Evaluating Robotic-Assisted Radical Prostatectomy: A Systematic Video-Based Review
by Tayla Fay 1,2*, Ting Zhang 3*, Thomas McMaster2*, Andrew Wu3, Akarsh Singh4, Owen Niall1,5*
1International Medical Robotics Academy, Melbourne, Australia
2Department of Urology, Sunshine Coast University Hospital, Birtinya, QLD, Australia
3Department of Surgery, The University of Melbourne, Melbourne, VIC, Australia
4Department of Surgery, Monash University, Melbourne, VIC, Australia
5Department of Urology, St Vincent’s Hospital Melbourne, Melbourne, VIC, Australia * Joint first author.
*Corresponding Author: Tayla Fay, Department of Urology, Sunshine Coast University Hospital, Birtinya, QLD, Australia
Received Date: 21 April 2026
Accepted Date: 27 April 2026
Published Date: 29 April 2026
Citation: Fay T, Zhang T, McMaster T, Wu A, Singh A, et al. (2026) Evaluating Robotic-Assisted Radical Prostatectomy: A Systematic Video-Based Review. J Surg 11: 11620 DOI: https://doi.org/10.29011/2575-9760.011620
Abstract
Background: Robotic Assisted Radical Prostatectomy (RARP) has gained popularity in recent years due better surgical dexterity and improved patient outcomes.
Objective: This systematic review aimed to assess the quality of available video resources for robotic assisted radical prostatectomy training.
Methods: A systematic review was conducted to evaluate the quality of available videographic robotic prostatectomy content. The search was carried out on PubMed, Ovid, and Web of Science using a predefined search strategy. Video quality was measured by three independent reviewers who assessed the operative steps and key teaching points, with results presented as a narrative synthesis.
Results: All videos showcased part or all of the surgical procedure, but only four provided clinical outcomes. Histopathology was included in three videos, with varied reporting of other outcomes, and patient-reported outcomes were notably absent in all videos. Only two videos documented the rate of recurrence during follow-up. Video quality was assessed using the Ro-VEGAS score, with a mean score of 13.2.
Conclusion: Articles utilising video provide valuable educational resources for disseminating and adopting robotic surgical techniques. Optimisation of video structure has the potential to increase the impact of these videos for learning.
Keywords: Prostate Cancer; Robotic Surgery; RARP
Introduction
Prostate cancer continues to pose a substantial health challenge. Between 2013 and 2017, one in three cancer diagnoses in men was a urological cancer. Annually, out of the 302,304 urological cancer cases diagnosed, 67% were localized in the prostate, with an estimated 1.41 million new cases worldwide in 2020 [1]. RARP offers a minimally invasive alternative to traditional open surgery. RARP is performed using a well-defined sequential approach. The robotic platform provides increased range of motion, improved ergonomics, and enhanced visualisation. These advancements have led to increased surgical precision, decreased blood loss, decreased complications, shorter hospital stays, and overall improved patient outcomes [2-4]. The most important variable in the outcome of the surgery is the experience of the surgeons, highlighting the requirements of high-quality training [5]. Robotic surgery has become ubiquitous in the field of urology [6]. Currently, there is a notable paucity of peer-reviewed, published videographic content in peer-reviewed journals. The growing popularity and distinct benefits of RARP make it crucial to establish comprehensive, accessible, and effective educational resources [7]. Robotic surgery, with its inherent ease of video recording due to the console-based system, presents a unique opportunity for surgical education and training. Videos serve as an invaluable learning tool, capturing nuanced, dynamic movements in surgery that may not be effectively communicated through text or images alone [8,9]. Video offers the ability to visualise key elements of each surgical step, aiding in understanding and mastering the complex surgical anatomy and procedural intricacies of RARP. Currently, although there have been reviews on educational strategies in robotic prostatic surgery, there has been little systematic evaluation of the current video resources published in peer-reviewed journals. To address this gap, we present a systematic review of the available videos published in peer-reviewed journals on RARP. Our review evaluates the technical, operative, anatomic, and educational aspects of these videos under the guidance of a modified LapVEGAS score, the Robotic Surgery Video Educational Guideline Assessment Score (Ro-VEGAS) [10,11]. This innovative approach to assess and score robotic surgical videos will provide a comprehensive understanding of the current state of available video learning resources for RARP and inform our design of video-based education in the future.
Methods
Methods: This systematic review was conducted in accordance with the Preferred Reporting Items for Scoping Reviews and Meta-Analyses (PRISMA) 2020 statement.
Protocol and registration: A protocol for this systematic review was developed and pre-registered on Prospero. (CRD42023421618)
Eligibility criteria: Eligibility criteria included all publications, including videographic information, about RARP in English between 2004 and 2023. Inclusion criteria were studies performed on human subjects, demonstrating part or all of a RARP, including any novel techniques. Exclusion criteria included conference abstracts, letters to the editor, and procedures on non-human and cadaver models.
Results
Two researchers independently reviewed the videos with a third senior urology consultant to resolve disagreements. The RO-VEGAS criteria were applied to assess the accuracy of the videos in their reporting and the quality of the video content for educational purposes. A comprehensive search was conducted using PubMed, Ovid, and Web of Science, supplemented by manual searches of the reference lists of relevant articles. The final searches were run on 26 August 2023 with the concepts linked together: “Prostate AND resection or excision or removal or Prostatectomy AND robot* AND video*. The MeSH term were Prostate, Prostatectomy and Robotic surgery. All search results were combined in a bibliographic management tool (EndNote).
Data Charting Process
Data items: Data items included study design, participant characteristics, type of publication, outcome measures, and results.
Synthesis of results: A narrative synthesis of the results was conducted, focusing on the RARP videos and their effectiveness in robotic surgery education.
Characteristics of sources of evidence: The included studies were primarily conducted in the United States, Europe, and Brazil.
Results of individual sources of evidence: Online video resources identified in the review included formal case presentations as well as video adjuncts related to a text article.
Results
In total, 248 articles were identified, 74 duplicates were removed, and 68 underwent abstract screening (Figure 1- PRISMA). After screening the titles and abstracts along with exclusion criteria, a total of 10 full-text original articles were included for the final systematic literature review. All videos were published between 2004 and 2022. 4 out of 10 videos were from the European Urology journal, 2 were from the International Brazilian Journal of Urology and Journal of Endourology, 1from the Journal of Robotic Surgery and 1 from Urology. Length of video ranged from 7.15minutes to 68.36 minutes, with an average time of 16.22 minutes (Tables 1,2).
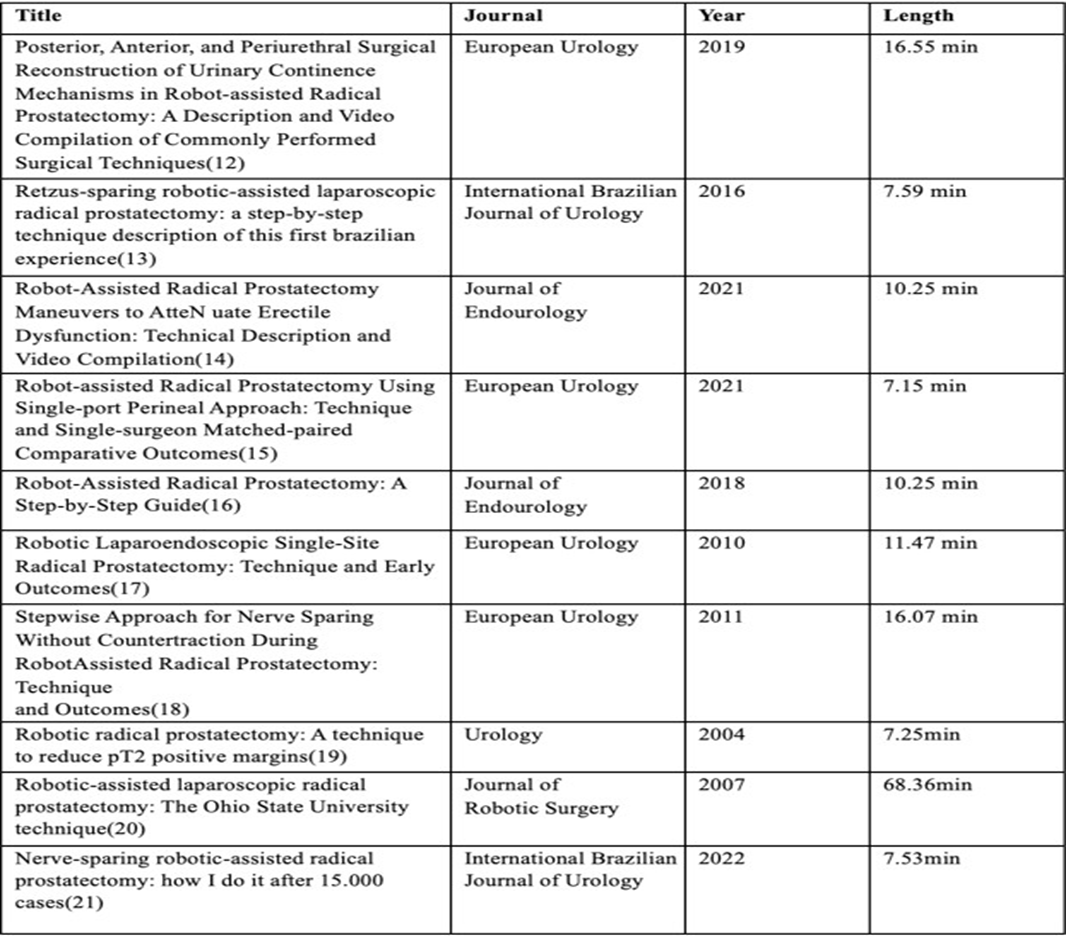
Table 1: A summary of included articles.
Key: V= Verbalised; VI = visualised ; L= labelled
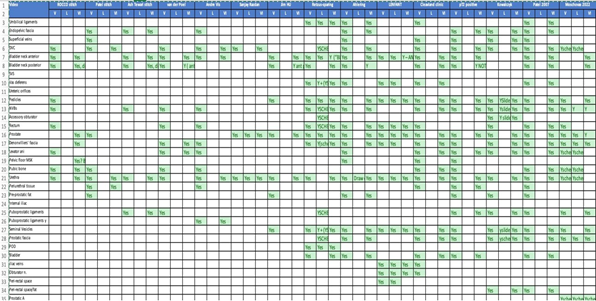
Table 2: Labelled anatomic structures.
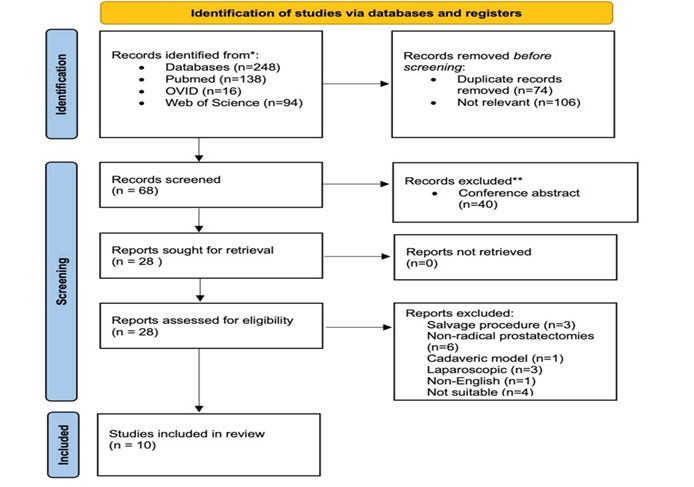
Figure 1: PRISMA diagram of search results.
Video Structure and Content
Content varied from whole procedures to single aspects of surgery. Video presented by Vis AN et al. [12] focused on one aspect of the surgery with partial visualisation of structures and comments. The video by Tobias-Machado M et al.[13] included a comprehensive list of materials used, robotic console types, operating times, console times, and 12 surgical steps. As well as intraoperative blood loss, postoperative complications, length of hospital stay, histopathology, continence and erectile function at 30 days. Basourakos SP et al. [14] listed outcomes from multivariate analysis, as well as histopathology of the musculoskeletal structures and urethra. Lenfant L et al.’s [15] video listed port placement, docking, incision site and the robotic system used. Anatomical structures were labelled, and a table of patient demographic data was presented. Overall, labelling was not consistently included across the videos. However, the urethra and the anterior bladder neck were labelled in most of the videos. Notably, the prostate was not labelled in 70% of the videos.
Video Graphic Points and Application 0f RO-VEGAS Score
The mean RO-VEGAS score was 13.22, ranging from 9 to 17. Details of the scoring are outlined in (Table 3). Notably, only 10% of videos demonstrate docking of the robot. All videos maintained a clear view of the operating field. Most videos included graphic aids at the beginning of the operation or between steps to demonstrate key anatomy or to provide additional educational content. One video had a graph of a meta-analysis including surgical outcomes. 40% of videos presented part or all of the procedure outcome data, operative time, post-op morbidity and histology. All the videos effectively highlighted key intraoperative findings and consistently referenced key anatomical landmarks either verbally or visually with the aid of diagrams. All videos presented the procedure in a structured, sequential manner. Information on the positioning of the patient, surgical team, ports and excision site was present in 40% of the videos. Most videos listed the institution and authors clearly and included the name of the procedure. Only 30% of the videos included the pathology being treated. Lastly, 40% of videos did not include a formal case presentation, omitting key details such as patient demographics and comorbidities, diagnostic imaging and indication for surgery. All cases maintained patient anonymity [16-21].
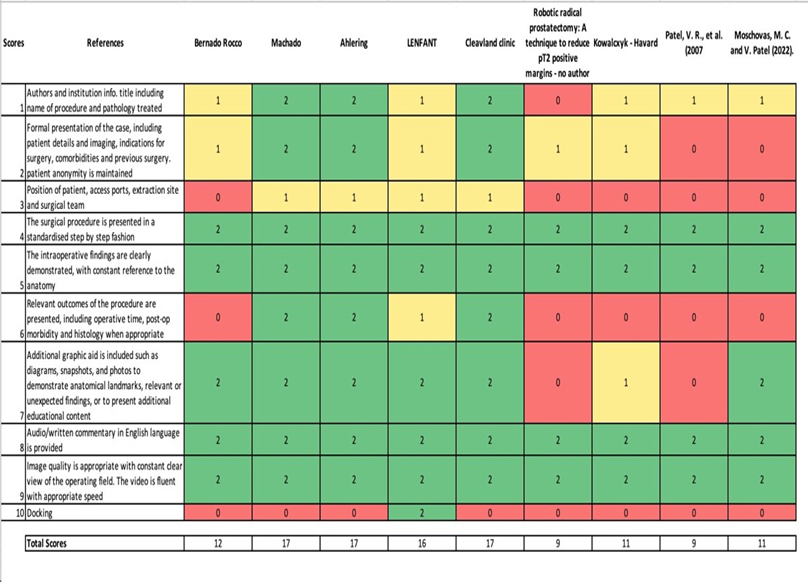
Table 3: A summary of the Ro-VEGAS score.
Discussion
Benefits of Video
learning It is well recognised that video resources are valuable learning tools, especially in the field of surgery. As technology advances, internet access and portable electronic devices have become ubiquitous [22]. Online educational video resources are available in multiple formats. Some are short snippets with loaded learning points, others are detailed and continuous recordings of the whole surgical procedure. Larkins et.al. recommend short videos presented in modules, under a specific heading with appropriate narration. This allows for an easily manageable cognitive load, increasing learner engagement and promoting active learning [23]. Research has shown that video case reports containing both audio and visual elements have better engagement with the audience, enhance understanding, and improve trainee application [24]. Online learning provides flexibility and feasibility to close the gaps in surgical training regardless of clinical workload, location of practice and socioeconomic status [25]. Online learning can present solely as video recordings of surgical procedures and lectures, or in combination with text to form more interactive virtual patient cases, modules, and online tutorials. A review presented by Bonk CJ et al [25] reported significant knowledge gain from e-learning presented within the above format. The incorporation of videos into surgical education also allows for asynchronous learning and broad dissemination of video resources. Video learning allows learners to revisit and critically evaluate material at their convenience. With the prevalence of smart devices and ubiquitous internet access, e-learning is an increasingly accessible and growing tool. These online materials can be accessed on demand, globally, if there is adequate internet coverage. When correctly presented, video resources offer enriched information and greater learning value. Additionally, peer-reviewed teaching tools are crucial in identifying benefits and gaps in the literature, as well as addressing potential difficulties in teaching and opportunities for research [26]. Publishing in peer-reviewed journals also provides assurance of maintaining the integrity of the video material and intellectual property ownership, which is impractical to maintain through other free-source platforms, such as YouTube.
Source of Video Learning
While searching for RARP videos, medical professionals use YouTube as a primary teaching tool for video references, especially for surgical specialities [27]. Due to publication limitations, most published videos condense hours of surgical recordings to just a few minutes of teaching points. Meanwhile, on YouTube, there are fewer restrictions, and videos can be easily posted, with a mean length of 1-2 hours. Newer generations of medical students also incorporate YouTube videos in many aspects of their learning, due to accessibility and ease of use [28]. Although no relevant videos from YouTube were included in this review, a brief search using the keywords revealed numerous videos ranging from short learning bites in a couple of minutes to detailed surgical encounters of hours in length. However, the search engine in YouTube provides personalised, rather than systematic, results, which are less objective compared to formal research databases due to a lack of rigorous Boolean operators and strict search terms. Some papers showed that YouTube does have higher-quality surgical videos compared with most curated sources based on the GEARS criteria, owing to the significantly larger quantity of videos on YouTube [29]. Notably, Arslan B et al found it challenging to predict the educational value of YouTube videos due to a lack of objective parameters [30]. Further research is required in this field to ensure greater consistency of YouTube video quality and ways of utilising them as accessible and structured educational resources.
Our Results and Relevant Studies
Robotic video case reports have been shown as a superior learning resource, especially in the field of surgery, as they ensure a visuospatial demonstration of complex anatomical structures. This review reveals a paucity of suitable learning and teaching videos on the topic of RARP and a low standard of quality using the IDEAL framework [31]. The use of video abstracts in established journals and publications is in its infancy, and this could account for the paucity of published RARP videos in our study. The genesis of Robotic prostatectomy predated the use of video abstracts. This is an area journals need to adapt and improve. A systematic review of Robotic pelvic side-wall lymph node dissection for rectal cancer by Mansour et.al [11] also found video resources in the relevant area had poor adherence to the IDEAL2a framework due to limited reporting of clinical outcomes, histopathology reports, zero patient-reported outcome measures and a lack of follow-up on the recurrence of cancer. Mansour et.al [11] are the first to present a systematic view of robotic videos using the ROVEGAS score. This article also acknowledges that videos are an important and valid exceptional teaching tool. However, to produce more consistent teaching videos that can benefit surgical trainees, standardisation criteria on video content will further enhance its educational value. Being the first to look at video resources in robot-assisted surgery in urology. Our results highlight the gaps in the literature regarding low adherence to the standard criteria. There is an urgent need to standardise video-based educational tools for RARP. Establishing frameworks will enhance the quality of robotic training and, in turn, improve patient outcomes.
Most Videos Did not Have the Surgical Date Visible
although this is not part of the scoring criteria, the dates play an important role in presenting videos in chronological order in this emerging field, where new techniques are being implemented. Furthermore, none of the videos mentioned journal names in their video: we believe this is an important feature to include for transparency and credibility of both the videos and the journals. Clear labelling on the videos is also recommended, especially labelling left and right on the operation field and any changes in angulation or the use of a 30-degree scope should be made clear. IMRA Video-Based Learning for Partial Nephrectomy
This review was used to continue to inform the refinement and development of an online simulation package at the International Medical Robotics Academy (IMRA). Using Kern’s model for curriculum development, this review helped identify gaps in current robotic videos to consider in design of the IMRA online partial nephrectomy module using Kern’s model for curriculum development.
Future Direction
This review challenges the quality of published RARP video resources and acknowledges that there is a need for standardised video guidelines for RARP and, more broadly, for robotic surgery videos to ensure the maximum value of videos as a teaching tool in the future. We aim to promote an increase in the quality of peerreviewed RARP videos with the establishment of the guidelines and criteria to standardise RARP training further; this will also promote wider adoption and clinical application of RARP in the treatment of prostate cancer.
Conclusion
This review evaluated current peer-reviewed RARP video standards in the treatment of prostate cancer, which highlighted the need for standardised guidelines to optimise the educational utility of videos as a teaching medium in robotic surgery. With emerging RARP popularity, it is essential to standardise the published videos to ensure high-quality, trusted educational resources for better surgical training and wider adoption of the RARP technique. Recommendations for future videos include clear real-time labelling of structures, inclusion of clinical outcomes and detailing patient positioning, port placement and docking.
Limitations
A key limitation of this study is its restriction to peer-reviewed robotic prostatectomy videos published in academic journals, excluding freely accessible sources such as YouTube. Future research should evaluate and compare the educational quality of peer-reviewed content versus freely posted videos to develop objective criteria
for standardising YouTube as a reliable educational platform. Additionally, this review was limited to studies published in English.
References
- Centers for Disease Control and Prevention. [Internet]. Centers for Disease Control and Prevention, US Department of Health and Human Services. 2020.
- Mack MJ (2001) Minimally invasive and robotic surgery. Jama 285: 568-872.
- Narula VK, Watson WC, Davis SS, Hinshaw K, Needleman BJ, et al. (2007) A computerized analysis of robotic versus laparoscopic task performance. Surgical endoscopy 21: 2258-2261.
- Diana M, Marescaux J (2015) Robotic surgery. Journal of British Surgery 102 :e15-e28.
- Top 10 Patient Safety Concerns for 2021 [Internet]. 2021.
- Marcus HJ, Hughes‐Hallett A, Payne CJ, Cundy TP, Nandi D, et al. (2017) Trends in the diffusion of robotic surgery: A retrospective observational study. The International Journal of Medical Robotics and Computer Assisted Surgery 13: e1870.
- Lanfranco AR, Castellanos AE, Desai JP, Meyers WC (2004) Robotic surgery: a current perspective. Annals of surgery 239: 14-21.
- Buch SV, Treschow FP, Svendsen JB, Worm BS (2014) Video-or textbased e-learning when teaching clinical procedures? A randomized controlled trial. Advances in Medical Education and Practice 2014: 257-262.
- Bilbro NA, Hirst A, Paez A, Vasey B, Pufulete M, et al. (2021) The IDEAL Reporting Guidelines: A Delphi Consensus Statement Stage Specific Recommendations for Reporting the Evaluation of Surgical Innovation. Ann Surg 273: 82-85.
- Celentano V, Smart N, Cahill RA, Spinelli A, Giglio MC, et al. (2021) Development and validation of a recommended checklist for assessment of surgical videos quality: the LAParoscopic surgery Video Educational GuidelineS (LAP-VEGaS) video assessment tool. Surgical endoscopy 35: 1362-1369.
- Mansour KP, Mohan HM, Jiang W, Waters PS, Larach JT, et al. (2023) Robotic pelvic side-wall lymph node dissection for rectal cancer: a systematic review of videos and application of the IDEAL 2A framework. Journal of Robotic Surgery. 2023:1-12.
- Vis AN, van der Poel HG, Ruiter AEC, Hu JC, Tewari AK, et al. (2019) Posterior, Anterior, and Periurethral Surgical Reconstruction of Urinary Continence Mechanisms in Robot-assisted Radical Prostatectomy: A Description and Video Compilation of Commonly Performed Surgical Techniques. European urology 76: 814-822.
- Tobias-Machado M, Nunes-Silva I, Hidaka AK, Sato LL, Almeida R, et al. (2016) Retzus sparing robotic-assisted laparoscopic radical prostatectomy: a step-by-step technique description of this first brazilian experience. Int Braz J Urol 42: 1250.
- Basourakos SP, Kowalczyk K, Moschovas MC, Dudley V, Hung AJ, et al. (2021) Robot-Assisted Radical Prostatectomy Maneuvers to Attenuate Erectile Dysfunction: Technical Description and Video Compilation. Journal of endourology 35: 1601-1609.
- Lenfant L, Garisto J, Sawczyn G, Wilson CA, Aminsharifi A, et al. (2021) Robot-assisted Radical Prostatectomy Using Single-port Perineal Approach: Technique and Single-surgeon Matched-paired Comparative Outcomes. EUROPEAN UROLOGY 79: 384-392.
- Huynh LM, Ahlering TE (2018) Robot-Assisted Radical Prostatectomy: A Step-by-Step Guide. JOURNAL OF ENDOUROLOGY 32: S28-S32.
- White MA, Haber G-P, Autorino R, Khanna R, Forest S, et al. (2010) Robotic laparoendoscopic single-site radical prostatectomy: technique and early outcomes. European urology 58: 544-550.
- Kowalczyk KJ, Huang AC, Hevelone ND, Lipsitz SR, Yu H-y, et al. (2011) Stepwise approach for nerve sparing without countertraction during robot-assisted radical prostatectomy: technique and outcomes. European urology 60: 536-547.
- E, Eichel L, Edwards RA, Lee DI, Skarecky DW (2004) Robotic radical prostatectomy: A technique to reduce pT2 positive margins. UROLOGY 64: 1224-1228.
- Patel VR, Shah KK, Thaly RK, Lavery H (2007) Robotic-assisted laparoscopic radical prostatectomy: The Ohio State University technique. JOURNAL OF ROBOTIC SURGERY 1: 51-59.
- Moschovas MC, Patel V (2022) Nerve-sparing robotic-assisted radical prostatectomy: how I do it after 15.000 cases. Int Braz J Urol 48: 369370.
- Mota P, Carvalho N, Carvalho-Dias E, Costa MJ, Correia-Pinto J, et al. (2018) Video-based surgical learning: improving trainee education and preparation for surgery. Journal of surgical education 75: 828-835.
- Larkins K, Mansour K, Costello D, Gray M, Warrier S, et al. (2023) Recommendations for the design of video-based educational interventions as instructional tools in robotic surgical training. Journal of Robotic Surgery 17: 779-784.
- Rasul S, Bukhsh Q, Batool S (2011) A study to analyze the effectiveness of audio visual aids in teaching learning process at university level. Procedia-Social and Behavioral Sciences 28: 78-81.
- Bonk CJ (2011) YouTube anchors and enders: The use of shared online video content as a macrocontext for learning. Asia-Pacific collaborative education journal 7: 13-24.
- Thomas S, Chie QT, Abraham M, Jalarajan Raj S, Beh L-S (2014) A qualitative review of literature on peer review of teaching in higher education: An application of the SWOT framework. Review of educational Research 84: 112-159.
- Rapp AK, Healy MG, Charlton ME, Keith JN, Rosenbaum ME, et al. (2016) YouTube is the Most Frequently Used Educational Video Source for Surgical Preparation. Journal of Surgical Education 73: 1072-1076.
- Youssef SC, Aydin A, Canning A, Khan N, Ahmed K, et al. (2023) Learning surgical skills through video-based education: a systematic review. Surgical Innovation 30: 220-238.
- Crisostomo-Wynne T, Hertz A, Banti M, Brand T, Caras R (2021) Comparison of Robotic Surgery Video Quality Between YouTube and Curated Sources Using GEARS Criteria. Urology 156: 44-46.
- Arslan B, Gönültaş S, Gökmen E, Özman O, Onuk Ö, Yazıcı G, et al. (2020) Does YouTube include high quality resources for training on laparoscopic and robotic radical prostatectomy? World J Urol 38: 1195-1199.
- McCulloch P, Altman DG, Campbell WB, Flum DR, Glasziou P, et al. (2009) No surgical innovation without evaluation: the IDEAL recommendations. The Lancet 374: 1105-1112.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.