Domaine-Specific Changes in Risk-Taking Propensity at Older Age – An Online Survey in a Danish Setting
by Nielsen JB1*, Andersen HS2
1Professor, Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark
2Statistician, Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark
*Corresponding author: Jesper Bo Nielsen, Professor, Research Unit of General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark
Received Date: 11 June, 2025
Accepted Date: 18 June, 2025
Published Date: 23 June, 2025
Citation: Nielsen JB, Andersen HS (2025) Domaine-Specific Changes in Risk-Taking Propensity at Older Age – An Online Survey in a Danish Setting. J Community Med Public Health 9: 523. https://doi.org/10.29011/2577-2228.100523
Abstract
Risk-taking propensity is reported to generally decrease with increasing age and be higher in males. Influence of age has, however, primarily focused on changes in early and midlife age. The present study aims at discussing associations between risk taking propensity and age and sex based on three 10-years groups of older Danish adults (age 51-80), and with a focus on characterizing associations observed within the fractions of the populations with lowest or highest risk-taking propensity. Materials & Methods: The present study is based on an online survey including three groups of older Danish adults (age 5180, N= 7,232 respondents), and with a focus on characterizing associations observed within the fractions of the populations with lowest or highest risk-taking propensities, respectively. We study generalized as well as domain-specific risk propensities. Questions were based on the validated German SOEP questionnaire. Results: We observe significant changes in risk propensity occurring during older age among females as well as males, but not similar changes, neither sex, direction, nor size-wise. We demonstrate a strong domain specificity related to changes in risk-taking propensity. In specific domains, the fraction of respondents with a high risk-taking propensity does not appear to decrease with increasing age. We find that stated domainspecific risk-taking propensity is significantly lower than stated general risk-taking propensity. Conclusion: The implications of our findings are that stated risk propensities to be used for guidance on policy or other regulations need to be domainspecific and need to be based on population-specific studies.
Keywords: Risk propensity; Age, Sex; Online survey; Domain specificity
Introduction
Decisions on risk-related behaviors are based on the information available, the degree to which the source of information is trusted, and on the individuals’ willingness to accept a risk. A number of factors are known to affect our propensity to take a risk [1,2]. Decisions may entail both positive and negative outcomes [3], and the size or importance of the outcomes may be rated individually. Thus, two individuals may, based on identical information, both argue that their decision is the best, despite presenting two different ‘best’ decisions. This has to do with the weight each individual put on each piece of information received, and their individual risk-taking propensity.
During recent years several papers have focused on changes in risk-taking propensity over lifetime [1,4]. A general observation appears to be that risk-taking propensity decreases with increasing age. Several theories have been discussed [2,4-6] with a focus on changes occurring during adolescence and early adulthood, where resource acquisition on several levels may be associated with the need for stronger risk-taking behavior [4,7,8]. Later in adulthood focus may change from collecting and establishing a good life to maintaining what has been accrued and avoiding loss, i.e. supporting a more risk averse behavior [4,9,10]. These thoughts or theories appear to be founded in more materialistic priorities, but other studies indicate that in domains associated with physical ability and health, there appears to be a perhaps not surprising higher propensity for risk taking in the younger age groups, where the absolute risk for adverse outcomes is known to be lower [11]. Domain specific risk-taking propensity data may offer more nuanced analyses on individual factors affecting stated risk-taking propensities [1,3].
Sex is the other frequent source for variation in risk-taking propensity studied, and the findings are often generalized to conclusions that women are more risk averse than men, but without much analytical focus on potential combined sex-, age- and domain-specific differences [4,12].
The influence of age on risk taking propensity appears to have mainly focused on changes during adolescence and early adulthood [3]. An often-used argument being that significant changes in life occurs during these periods of life. While this is true, equally large changes in people’s life situation occurs dung older age. Changes in risk taking propensity among people above 60 years-of-age appear to vary in domain-specific ways [12]. With a continuing increase in the fraction of people aged 50-80 years-of-age, this period of life deserves more attention. Important decisions are made during these years related to retirement and financial stability (pension) during older age, and during the same period people become frailer and the statistical absolute risk for disease increases [11,13]. This paper will therefore focus on changes in later life covering the age span from 50 to 80 years of age.
It could be argued that the preferred method to study age-related changes in risk taking propensity over time would be to follow the same individual repeatedly over a period of years. However, individual risk-taking propensities related to different domains are expectedly susceptible to external factors like the Covid-19 pandemic [14,15], financial crisis, war, personal disease etc., and such influence would potentially challenge comparisons of propensities measured longitudinally at different time points. Further, and for practical reasons, it would take a long time to collect data on age-related changes covering a 30-years period. We therefore choose a trans-sectional approach comparing risk taking propensities in three age cohorts sampled at the same time.
Propensity measures have repeatedly been shown to vary considerably between individuals with some fraction of a population being very risk averse, while in the same population another fraction show a high willingness to take risks. There is a risk that such differences within a population may not be identified if analysis and comparisons are based on mean or median values only. The focus in this paper is therefore not on the median or average risk-taking propensities but on understanding and characterizing those individuals belonging to the highest or lowest fractiles of the population related to risk taking propensity.
Risk taking propensity (‘how do you see yourself – are you generally a person willing to take a risk or do you try to avoid taking a risk?’) will be evaluated in general as well as in 6 domains related to driving, economy, sport and leisure activities, job situation, trust in other people, and own health based on questions originally developed, validated, and used in the German SocioEconomic Panel Studies (SOEP, www.leibniz-soep.de).
The present study aims at discussing associations between risk taking propensity and age and sex based on three 10-years groups of older Danish adults (age 51-80), and with a focus on characterizing associations observed within the fractions of the populations with lowest or highest risk-taking propensity. Our expectation is that the stated risk-taking propensity will vary with age among both the most and the least risk averse participants, but also that their response will be domain dependent.
Materials & Methods
We used a cross-sectional survey design based on a representative group of 15,072 Danish citizens aged 51-80 years. Data was collected in 2019 through a web-based standardized questionnaire (digital mail) administered by Statistics Denmark. Two reminders were sent through digital mail. Among the net sample, 7,232 persons (48%) returned a questionnaire on topics related to risk propensity.
Risk-taking propensity was reported on an eleven-point Likert scale (0 = not willing to take a risk; 10 = full willingness to take a risk). Based on the lowest and highest quartiles of the answering categories, respectively, a low risk-taking propensity (answering 0, 1, or 2 on the Likert scale) and a high risk-taking propensity (answering 8, 9, or 10 on the Likert scale) were compared.
Statistical analyses
To test for associations between age, sex, and risk willingness, a chi-squared test was used. First, it was used to test for associations between age group, and low (or high) risk willingness and not having low (or high) risk willingness, stratified by gender. Secondly, we used a chi-squared test to test for associations between gender (male, female) and low (or high) risk willingness. All tests were done for general risk willingness and for each of the six domains. All analysis was done using Stata version 18 (StataCorp LP, College Station, TX, USA).
Ethics
According to the Act on a Biomedical Research Ethics Committee System in Denmark, the project was not a biomedical research project and did not need the ethic committee’s approval. Data include information that could potentially identify individuals, and the project is therefore registered at the University’s Research and Innovation Office, and data handling is in accordance with the General Data Protection Regulation (GDPR) from (EU) 2016/679.
Results
With 7,232 persons responding to our questionnaire, we received a response rate of 48% and a representative sample compared with the Danish population with only slightly overrepresentation of female respondents and respondents aged 61-70 year-of-age (Table 1).
|
Respondents; N (%) |
Net sample; N (%) |
DK population; (%) |
|
|
Sex |
|||
|
Female |
3806 (52.6%) |
7695 (51.1%) |
(50.9%) |
|
Age |
|||
|
51-60 |
2832 (39.2%) |
6375 (42.3%) |
(42.3%) |
|
61-70 |
2641 (36.5%) |
4877 (32.4%) |
(32.1%) |
|
71-80 |
1759 (24.3%) |
3820 (25.4%) |
(25.6%) |
Table 1: Sample characteristics (sex and age distribution) of the study group of Danish citizens aged 51-80 years.
The average risk propensity scores related to general risk taking (non-domain-specific) were 5.7, 5.7, and 5.5 on the 11-point Likert scale in the three age groups ranging from age 51-60, 61-70, and 71-80, respectively (data not shown). Thus, based on average scores, the influence of increasing age from age 51 and upwards toward 80 on general risk-taking propensity was limited.
However, a more nuanced picture was seen when focusing on the subpopulations with the most (Likert score 0, 1, and 2) and the least (Likert score 8, 9, and 10) risk averse respondents. With increasing age, a significantly larger faction of females (p<0.001) shifted into the most risk averse group (Likert score 0, 1, and 2) (Figure 1). The fraction of males also increased, but not statistically significant (p=0.09). Among males and females with the highest stated general willingness to take a risk (Likert score 8, 9, and 10), the prevalence did not change significantly over the three age decades (Figure 1). The findings indicate significant changes in risk propensity occurring during older age, but not similar changes, neither sex, direction, nor size-wise (Figure 1).
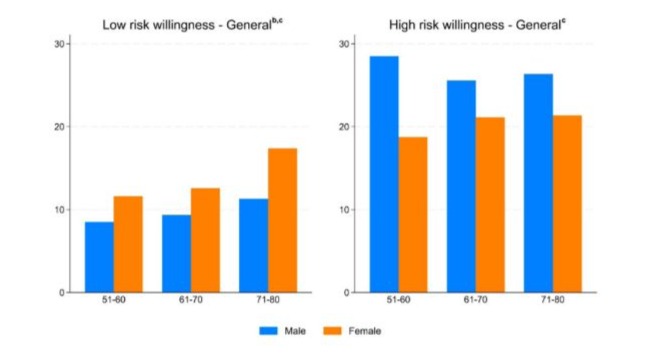
Figure 1: Risk-taking propensity (per cent of respondents) among 51-80-years old respondents with low (Likert scores 0, 1, 2) or high (Likert score 8, 9, 10) general risk willingness. a – significant increase with age, male; b - significant increase with age, female; c – significant difference between males and females. Level of significance was set at p<0.05.
Compared to the stated domain-specific risk propensities (e.g. health and trust), a significantly smaller fraction of the respondents’ state that they in general belong to the most risk averse individuals (0, 1, or 2 on the Likert scale). Likewise, a high-risk willingness (8-10 on the Likert scale) is stated by 23% of our respondents related to the general and unspecified risk domain, whereas a significantly lower fraction of the respondents state this high-risk willingness when it comes to domain-specific risk scenarios (health 4%; trust 17%). Thereby demonstrating a strong domain specificity when it comes to risk-taking propensity (Figure 2).
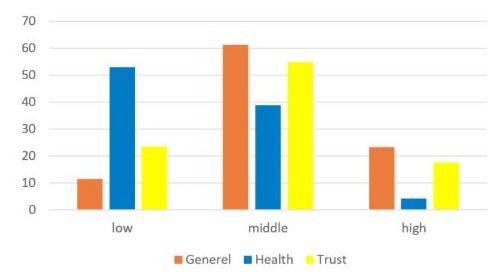
Figure 2: Distribution of risk-taking propensities (per cent of respondents) between respondents with low (Likert scores 0, 1, 2), middle (Likert scores 3-7), and high (Likert score 8, 9, 10) risk willingness in general and in the health and trust domains.
Across all six tested risk domains and across all three age decades included, a higher fraction of the female than the male population, stated that they had a low risk-taking propensity (p<0.001). Across all six tested risk domains and for males as well as females the fraction of respondents stating a low risk-taking propensity increased with increasing age (p<0.05; Figure 3).
Within the group of respondents stating a high risk-taking propensity, the response was more nuanced and domain specific. Regarding sport and leisure activities as well as in the domain of job and labor marked, the fraction of both male and female respondents stating high risk-taking propensity decreased with increasing age from 51 to 80 years-of-age (p<0.001; Figure 3).
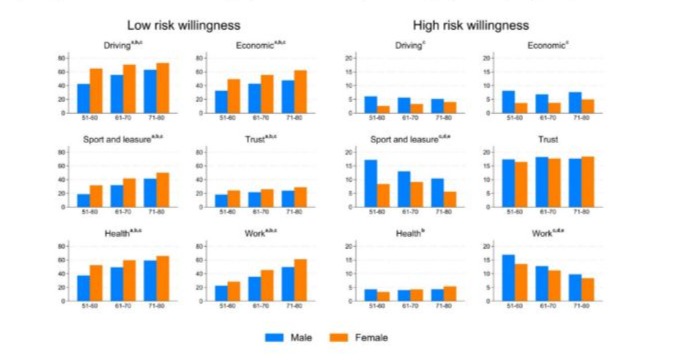
Figure 3: Risk-taking propensity (per cent of respondents) among 51-80-years old respondents with low (Likert scores 0, 1, 2) or high (Likert score 8, 9, 10) domain specific risk willingness. a – significant increase with age, male; b - significant increase with age, female; c – significant difference between males and females; d - significant decrease with age, male; e - significant decrease with age, female. Level of significance was set at p<0.05.
A relatively high fraction of our respondents (16-18%) stated that they had high trust in other people by rating their individual risk-taking propensities in this domain between 8 and 10 on the Likert scale. These numbers did not change significantly across the included age groups (p=0.4-0.8), and both genders responded similarly with a high risk-taking propensity towards trusting other people (Figure 3).
A limited fraction of our respondents (less than 8%) stated a high willingness to accept risks related to driving, economy, and health. Within the domains of driving and economy, the risktaking propensity decreased slightly with increasing age among male respondents, whereas it in contrast increased slightly, but insignificantly (p=0.13) when female respondents got older (Figure 3). In the domain related to the willingness to take risks related to your own health, around 4% of the male respondents, irrespectively of age, stated a high risk-taking propensity. Female respondents stated a slightly lower risk-taking propensity in this domain in the youngest of our age groups (3.2% among 51-60 years old), but the risk-taking propensity increased by more than 50% (p=0.05) with increasing age and reached 5.4% in the oldest age group. There was a significant difference in risk-taking propensity in the health domain among females and males (Figure 3).
Discussion
Our data demonstrate that stated domain-specific risk-taking propensity is significantly lower than non-specific, general risktaking propensity. Further, that domain specific risk propensity can be country specific. Eventually, we demonstrate that within some risk domains the expected diminishing risk propensity with increasing age cannot be found in our Danish population aged 5180 years-of-age. The implications of these findings are that stated risk propensities used for guidance on policy or other regulations need to be domain-specific and need to be based on populationspecific studies.
It is a strength that our net sample is very similar to the Danish population, and that our respondents have almost identical age and sex distribution as the net sample. Further, it is a strength that we have a solid sample size with more than 7,000 respondents that allow for relevant subgroup analyses. It is a limitation for the representativity of our findings that the Danish population on average is better off financially as well as health-wise than many other countries - till example all Danes receives a state-paid pension from age 67, and most health care is free. It is an inherent limitation with self-reported data that we do not know how well the stated propensities align with real world behavior.
The average risk propensity score for general risk taking demonstrated limited change with increasing age. In contrast, more nuanced information emerged when focusing on the subgroups with lowest and highest risk-taking propensity. The literature describes a reduced risk-taking propensity with increasing age [4,6,9] indicating a shift to the left on the Likert scale distributions. This is also clear in the lowest risk propensity group for males as well as females with a significant trend over time for an increasing fraction of the population moving into this group. For the 20-25% of the population with a high stated risk propensity at age 51-60 the situation is, however, less clear as the expected decrease reflecting the increased fraction of low risk propensity respondents does not occur. For female respondents, the fraction of the population stating high risk propensity slightly increase and almost eliminates the sex difference that is often stated in the literature to be general across all ages [4,12]. Thus, our more nuanced data analysis shows that those respondents that are least risk adverse at age 51-60 keep this stated behavior during subsequent decades of aging, and that sex differences in risk propensity diminish at older age.
About 5-10% and 20-25% of our populations stated their general risk propensity as low or high, respectively. Our data from 6 different risk domains demonstrate very different and clearly domain-specific risk propensities. Generally, most respondents state a significantly lower risk-taking propensity when asked to state a domain-specific risk propensity than when asked to state their general risk propensity. A similar observation is evident in the high-risk propensity groups, where risk taking propensity is generally higher when the risk domain is unspecific. These observations suggest that general risk propensity assessments are too unspecific, and that domain-specific analyses are needed for a more correct assessment of an individual’s risk-taking propensity.
The domain with the lowest fraction of our Danish population across age and sex stating low risk willingness, and the highest fraction stating high risk-taking propensity, was related to trust in other people. This domain is probably sensitive to the society, country, local crime statistics etc., and our findings are not unexpected in a Danish setting characterized by a high degree of societal homogeneity, and where citizens generally demonstrate very high trust in other people as well as authorities (https://ourworldindata. org/grapher/self-reported-trust-attitudes?time=2022). Risk propensity related to trust in other people appears to vary significantly between populations/countries with societal homogeneity as an important factor [16,17]. Trust being perhaps a more general, intrinsic, and value-based thing may also explain why changes with increasing age in the high willingness groups if anything, and in accordance with the literature [16], is increasing.
Both financial income and health changes to become a more limited and fragile resource for most people when they get older. Thus, it is not unexpected, and in line with the existing literature [1], that the fraction of people with a low willingness to take risks related to economy and personal health increased from 30-50% among 51-60 years-old to around 60% among respondents between 71 and 80 years-of-age. As already mentioned above, these domainspecific risk aversities are significantly higher than those given for unspecified risk aversity. An interesting finding here is, however, that the fraction (4-6% across genders) of respondents stating a high willingness to take risks related to economy and personal health does not decrease with increasing age– for females it actually increases. The finding could be explained by the increasing life expectancy over the last decades, where an increasing fraction of the Danish/Northern European populations keep at good health for longer [18], and likewise that a certain fraction of the population has accrued sufficient economy through their working life to enable them to continue with comparable economy even after retirement due to individual and governmental supported pensions, investments etc. The implications of this finding could be significant for the insurance and pension business. It should, however, not be overseen, that the by far largest group of respondents state an increasing risk aversity that could perhaps be seen as worry for their economic as well as health situation in their older age.
Placing our findings in a broader public health and policy framework means that initiatives either dependent upon or intended to change risk behavior among the growing fraction of elderly will need to consider that this group of citizens not necessarily have the same perceptions of risk than younger citizens, and that a significant scenario-dependent variability exists between risktaking propensities. To avoid unintended worries related to risk scenarios with an already very high focus among most elderly such as economy or health issues, a more targeted approach to publicly issued risk communication/campaigns directed towards elderly may be needed.
References
- König AN (2021) Domain-specific risk attitudes and aging—A systematic review. Behav Dec Making 34: 359-378.
- Frey R, Richter D, Schupp J, Hertwig R, Mata R (2021) Identifying robust correlates of risk preference: A systematic approach using specification curve analysis. J Pers Soc Psychol 120: 538-557.
- Fryt J, Szczygiel M, Duell N (2022) Positive and negative risk-taking: age patterns and relations to domain-specific risk-taking. Advances in Life Course Research 54: 100515.
- Liu Y, Bagaïni A, Son G, Kapoor M, Mata R (2023) Life-Course Trajectories of Risk-Taking Propensity: A Coordinated Analysis of Longitudinal Studies. J Gerontol B Psychol Sci Soc Sci 78: 445-455.
- Düzel E, Bunzeck N, Guitart-Masip M, Düzel S (2010) Novelty-related motivation of anticipation and exploration by dopamine (NOMAD): implications for healthy aging. Neurosci Behav Rev 34: 660-669.
- Dohmen T, Falk A, Golsteyn BHH, Huffman D, Sunde U (2017) Risk attitudes across the life course. The Economic Journal 127: F95-F116.
- Defoe IN, Dubas JS, Figner B, van Aken MAG (2015) A meta-analysis on age differences in risky decision making: Adolescents versus children and adults. Psychol Bull 141: 48-84.
- Mata R, Josef AK, Hertwig R (2016) Propensity for risk taking across the life span and around the globe. Psychological Science 27: 231243.
- Depping MK, Freund AM (2011) Normal aging and decision making: The role of motivation. Human Development 54: 349-367.
- Bleidorn W, Klimstra TA, Denissen JJA, Rentflow PJ, Potter J, et al. (2013) Personality maturation around the world: a cross-cultural examination of social-investment theory. Psychol Sci 24: 2530-2540.
- Chang AY, Skirbekk VF, Tyrovolas S, Kassebaum NJ, Dieleman JL (2019) Measuring population ageing: an analysis of the Global Burden of Disease Study 2017. Lancet Public Health 4: e159-e167.
- Josef AK, Richter D, Samanez-Larkin GR, Wagner GG, Hertwig R, et al. (2016) Stability and change in risk-taking propensity across the adult lifespan. J Pers Soc Psychol 111: 430-450.
- Bai G, Wang Y, Mak JKL, Ericsson M, Hägg S, et al. (2023) Is Frailty Different in Younger Adults Compared to Old? Prevalence, Characteristics, and Risk Factors of Early-Life and Late-Life Frailty in Samples from Sweden and UK. Gerontology 69: 1385-1393.
- Bruine de Bruin W (2021) Age differences in COVID-19 risk perceptions and mental health: evidence from a national U.S. survey conducted in March 2020. J Gerontol B Psychol Sci Soc Sci 76: e24-e29.
- Pasion R, Paiva TO, Fernandes C, Barbosa F (2020) The age effect on protective behaviors during the COVID-19 Outbreak: sociodemographic, perceptions and psychological accounts. Front Psychol 11: 561785.
- Li T, Fung HH (2013) Age differences in trust: An investigation across 38 countries. J Gerontol B Psychol Sci Soc Sci 68: 347-355.
- Beugelsdijk S, Klasing MJ (2016) Diversity and trust: The role of shared values. J Comp Economics 44: 522-540.
- Nielsen CR, Ahrenfeldt LJ, Jeune B, Christensen K, Lindahl-Jacobsen R (2021) Healthy life expectancy by frailty state in Europe from 2004 to 2015: findings from SHARE. Eur J Publ Health 31: 554-560.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.