-Mohaissen M, Yousef H (2019) Cardiac involvement in disseminated diffuse large B-cell lymphoma, successful management with chemotherapy dose reduction guided by cardiac imaging: A case report and review of literature. World J Clin Cases 7: 191-202.
- Lokesh KN, Sathyanarayanan V, Kuntegowdanahalli CL, Suresh TM, Dasappa L, et al. (2014) Primary diffuse large B-cell lymphoma of testis: A single centre experience and review of literature. Urol Ann 6: 231-234.
- Clemens JQ, Pins M (2000) Non-Hodgkin’s lymphoma presenting as bilateral testicular and adrenal masses. J Urol 163: 241-242.
- Metser U, Goor O, Lerman H, Naparstek E, Even-Sapir E (2004) PET-CT of extranodal lymphoma. AJR Am J Roentgenol 182: 1579-1586.
- Mane S, Phatak S, Dhok A, Shaikh AS (2023) Primary testicular non-Hodgkin’s lymphoma with bilateral adrenal metastasis: A rare presentation. Cureus 15: e43766.
- Agrawal K, Mittal BR, Manohar K, Kashyap R, Bhattacharya A, et al. (2012) FDG PET/CT in Detection of Metastatic Involvement of Heart and Treatment Monitoring in Non-Hodgkin's Lymphoma. World J Nucl Med 11: 33-34.
- Lucchini E, Merlo M, Ballerini M, Porcari A, Sinagra G, et al. (2021) Cardiac involvement by lymphoma: Rare but heterogeneous condition with challenging behaviors. Front Oncol 11: 665736.
- Rashidi A, Fisher SI (2013) Primary adrenal lymphoma: a systematic review. Ann Hematol 92: 1583-1593.
- O'Mahony D, Peikarz RL, Bandettini WP, Arai AE, Wilson WH, et al. (2008) Cardiac involvement with lymphoma: A review of the literature. Clin Lymphoma Myeloma 8: 249-252.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.