Evaluation and Treatment of Recurrent Metastatic Breast Cancer: A Case Report
by Anwar Alroubaie
Canadian Specialist Hospital, Dubai, UAE
*Corresponding author: Anwar Alroubaie, Canadian Specialist Hospital, Dubai, UAE
Received Date: 24 February, 2026
Accepted Date: 06 March, 2026
Published Date: 09 March, 2026
Citation: Alroubaie A (2026) Evaluation and Treatment of Recurrent Metastatic Breast Cancer: A Case Report. J Oncol Res Ther 11: 10333. DOI: https://doi.org/10.29011/2574-710X.10333
Abstract
Background: Breast cancer a most common cancer, has a large impact on global cancer morbidity. A 45-year-old female patient underwent a simple mastectomy for carcinoma of the left breast in the year 2020. She did not follow up further with the oncologist. In July 2023, she presented in the emergency department with severe left axillary and chest pain, uncontrolled hypertension, and shortness of breath with desaturation. She was hospitalized, treated intensively, and stabilized. The subject was started on the biological targeted therapy a cyclin-dependent kinase (CDK) inhibitor 4 and 6 (CDK inhibitors 4/6) abemaciclib in combination with hormone therapy of letrozole, and goserelin, along with bone support agent zoledronic acid. After three cycles, the local axillary mass was reduced by more than 50%, the respiratory function became normal, and there was no more chest or axillary pain. After cycle 5, the local mass almost disappeared along with the bone pain. The subject was continued on the same treatment. Presently the patient has a stable disease, showing excellent treatment response without any chemotherapy and experiencing a better quality of life. Metastatic breast cancer (MBC) does not always require chemotherapy for disease regression. Endocrine therapy combined with adjuvant CDK 4/6 inhibitors tailored as per the patient’s preference can play a crucial role in extending overall survival in patients with MBC.
Key-words: Metastatic Breast Cancer; Hormonal Treatment; Metastasis; Case Report; Patient Preference; Patient Participation; Endocrine Therapy;
Introduction
Breast cancer is the most common cancer worldwide, with over 2.3 million new cases and 685,000 deaths in 2020 [1]. It continues to have a large impact on the global number of cancer deaths.1 To date, a number of factors with prognostic significance in early-stage breast cancer have been established, including age, race, tumor size, nodal status, histologic grade, estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor-2 (HER-2) status, with the axillary nodal status being arguably the most significant prognostic indicator [2]. The incidence rate of metastatic female breast cancer was 5.8 per 100,000 in 2001 and increased to 7.9 per 100,000 in 2021 [3]. Breast cancer is commonly treated by various combinations of surgery, radiation, chemo-, and hormone therapy according to disease and patient factors. Over the past four decades, systemic therapy with endocrine therapy or cytotoxic chemotherapy became the fundamental treatment approach for the management of metastatic breast cancer [4].
The responsibilities of an oncologist or expert healthcare professional extend beyond diagnosis and treatment planning. They also include providing patient counseling and engaging in dialogue with the patient to comprehend their preferences in treatment planning to ensure good treatment adherence and outcomes. Current guidelines recommend frequent follow-up visits to evaluate for new primary cancers, recurrence, and treatment side-effects [5].
For the success of any treatment patient’s active involvement in decision-making to planning, to achieve the treatment target is essential. Studies showed that women experiencing active involvement in treatment decisions for breast cancer reported a significantly higher quality of life than women experiencing passive involvement [6].
We present a case report of a patient with a simple mastectomy for carcinoma of the left breast, who presented in critical condition in the emergency department. She was diagnosed with recurrence and metastasis. The patient was successfully stabilized without using chemotherapy as per her wishes.
Case Description
A 45-year-old female patient was diagnosed with carcinoma of the left breast (T2N0M0) which was positive for hormone receptors but negative for HER-2, in the year 2020. She had previous of two pregnancies. The patient underwent a simple mastectomy for carcinoma of the left breast without adjuvant chemotherapy. After surgery, the patient did not come for any follow-up visits.
In July 2023, the patient presented in the emergency department of the hospital with severe pain in the left axilla and chest not controlled by analgesics, uncontrolled hypertension (200/100 mmHg), and shortness of breath with desaturation. She was hospitalized and treated intensively. Pain and hypertension were controlled. She received oxygen support and hydration.
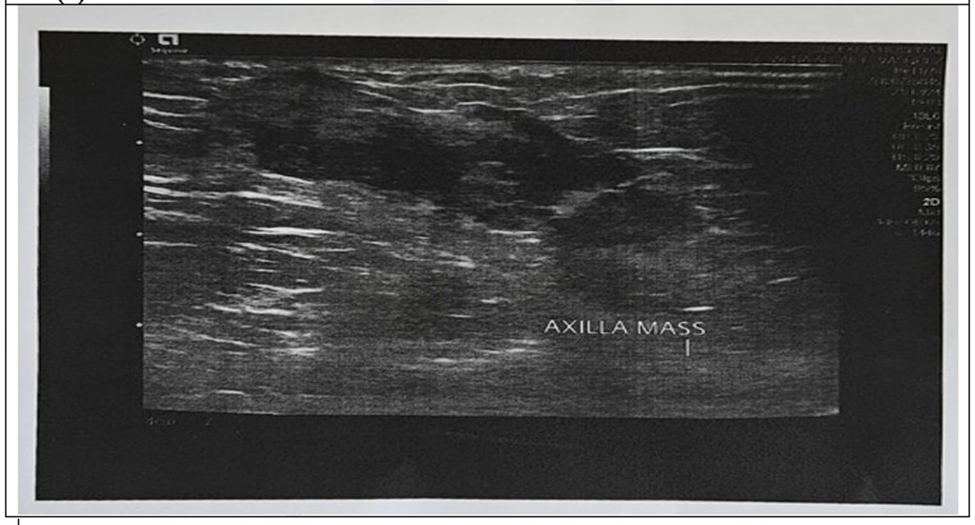
On stabilizing the patient’s general condition, a biopsy of the axillary tail mass which was almost 7x7cms was done. The biopsy of the mass reported invasive adenocarcinoma of the breast with mucinous differentiation (Grade 2) with lympho-vascular invasion. The imaging scan showed the left axillary mass to be 48 x 45 x 44mm in size, well-defined, lobulated, partially necrotic, and seen reaching up to the skin surface with thickening. The features were suggestive of recurrence. A similar partially necrotic mass of 5.3mm in craniocaudal extent and 3.3cm in width, is seen along the left lateral chest wall with invasion of overlying subcutaneous fat and skin. It also reported left pleural effusion suggestive of lung metastasis, mediastinal lymph nodes, and bone metastasis. Immunohistochemistry (IHC) of the tissue demonstrated 90% positivity for ER, 5% positivity for PR, HER2 negativity (1+), and a Ki 67% score of 20%. She was diagnosed with ‘recurrent metastatic breast cancer with metastatic disease in lungs, lymph nodes, and bones.’
Clinically, the patient was in impending respiratory crisis and failure. However, the patient refused to take chemotherapy.
Hence, the subject was started on the biological targeted therapy, a cyclin-dependent kinase (CDK) inhibitor 4 and 6 (CDK inhibitors 4/6) abemaciclib in combination with hormone therapy of letrozole, and goserelin, along with bone support agent zoledronic acid.
After three cycles, local axillary mass was reduced by more than 50%, respiratory function became normal, and there was no more chest or axillary pain. The repeat scan done after three months of the treatment demonstrated a good treatment response.
After cycle 5, the local mass almost disappeared along with the bone pain. The subject was continued on the same treatment. A comparison between before and after the treatment scan images of axillary mass and lung metastasis is presented in images 1 and 2, respectively.Presently the patient is in stable disease with excellent treatment response without any chemotherapy. The patient reported a better quality of life where she is able to enjoy with her family and friends.
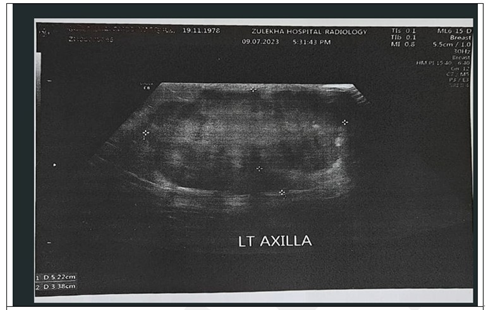
(a) Before the treatment for MBC.
(b) After the treatment for MBC.
Figure 1: Ultrasound image comparison of left axillary mass before and after MBC treatment.
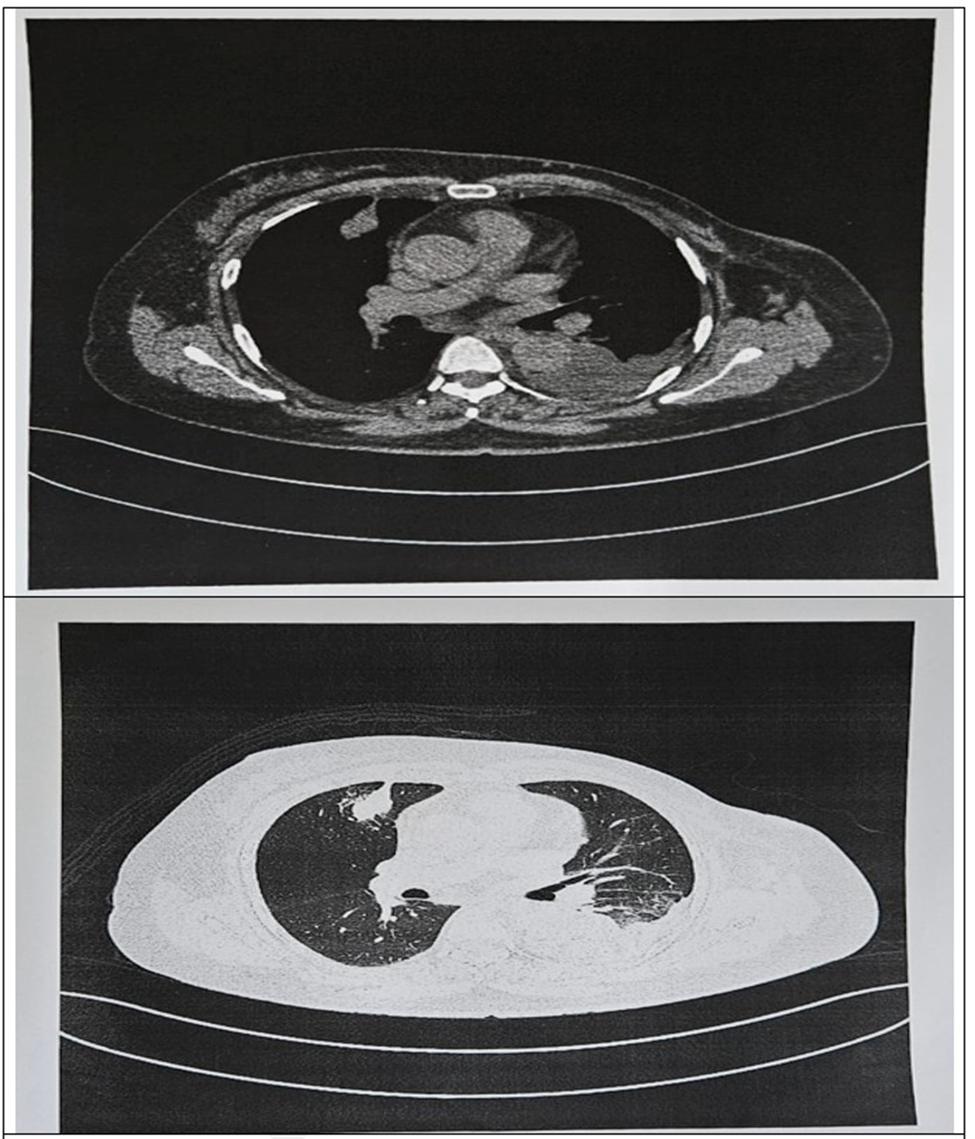
Figure 2: Computed tomography image comparison of Lung metastasis before and after treatment. (a) Before the treatment of MBC. (b) After the treatment of MBC
Discussion
Carcinogenesis is a multifactorial process that is primarily stimulated by both—genetic predispositions and environmental causes. Incidence of breast cancer and death rates have increased over the last three decades due to the change in risk factor profiles, better cancer registration, and cancer detection [7]. About 5-10% of breast cancer patients will have local or locoregional recurrence after breast-conserving surgery and radiotherapy within ten years of first being diagnosed with breast cancer. If the breast was removed in the course of initial treatment, about 5% of the women will have a local recurrence in the armpit or the chest wall within ten years [8]. The occurrence of locoregional recurrence is often associated with distant spread and such patients should undergo full staging procedures before undergoing local treatments [9]. Hence, it is important for patients to follow up with the oncologist or expert health care provider even after primary diagnosis and treatment completion. In case of our patient, she was lost to follow-up post mastectomy and presented after 2 years with local recurrence and symptomatic disease progression in an acute respiratory crisis. Her further work-up showed metastasis in the lungs, lymph nodes, and bones with a recurrence of breast cancer.
The two main goals for the treatment of metastatic breast cancer (MBC) patients are to improve survival and to optimize the quality of life [10]. Patients with cancer face a great amount of mental and physical distress, which itself has been linked to increased healthcare usage, decreased survival, and suboptimal quality of life. Ensuring a positive patient experience should be a top priority throughout the entire treatment journey, as higher patient satisfaction can drive improved health outcomes, treatment adherence, and quality of life [11]. It is crucial to understand the patient’s wishes while planning the treatment for its adherence and success.
ESMO guideline states that the management of MBC should involve all appropriate specialties in a multi/interdisciplinary team (medical, radiation, surgical, and imaging oncologists, palliative care specialists, and psychosocial support), and patients should be offered personalized appropriate psychosocial, supportive, and symptom-related interventions as a routine part of their care. Systemic treatment options for MBC are endocrine therapy, chemotherapy, and bone-directed agents.9 The guideline emphasizes considering patient preferences along with other factors for treatment selection.9 For patients with (ER+ve and HER2-ve) MBC, ESMO living guideline suggests systematic chemotherapy or combination therapy with an aromatase inhibitor and CDK4/6 till the progression of disease [12].
Our patient was not willing to receive chemotherapy for MBC. Respecting our patient’s wish to not be treated with chemotherapy for MBC (ER+ve, HER2-ve), the subject was treated with a CDK inhibitor 4/6 abemaciclib in combination with hormone therapy of letrozole, and goserelin along with zoledronic acid.
Endocrine therapy is among the most powerful tools currently available for the prevention and treatment of breast cancer, whether in the adjuvant or metastatic setting [13]. Breast cancer cells with ER and/or PR depend on estrogen and/or progesterone to grow. ER and/or PR expression is a crucial determinant for patients to be able to benefit from endocrine therapy targeting estrogen action, such as selective ER modulators (tamoxifen), aromatase inhibitors (letrozole, anastrozole, exemestane), and ER down regulators (fulvestrant). Endocrine therapy is generally well tolerated and an easy-to-administer option for hormone-positive breast cancer patients [14].
CDK 4/6 inhibitor, is a comparatively novel therapy. Currently, three CDK4/6 inhibitors are approved by the U.S. Food and Drug Administration for the management of advanced breast cancer in combination with endocrine therapy. These include, palbociclib, ribociclib, and abemaciclib. Specifically, these agents are used for the treatment of hormone receptor-positive, and HER2-negative metastatic breast cancers [15]. They act by targeting the cell cycle machinery, interrupting intracellular and mitogenic hormone signals that stimulate the proliferation of malignant cells [16]. A study assessing two years of adjuvant abemaciclib combined with endocrine therapy resulted in a significant improvement in invasive disease-free survival and distant relapse-free survival that persisted beyond the 2-year treatment period in patients with hormone receptor-positive, HER-2–negative, node-positive, highrisk early breast cancer [17].
Our patient demonstrated a good response to biological targeted therapy in combination with hormonal therapy with no local or bone pain, improved respiration, and almost disappeared axillary mass. There were no adverse reactions or toxicities. The patient showed good treatment adherence. She reported a significantly improved quality of life, where she can actively enjoy life with her loved ones.
Conclusion
Breast cancer is a complex disease that necessitates thorough evaluation to determine the most suitable treatment plan. It is essential for patients to follow up with oncologists or expert healthcare providers after primary treatment for effective screening, facilitating early detection of disease recurrence or progression to avoid critical situations. Encouraging patient participation in decision-making and respecting their preferences is vital for better treatment adherence, and success. Metastatic breast cancer (MBC) does not always require chemotherapy for disease regression. Endocrine therapy combined with adjuvant CDK 4/6 inhibitors tailored as per the patient’s preference can play a crucial role in extending overall survival in patients with MBC.
List of Abbreviation
CDK: Cyclin-dependent kinase
ER: Estrogen receptor
HER2: Human epidermal growth factor receptor-2
IHC: Immunohistochemistry
LR: Local recurrence
LRR: Locoregional recurrence
MBC: Metastatic breast cancer
PR: Progesterone receptor
Author Contributions (per ICMJE, adapted for a Case Report)
Dr. Anwar Alroubaie conceptualized the case report, gathered and interpreted clinical data, drafted, reviewed and finalized the article. He takes full responsibility for the integrity and accuracy of the entire report.
Guarantor of the Article
Dr. Anwar Alroubaie is the guarantor of this case report, and accepts full responsibility for the integrity of the work as a whole, ensuring that any questions regarding accuracy or integrity of any part of the report are appropriately addressed.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
References
- Arnold M, Morgan E, Rumgay H, Mafra A, Singh D, et al. (2022) Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast Off J Eur Soc Mastology. 66:15-23.
- Ren Z, Li Y, Hameed O, Siegal GP, Wei S, et al. (2014) Prognostic factors in patients with metastatic breast cancer at the time of diagnosis. Pathol - Res Pract. 210:301-306.
- CDC. Metastatic Female Breast Cancer Incidence. United States Cancer Statistics. 2025.
- Margolese RG, Hortobagyi GN, Buchholz TA (2003) Management of Metastatic Breast Cancer. In: Holland-Frei Cancer Medicine. 6th Edition. BC Decker; 2003.
- Neuman HB, Steffens NM, Jacobson N, Tevaarwerk A, Anderson B, et al. (2016) Oncologists’ Perspectives of their Roles and Responsibilities during Multi-disciplinary Breast Cancer Follow-up. Ann Surg Oncol.23:708-714.
- Noteboom EA, May AM, van der Wall E, de Wit NJ, Helsper CW, et al. (2021) Patients preferred and perceived level of involvement in decision making for cancer treatment: A systematic review. Psychooncology.30:1663-1679.
- Łukasiewicz S, Czeczelewski M, Forma A, Baj J, Sitarz R, et al. (2021) Breast Cancer—Epidemiology, Risk Factors, Classification, Prognostic Markers, and Current Treatment Strategies—An Updated Review. Cancers. 13:4287.
- Breast cancer: Learn More – Recurrent non-metastatic breast cancer. 2025.
- Cardoso F, Harbeck N, Fallowfield L, Kyriakides S, Senkus E, et al. (2012) Locally recurrent or metastatic breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 23:vii11-vii19.
- Chacón López-Muñiz JI, de la Cruz Merino L, Gavilá Gregori J, Dueñas EM, Oliveira M, et al. (2019) SEOM clinical guidelines in advanced and recurrent breast cancer (2018). Clin Transl Oncol. 21:31-45.
- Ho T. (2022) Building the Optimal Patient Experience Takes Planning and Effort. 23:48-49.
- ESMO Metastatic Breast Cancer Living Guideline | ESMO. 2025.
- Wisinski KB, Tevaarwerk AJ, O’Regan RM. 70 (2018) Endocrine Therapy for Breast Cancer. In: Bland KI, Copeland EM, Klimberg VS, Gradishar WJ, eds. The Breast (Fifth Edition). Elsevier 907-923.e6.
- Li Z, Wei H, Li S, Wu P, Mao X (2022) The Role of Progesterone Receptors in Breast Cancer. Drug Des Devel Ther 16: 305-314.
- Sheikh MS, Satti SA (2021) The emerging CDK4/6 inhibitor for breast cancer treatment. Mol Cell Pharmacol 13: 9-12.
- Scott SC, Lee SS, Abraham J (2017) Mechanisms of therapeutic CDK4/6 inhibition in breast cancer. Semin Oncol 44: 385-394.
- Rastogi P, O’Shaughnessy J, Martin M, Boyle F, Cortes J, et al. (2024) Adjuvant Abemaciclib Plus Endocrine Therapy for Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2– Negative, High-Risk Early Breast Cancer: Results From a Preplanned monarchE Overall Survival Interim Analysis, Including 5-Year Efficacy Outcomes. J Clin Oncol 42: 987-993.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.