Endoscopic Dural Tear Repair: Technical Note and Literature Review
by Luis E. Carelli1,2, Silvia M. Flores Taracena1,2*
1National Institute of Traumatology and Orthopaedics (INTO), Rio de Janeiro, RJ, Brazil.
2Spine Institute of Rio de Janeiro (INCOL), Rio de Janeiro, RJ, Brazil.
*Corresponding author: Silvia M. Flores Taracena, Department of Spine Surgery, National Institute of Orthopedics and Traumatology, INTO, Rio de Janeiro, Brazil
Received Date: 28 January 2025
Accepted Date: 01 February 2025
Published Date: 04 February 2025
Citation: Carelli LE, Flores Taracena SM (2025) Endoscopic Dural Tear Repair: Technical Note and Literature Review. Ann Case Report. 10: 2182. https://doi.org/10.29011/2574-7754.102182
Abstract
Background: Incidental dural tears during lumbar spine surgery are one of the most important complications, with highest rate in older patients, lumbar stenosis cases and bilateral decompression realized with a unilateral approach. The primary repair of a dural tear is the gold standard treatment, but in endoscopic surgery there is no standard protocol, the common strategies include patch compression (in small dural tears) and conversion to open repair.
Case Description: 81-years-old female, severe right leg radiculopathy and neurological claudication, lumbar hypertrophic facets in L4-L5 and hypertrophy of ligamentum flavum causing lumbar stenosis in the same level. Endoscopic decompression with an incidental durotomy on the dorsolateral aspect, approximately 7mm. We proceed to repair the lesion, full endoscopic, using the “Inside-out technique”.
Conclusions: Older patient with lumbar stenosis, doing a successful full endoscopic primary repair, without especial instruments, led to a successful recovery, no cerebrospinal fluid leakage and allowing early mobilization.
Keywords: Spinal Stenosis; Surgical Decompression; Minimally Invasive Surgery; Endoscopy; Dura Mater.
Introduction
Incidental dural tears during lumbar spine surgery are one of the most important complications, the prevalence has been reported ranging from 0.5 to 18% [1,2].
The predisposing conditions include fibrotic adhesion (especially in migrated hernias), eroded dura, redundant dura in patients with large disc herniation. Patients under local anesthesia and sedation can report back pain, leg numbness and sometimes the urge to urinate when the dural tear occurs [1].
Cerebrospinal fluid leakage induces headache, nausea, intracranial hypotension, intracranial hemorrhage, pseudo-meningocele, wound infection, meningitis and neurologic deficit [3]. Usually the typical symptoms (wound swelling, headache or dizziness caused by CSF leakage) are not typical in endoscopic spine surgery, because there is not enough space to collect CSF [1,4].
As time passes with the dural tears, delayed widening of the dural opening due to the increased intraspinal pressure may cause significant neural entrapment syndrome [1]. If the dural tear is not treated appropriately it could lead to pseudomeningocele due to cerebrospinal fluid leakage, surgical site infection or meningitis [2].
The highest rate of dural tears was in older patients, lumbar stenosis cases (3.7%), cases in which synovial cysts were resected; in relation to the type of procedure, a highest risk when a bilateral decompression was realized with a unilateral approach [5]. Because lumbar stenosis is more frequent to have dural tears, interlaminar approach may have more dural tears than transforaminal approach [6].
The primary repair of a dural tear is the gold standard treatment, but in endoscopic surgery there is no standard protocol. The common strategies include patch compression in small dural tears, conversion to open repair with discontinuation of minimally invasive spine surgery or conservative management with a delayed decision depending on the state of the sequelae [2]. Suturing larger dural tears will also allow early mobilization of the patient and early discharge.
There are few reports of full endoscopic repair or dural tears with different techniques, uniportal with Youn´s technique [7], transforaminal approach by Machado Bergamaschi [8], some with 2-3 portal method, repair with clips and sutures [2,3]. In uniportal methods there are no clips available, considering it too difficult to repair primarily with sutures [3].
In a study of 922 patients with endoscopic surgery they reported incidental dural tears in 5.3% of the patients, 2.5% required suture which was done without converting to open surgery and properly repaired endoscopically. The dural tears were more frequent in micro endoscopic laminectomy patients, 8.1%. The repair was done with a polypropylene 6-0 suture, double arm needle, insideout technique to prevent nerve damage [9].
Other techniques without suture include using polyglactin-910 fixed to the injured dura, small lesions, and then adding fibrin glue [10]. In a report case of bullet wounds of the spine, the dura defect in one case was covered with a patch of fibrin collagen with a biportal technique [11]. Oertel et. al showed a series of 9 cases where the dural tear was repaired using autologous muscle sample fixated with fibrin sealant and gel foam without complications [12].
Technical Report
The patient, 81-years-old female, admitted for severe right leg radiculopathy and neurological claudication. X-rays, computed tomography and magnetic resonance confirmed lumbar hypertrophic facets in L4-L5 and hypertrophy of ligamentum flavum causing lumbar stenosis at the same level. After not improving with conservative treatment, endoscopic surgery was indicated, for spinal stenosis decompression of L4-L5. See Figure 1.
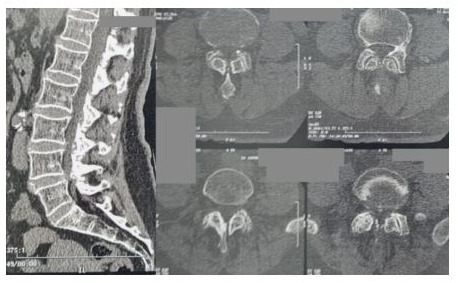
Figure 1: Preoperative Computer Tomography for lumbar spine showing spinal stenosis L4-L5.
Technique description
Patient in prone position under general anesthesia, a right interlaminar approach of L4-L5 using a large stenoscope with a workspace of 7.1mm internal diameter. After using fluoroscopy to mark the entry point, we did a puncture wound from skin to deep fascia, dilators were inserted and later the working sheath. Exposing the interlaminar window with facet hypertrophy, we proceed to do ipsilateral decompression with partial bone resection using a highspeed drill and an endoscopic bone knife (Kerrison) of the facets and lamina to widen the interlaminar window and expose the ligamentum flavum. Careful resection of ligamentum flavum which had many adherences to the dura. We did “over the top” technique to decompress contralateral side. When we were checking the decompression of the neural structures, we noted a durotomy on the dorsolateral aspect, approximately 7mm, which we suspected was done with the working sheath during the “over the top” technique. We proceed to repair the lesion using the “Inside-out technique”, after passing the needle of polypropylene 6-0 in both sides of the lesion we did the knot in the outside of the stenoscope and using the Love we descended the knot without any especial instruments. We did two simple sutures to close the durotomy. See Figure 2. After verifying hemostasia and decompression of the neural structures we did a tight suture of the skin wound and dressed the wound.
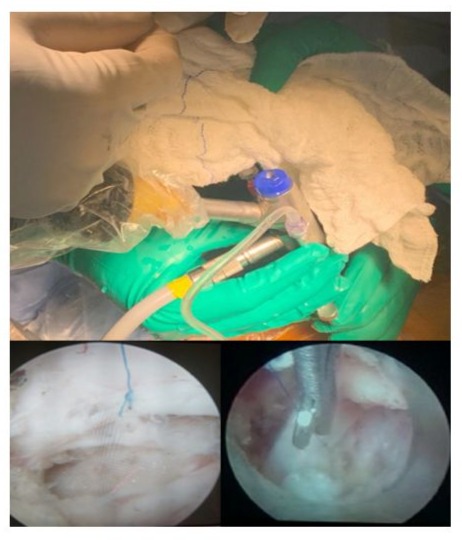
Figure 2: “Inside-out” dural repair technique.
Post-operative, the patient was one day with strict bed rest, no walking, after that the patient started walking with no pain nor headache. The total hospital stay post-operative was 3 days.
The radicular pain improved in three months. Post-operative computer tomography and magnetic resonance showed the interlaminar approach and decompression of the stenosis with partial facet preservation. See Figure 3.
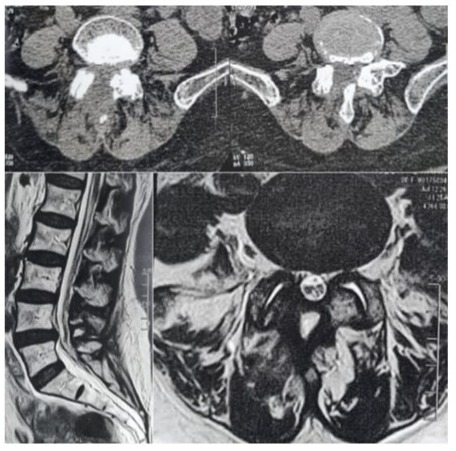
Figure 3: Post-operative Computer Tomography and Magnetic Resonance for lumbar spine showing the decompression made at L4-L5.
Conclusion
In the technical note presentation, an older patient with lumbar stenosis, doing a successful full endoscopic primary repair, without especial instruments, led to a successful recovery.
It is feasible to do the dural suture using a large stenoscope with a wide workspace, so we recommend always to have a larger stenoscope, so if it is not possible to do the repair in a small one, changing to a big one will help to do the repair, decreasing the risk of cerebrospinal fluid leakage and allowing early mobilization.
Acknowledgments: Authors Contributions: all authors contributed equally to this work.
Ethical considerations and informed Consent Statement: Written informed consent has been obtained from the patient(s) to publish this paper.
Conflicts of Interest: None.
Funding: This research received no external funding.
Disclosures: The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.
References
- Yong A, Lee HY, Lee SH, Lee JH (2010) Dural tears in percutaneous endoscopic lumbar discectomy. European Spine Journal. 20: 58-64.
- Kim JE, Choi DJ, Park EJ (2020) Risk Factors and Options of Management for an Incidental Dural Tear in Biportal Endoscopic Spine Surgery. Asian spine journal. 14: 790–800.
- Dong Hwa H, Ha JS, Lee DC, Kim HS, Chung HJ (2020) Repair of Incidental Durotomy Using Sutureless Nonpenetrating Clips via Biportal Endoscopic Surgery. Global Spine Journal. 12: 452-457.
- Choi G, Pophale CS, Patel B, Uniyal P. (2017) Endoscopic Spine Surgery. Journal Korean Neurosurgery Society. 60: 485-497.
- Muller SJ, Burkhardt BW, Oertel JM. (2018) Management of Dural Tears in Endoscopic Lumbar Spinal Surgery: a Review of the Literature. World Neurosurgery. 119: 494-499.
- Lewandrowski KU, Hellinger S, Teixeira De Carvalho PS, Freitas Ramos MR, Soriano-Sánchez JA, et al. (2021) Dural Tears During Lumbar Spinal Endoscopy: Surgeon Skill, Training, Incidence, Risk Factors, and Management. International Journal of Spine Surgery. 15: 280-294.
- Shin JK, Youn MS, Seong YJ, Goh TS, Lee JS. (2008) Iatrogenic dural tear in endoscopic lumbar spinal surgery: full endoscopic dural suture repair (Youn’s technique). European Spine Journal. 27: S544-S548.
- Machado Bergamaschi JP, Flores de Araújo F, Queiroz Soare T, de Oliveira Teixeira K, Dias Sandon LH, et al. (2022) Dural Injury Treatment with a Full-Endoscopic Transforaminal Approach: A Case Report and Description of Surgical Technique. Hindawi. 2022: 6570589.
- Soma K, Kato S, Oka H, Matsudaira K, Fukushima M, et al. (2019) Influence of incidental dural tears and their primary microendoscopic repairs on surgical outcomes in patients undergoing microendoscopic lumbar surgery. The Spine Journal. 19: 1559-1565.
- Sibayama M, Mitzutani J, Takahashi I, Nagao S, Ohta H, Otsuka T. (2008) Patch technique for repair of a dural tear in microendoscopic spinal surgery. The Journal of Bone and Joint Surgery. 90: 1066-7.
- Kravtson MN, Manukovsky VA, Bulyshchenko GG, Mirzametov SD, Byvaltsev VA. (2022) Case Report: Full-Endoscopic Surgery for Bullet Wounds of the Spine: a Report of Three Cases. Frontiers in Surgery. 25: 873365.
- Oertel JM, Burkhardt BW. (2017) Full endoscopic treatment of dural tears in lumbar spine surgery. European Spine Journal. 26: 24962503.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.