Early Interruption of ongoing Posttraumatic Dystrophy
by Egmont Scola*
Department of Traumatology, Dietrich-Bonhoeffer-Klinikum Neubrandenburg, affiliated Hospital of Medical School of University Greifswald, Mecklenburg-Vorpommern, Germany
*Corresponding Author: Egmont Scola, Department of Traumatology, Dietrich-Bonhoeffer-Klinikum Neubrandenburg, affiliated Hospital of Medical School of University Greifswald, Mecklenburg-Vorpommern, Germany
Received Date: 15 December 2025
Accepted Date: 22 December 2025
Published Date: 24 December 2025
Citation: Scola E (2025) Early Interruption of ongoing Posttraumatic Dystrophy. J Surg 10:11523 https://doi.org/10.29011/2575-9760.011523
Abstract: Posttraumatic dystrophy remains an unresolved therapeutical problem. The innate immunity response persists with local perpetuation of vicious circles of aseptic inflammatory reactions. Representative cells for such reactions are the lymphocytes and especially the ubiquitous tissue homing natural killing T cells NKT. Lymphotoxic drugs (glucocorticoides GC) showed the expected good effect in 9 patients (preliminary report).
Keywords: DAMPs; dNKT Cells; Glucocorticoid; Innate Immunity; Lymphotoxic Drug; Posttraumatic Dystrophy
Introduction
Posttraumatic dystrophy remains an unresolved therapeutic problem. Recently the origin of this complication was deduced on damage associated molecular patterns DAMPs, which are formed during tissue trauma from cellular fragments and humoral processes. From the beginning the innate immunity reacts on these “foreign” self molecules with activation of cells and cytokines. Phagocytosis by antigen presenting cells APC provides a strong control of detritus to detect invaders and prevent dangers for the host (Figure 1). Normally posttraumatic inflammatory reaction is aseptic and healing is reached in two to three weeks. In this period the detritus should be absorbed and the local homeostasis restored. Any disorder like hypoxia provokes the activation of local transient receptor potentials, acidosis by free radicals and cellular response. The innate immunity response persists with local perpetuation of vicious circles of aseptic inflammatory reactions. Representative cells for such reactions are the lymphocytes and especially the ubiquitous tissue homing natural killing T cells NKT. Owing their plasticity in different tissues they imply divers T cell receptors and are therefore named dNKT cells. They are self propagating and stimulate the building of neutrophils and B-cells beside extrusion of cytokine storm (Table 1).
Taking together the conclusion is to use lymphotoxic drugs to suppress lymphocytes in case of prolonged posttraumatic aseptic inflammatory reaction with clinical signs and symptoms locally around the trauma region.
Materials and Methods
For the first time nine consecutive out-patients with traumata of upper extremity or foot were treated because of persistent pain and restricted functionality of the traumatized extremity. Further details are provided in Table 3, the reader is requested to see there. As usual, venous oxygen pressure was high on the affected limb and lower on contralateral side [2,3]. Referring therapy there are several international communications [4,5], which recommend the use of GC generally in the case of perpetual inflammatory reactions. Different diagnoses from distinct clinical departments make it difficult to transfer this recommendation to Posttraumatic Dystrophy where damage of tissues triggers the inflammation. It is notable that most patients were affected by healthy conditions. Furthermore the aseptic posttraumatic inflammatory reactions are locally developed and maintained by innate immunity. Therefore the effectors of dNKT cells (Table 1) [6] were compared with the specific efficacy of GC analyzed in three pharmacological publications [7-10] (Table 2A and Table 2B). Nearly all cytokines and chemokines of dNKT effectors were blocked also the transcription factor iNOS, cellular immune response, T cell development and antigene presentation. Further transcription factors of the cytosolic pathway are suppressed and prevent the transcription of proinflammatory cytokines [10]. These results encouraged to use GC in posttraumatic patients with chronification of innate inflammatory reactions and typical PTD history (8 to 13 weeks of aggravation), clinical signs and symptoms (Table 3).
|
age (yr) |
m/fm |
trauma diagnosis |
PTD diagnosis after (wk) |
therapy with proved diagnosis PTD |
outcome 3 wk after therapy |
|
HAND (n = 7) |
|||||
|
59 |
m |
humerus fx left |
12 |
wrist free function, shoulder slightly limited |
|
|
72 |
fm |
dist. radius fx left |
9 |
free function |
|
|
59 |
m |
incision of carpal tunnel left |
10 |
glucocorticoid (GC) following circadian cycle of cortisol, schema see text |
free function |
|
62 |
fm |
dist. radius fx left |
8 |
physiotherapy, ergo therapy |
free function |
|
70 |
m |
avulsion of hamulus ossis hamati left |
12 |
impulse compression cuff during therapy free periodes |
improved hand function, wrist limited motion |
|
82 |
fm |
dist. forearm fx right |
8 |
wrist free, arthrosis of carpal art. sellaris |
|
|
64 |
m |
dist. radius fx right |
9 |
free function |
|
|
FOOT (n = 2) |
|||||
|
18 |
m |
metatarsal fx left |
11 |
free function |
|
|
ditto |
|||||
|
60 |
fm |
tarsal fx left |
13 |
free function |
|
Table 3: Patients: Nine consecutive patients with prolonged aseptic inflammatory reactions after traumatic incidence of the arm or foot were treated in the trauma department of affiliated Hospital of Medical School of University of Ulm in Immenstadt/Allgäu, Bavaria, Germany, leader Dr. A. Scola.
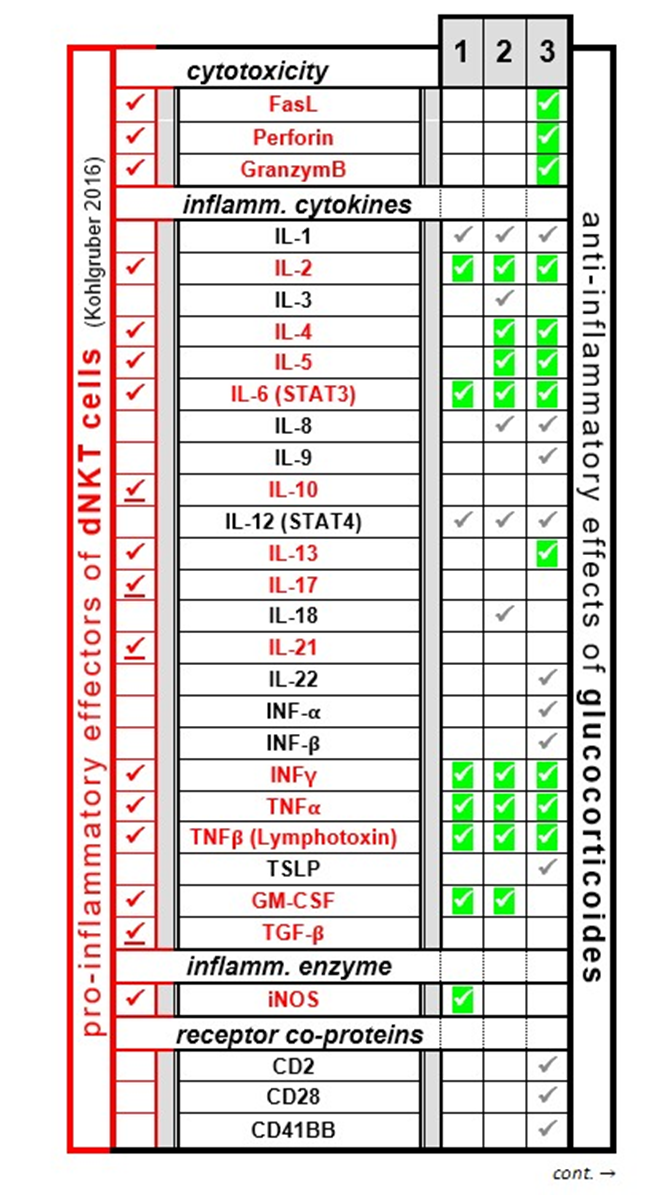
Table 2A
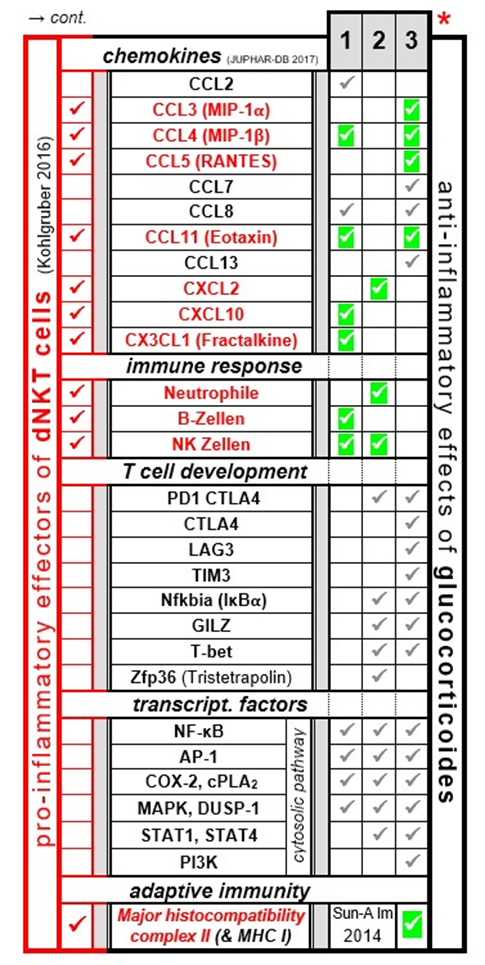
Table 2B
Table 2A and 2B: Comparison of activated dNKT cell effectors (red column, signs and terms,[6]) and their suppression by glucocorticoides (black column, signs and terms) with three pharmacologic articles 1: Czock 2005 [9], 2: Shimba 2020 [7,8], 3: Taves 2021 [10]. The majority of the activated dNKT cell effectors (25/29) are inhibited, only four cytokines out of 23 (indicated as ü: IL-10, IL-17, IL-21 and TGFβ) are not suppressed directly but indirectly reduced by impaired production of T helper cells. Coincidences are indicated as ü.. However, the activity of GC encompasses a large range of additional proinflammatory effectors (examples indicated as ü).
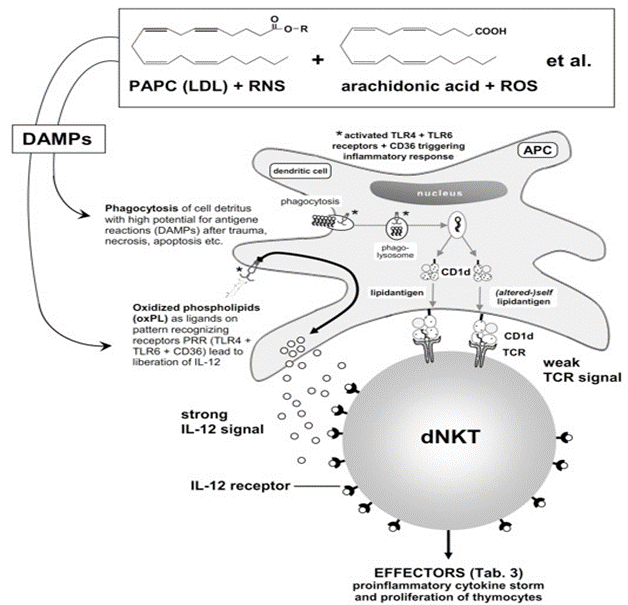
(Abrivation: PAPC 1-palmitoyl-2-arachidonyl-sn-glycero-3-phosphatidylcholine, LDL low density lipoprotein, RNS reactive nitrogen species, ROS reactive oxygen species, TLR toll-like receptor, CD cluster of differentiation)
Figure 1: (mod. based on [11] ): Schematic presentation of activation of dNKT cell through antigene presenting dendritic cell activated T cell receptor (weak) and strong IL receptor signal (IL-12, extruded form DC granules). Effectors see Table 3.
|
EFFECTORS of activated dNKT cell |
||
|
cytokines |
IL-1, IL-2, IL-3, IL-4, IL-5, IL-6, IL-8, IL-9, |
|
|
(IL-10), IL-12, IL-13, (IL-17), IL-18, IL-21, IL-22, INF-α, INF-β, INF-γ, TNFα, TNFβ (lymphotoxin), TSLP, GM-CSF, TGF-β |
||
|
chemokines |
CCL2, CCL3 (MIP-1α), CCL4 (MIP-1β), CCL5 (RANTES), CCL7, CCL8, CCL11 (Eotaxin), CCL13, CXCL5, CXCL10, CX3CL1 (fractalkine) |
|
|
enzyme |
iNOS |
|
|
cytotoxicity |
Fas-Ligand, Perforin, Granzyme B |
|
|
receptor co-proteins |
CD2, CD28, CD41BB |
|
|
enhanced immune responses |
neutrophils, eosinophils, T cells, B cells, NK cells, TH1 cells, macrophages M1, DC |
|
|
T cell development |
PD-1, CTLA4, LAG-3, TIM3, Nfkbia (IκBα), |
|
|
GILZ, T-bet, Zfp36 (tristetrapolin); |
||
|
cell-communication: Cx 32 |
||
|
enhanced Adaptive Immunity |
MHC I, MHC II |
|
|
transcription factors |
NF-κB, AP-1, COX-2, cPLA2, MAPK, |
|
|
(cytosolic pathway) |
DUSP-1, STAT1, STAT4, PI3K |
|
Table 1: Effectors of activated dNKT cell (cytokine storm) (6). Exocytosis starts about 30 min after activation due to innate microRNA of cytokins (INF-γ, IL-4) and lasts up to 2 days.
Treatment (consider contraindications) [9] The treatment with glucocorticoides (GC) was initiated with 80 mg a day for 4 days (à three doses each day in 8 hrs interval: 40 / 20 / 20 mg, following the circadian cycle of cortisol), 4 days à 40 mg (8 hrs interval 20 / 10 / 10 mg) and 4 days á 20 mg (8 hrs interval 10 / 5 / 5 mg). If necessary an extension of the therapy is possible even with higher doses.
Results
As expected the signs of aseptic inflammation disappeared in one to two days and the efficiency of physiotherapy increased. Never the less the glucocorticoid therapy was completed according to the scheme. With normal clinical findings after accomplished therapy the venous oxygen measurement was not controlled. No rebound phenomenon was observed.
Discussion
Enormous progress in immunology, namely aseptic inflammatory reactions after traumata by DAMPs [1] changed the point of view for effective treatment fundamentally. With PTD treatment common antiphlogistic drugs had no effects for too small specivity of action. In contrast the effectors of NKT cells are suppressed and blocked for a great amount with application of GC. The first indication of GC in PTD showed good clinical results. As prelimitary report further experience in this field is needed.
Conclusion
The insight into the nature of interplay between PAMPs and innate immunity allows a better understanding of aseptic inflammation after traumatic tissue lesions. The question about normal and atypical development becomes clearer answered actually. Cellular and humoral factors can work together in order to support the host in healing intentions. But sometimes gets the innate immunity irritated by molecules which were built by the host and provoke a long lasting inflammatory reaction. This bears the danger of creating antigens against host tissues, which leads to a disaster like PTD [12]. Therefore the necessity exists to battle against this complication as soon as possible. GC repress the lymphocytes and their effectors. First applications against immanent posttraumatic dystrophy showed very good results.
Acknowledgement: I would like to thank Dr. Alexander Scola who treated the out-patients.
Ethical Guidelines: Not applicable
Conflict of interest: The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Scola E (2025) Interplay of trauma-triggered auto-inflammatio and T-cell auto-reactivity in posttraumatic dystrophy. Front Immuol 16: 1404161.
- Scola A, Scola E (2013) Posttraumatic dystrophy. diagnosis and therapy after distal radius fractures and hand injuries. Unfall 116: 723732.
- Scola A, Scola E (2017) Reliability of venous blood gas analysis and radionuclide angiography in post-traumatic dystrophy. Unfall 120:501– 508.
- Kozin F, McCarty DJ, Sims J, Genant H (1976) The Reflex Sympathetic Dystrophy Syndrome. I. Clinical and Histologic Studies: Evidence for Bilaterality, Response to Corticosteroids and Articular Involvement. Am J Med 60: 321-331.
- Birklein F, Dimova (2017) Complex regional pain syndrome-up-todate. Pain Rep 2: e624.
- Kohlgruber AC, Donado CA, LaMarche NM, Brenner MB, Brennan PJ (2016) Activation strategies for invariant natural killer T cells. Immunogenetics 68: 649-663.
- Shimba A, Ikuta K (2020) Glucocorticoids Regulate Circadian Rhythm of Innate and Adaptive Immunity. Front Immunol 11: 2143.
- Shimba A, Ikuta K (2020) Control of immunity by glucocorticoids in health and disease. 5Seminars in Immunopathology 42: 669-680.
- Czock D, Keller F, Rasche FM, Häussler U (2005) Pharmacokinetics and Pharmacodynamics of Systemically Administered Glucocorticoids. Clin Pharmacokinet 44: 61-98.
- Taves MD, Ashwell JD (2021) Glucocorticoids in T cell development, differentiation and function. Nature Reviews Immunology 21: 233-243.
- Brigl M, Tatituri RVV, Watts GFM, Bhowruth V, Leadbetter EA, et al. (2011) Innate and cytokine-driven signals, rather than microbial antigens, dominate in natural killer T cell activation during microbial infection. J Exp Med 208: 1163-1177.
- Matzinger P (2022) Autoimmunity: are we asking the right question? Front Immunol 13: 864633.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.