Direct Carotid Puncture as a Bailout Technique for Mechanical Thrombectomy and Carotid Artery Stent in Tandem Occlusion Stroke and Extreme Vascular Anatomy
by Giancarlo Salsano1*, Bruno Del Sette1, Davide Sassos2, Alessandra Murialdo2, Massimo Del Sette2, Lucio Castellan1
1UOC Neuroradiologia. IRCCS Azienda Ospedaliera Metropolitana, Genova, Italy
2Neurology and Stoke Unit, RCCS Azienda Ospedaliera Metropolitana, Largo Rosanna Benzi, 10, 16122, Genoa, Italy
*Corresponding author: Giancarlo Salsano, Department of Radiology and Interventional Radiology, RCCS Azienda Ospedaliera Metropolitana, Largo Rosanna Benzi, 10, 16132, Genoa, Italy
Received Date: 24 November 2025
Accepted Date: 29 November 2025
Published Date: 03 December 2025
Citation: Salsano G, Del Sette B, Sassos D, Murialdo A, Del Sette M, et al. (2025) Direct Carotid Puncture as a Bailout Technique for Mechanical Thrombectomy and Carotid Artery Stent in Tandem Occlusion Stroke and Extreme Vascular Anatomy. Ann Case Report. 10: 2459. DOI: https://doi.org/10.29011/2574-7754.102459
Case Presentation
An 81-year-old man presented with left-sided hemiparesis and dysarthria upon awakening, consistent with a wake-up stroke. He had a history of coronary artery disease, previous minor stroke due to right carotid artery stenosis managed with endarterectomy and chronic peripheral vascular disease treated with an aortobifemoral bypass. Computed tomography (CT) showed no early signs of ischemia (Figure 1A), but demonstrated occlusion of the right internal carotid artery (ICA) along with distal occlusion of the middle cerebral artery (MCA) (Figure 1B). CT perfusion imaging revealed a large ischemic penumbra, estimated at 136 mL (Figure 1C). Diagnostic angiography was performed via puncture of the right aortofemoral graft (Figure 2A), confirming right ICA occlusion with poor collateral flow from the contralateral carotid circulation (Figures 2B-C). Severe calcified stenosis at the origin of the right common carotid artery (CCA) precluded mechanical thrombectomy (MT) via both femoral and radial access routes (Figures 2D-E).
Under general anesthesia and ultrasound guidance, direct puncture of the right CCA was performed approximately 2 cm above the clavicle. A 0.025” wire was advanced toward the external carotid artery. After needle removal, a 6F thin-wall sheath (Glidesheath Slender; Terumo Medical, Somerset, NJ, USA) was inserted into the right CCA. A 0.014” guidewire was then placed into the right ICA, followed by balloon angioplasty using a 4×20 mm catheter.
MT was performed using a 4×28 mm stent retriever (Trevo NXT ProVue Retriever, Stryker, CA, USA) in combination with a distal aspiration catheter (Catalyst 6F, Stryker, CA, USA), resulting in complete MCA recanalization (Figures 3A-C). Following the procedure, recurrence of carotid stenosis was observed. To restore and maintain carotid blood flow, a 5×30 mm carotid stent (Wallstent, Boston Scientific, Santa Clara CA, USA) was deployed (Figure 3D). Hemostasis at the carotid access site was achieved with an Axiostat patch (Axio Biosolutions Pvt. Ltd., Gujarat, India) and 5 minutes of light manual compression (Figure 3E). Follow-up CT revealed a small insular infarction and a minimal subarachnoid hemorrhage in the right Sylvian fissure. The carotid stent remained patent, with no complications observed (Figures 4A-C).
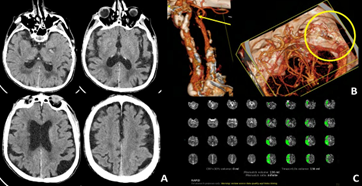
Figure 1: CT showed no early signs of ischemia (A). CT angiography pointed out tandem occlusion of right ICA and distal M2 segment of MCA (yellow arrow and circle; B). No ischemic core was found on perfusion imaging (C).
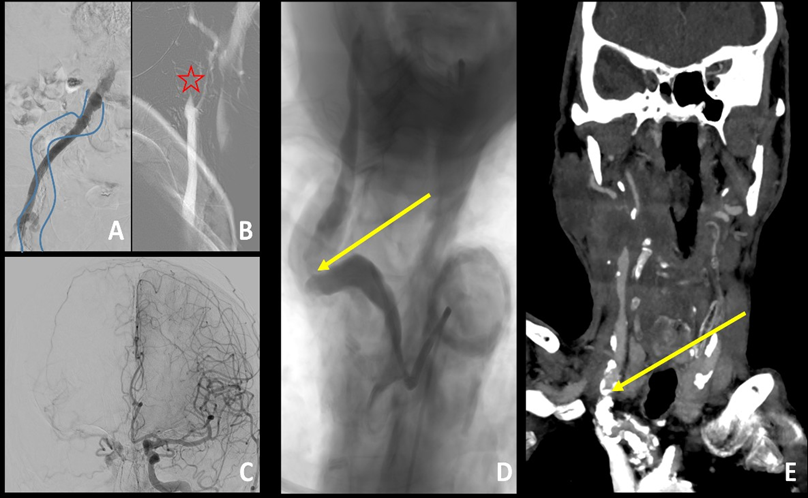
Figure 2: Diagnostic angiography was performed via puncture of the right aortofemoral graft (native femoral artery was underlined by blue curved lines; A). It confirmed occlusion of right ICA (red star; B) with poor collateral circulation from contralateral carotid artery (C). Moreover severe calcific stenosis at origin of CCA (yellow arrow; D-E) was identified.
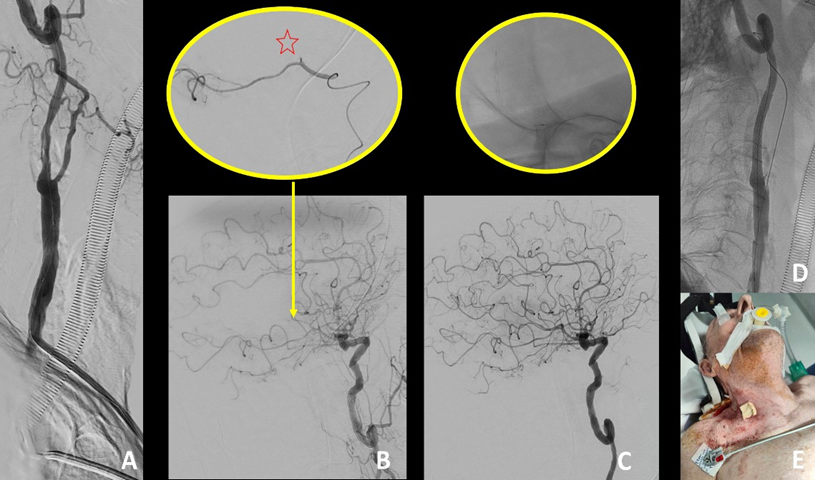
Figure 3: Mechanical thrombectomy and carotid stent deployment via direct CCA approach was performed (A-D). Hemostasis of the cervical access was obtained through chitosan-based patch (E).
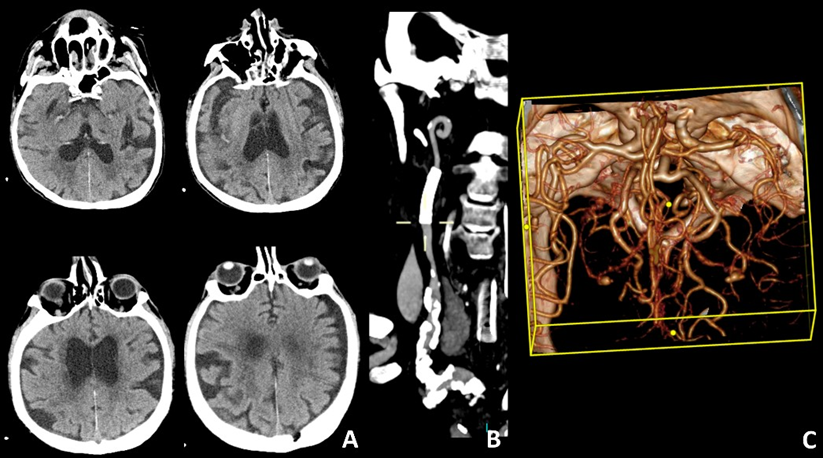
Figure 4: CT follow-up at 1 week (A-C).
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.