Differential Diagnosis of Otorhinolaryngological Disease with Temporo-Mandibular Joint (TMJ) Dysfunction
by Tonuzi Orjeta1, Alketa Qafmolla2*
1Doctor of Sciences, University Hospital Center, Tirana, Albania
2Associate Professor, Faculty of Dental Medicine, Tirana, Albania
*Corresponding author: Alketa QAFMOLLA, Associate Professor, Faculty of Dental Medicine, Tirana, Albania
Received Date: 19 December, 2024
Accepted Date: 27 December, 2024
Published Date: 31 December, 2024
Citation: Orjeta T , Qafmolla A (2024) Differential Diagnosis of Otorhinolaryngological Disease with Temporo-Mandibular Joint (TMJ) Dysfunction. Dent Adv Res 9: 209. https://doi.org/10.29011/2574-7347.100209.
Abstract
The anatomical proximity of the ear to the Temporo-Mandibular Joint can confuse the localization of pain caused in that area [1]. This affair is the reason why patients with TMJ dysfunction often present to the Otorhinolaryngological doctor for ear problems [11,12].
They complain of ear pain, ringing in the ear, the feeling of blockage in the ear, dizziness, etc. Pain and the feeling of blockage in the ear are often the symptoms complained of by patients with middle ear damage. Tinnitus, dizziness are the symptoms of patients with vestibular pathology and Meniere’s syndrome, etc. [12,13]. Pain, which is the most frequent symptom, is also referred by the patient in a state of rest, which differentiates it from joint pain, which is aggravated during the movement of the lower jaw, called the mandible.
In order to make the differential diagnosis of Otorhinolaryngological disease with TMJ dysfunction, two individual groups of patients were selected and involved for our study. The first group consisted of 60 individual patients with Otorhinolaryngological pathology and the second group consisted of 211 patients with dysfunctional of TMJ disorders.
The results of the study showed that in both study groups, women predominate, respectively with 53.3% (32 individual patients) of all cases, while in the second group with 78.7% (166 individual patients). Earaches can appear at any age, which according to statistical analysis shows that there is a statistically significant relationship after P=0.041, while for the thymus the results of the study show that there is no statistically significant relationship after P=0.275.
Keywords: Tinnitus; Dizziness symptoms; Dysfunction of TMJ; Earaches; Thymus; Trigeminal nerves.
Introduction
The Temporo-Mandibular Joint is affected by various pathologies. The most frequent pathology encountered in daily practices are the dysfunctional disorders of this system. Different pathologies appear in the stomatognathic apparatus, the consequences of which reflect in the TMJ system [1]. The number of studies on the dysfunctional pathology of the TMJ is quite wide, the more rightly the discussion of this problem with contemporary literature is justified [2,3].
The problem of differential diagnosis of TMJ dysfunction with other pathologies of the stomatognathic apparatus is even greater today [4,5]. There are pathologies such as Otorhinolaryngological pathologies, arterial hypertension, migraine, sponoliarthrosis etc., which reflect similar to pain in the TMJ joint.
In daily practice, it is of particular importance to make a differential diagnosis of pain in the TMJ with diseases of Otorhinolaryngology. The anatomical proximity of the ear to the Temporo-Mandibular Joint can confuse individual patients to localize the pain happened in that region.
Ear pain is perceived more posteriorly (on the side) than pain in the TMJ joint. This is explained by the fact of their anatomical proximity to each other, but also due to the innervation from the same nerve, mandibular branch and trigeminal nerve. This anatomical afference with the same phylogenetic inheritance and nerve innervation, can confuse the patient’s ability to localize the pain caused in that area [14,15].
The differential diagnosis must be made through a very careful anamnesis, as well as through imaging with a scanner or magnetic resonance. Among the symptoms that differentiate any Otorhinolaryngological pathology is another way of differential diagnosis with that of TMJ pathology.
The differential diagnosis of Ear Diseases from dysfunction in the Temporo-Mandibular Joint is made through these symptoms:
1] Absence of pain during jaw movement; 2] Lack of jaw movement limitation; 3] Absence of mouth opening difficulties.
Meniere’s Syndrome has the following symptoms:
a] Thinking; b] ringing in the ears; c] decrease in hearing up to complete deafness with or without nystagmus.
The main purpose of the study is: Let’s do it by determining the differential diagnosis of the Ear Pathology with the TemporoMandibular Joint dysfunction-TMJD.
Objectives of the study
1] To explain, what are the symptoms that differentiate Ear Diseases from Temporo-Mandibular Joint Dysfunction (TMJD) ?
2] To determine, which are the most frequently used methods for the treatment of each of the pathologies found ?
Material and method
From 2022-2024 period, 60 patients aged 6-78 years old were examined and treated with Otorhinolaryngological pathology of ear pain. Of these patients, 32 (53.3%) of the cases were female and 28 (46.7%) were male. We made the differential diagnosis with a group of 211 individual patients with TMJ dysfunction.
The Otorhinolaryngological pathology was treated by the relevant specialist, while the TMJ dysfunction was performed by a specialist dentist through combined medical-prosthetic treatment.
The results
In this study, 60 individual patients with Otorhinolaryngological pathology of the ear were involved, who completed the questionnaire, specially prepared for the above period of time. The statistical analysis of the data collected was processed using the SPSS program (Statistical Package for Social Sciences), improved version 21.0.
We made the differential diagnosis with the dysfunctional pathology of the TMJ, which we carried out with the investigation of 211 students of “ALDENT” University, Tirana. About, 60 individual patients were treated in the Otorhinolaryngology department near the University Hospital Center, Tirana, and about 32 individual patients were female, while 28 individual patients were male.
Table 1 shows the distribution of the individual patients involved in the study in relation to gender. From the results of the study, it is noted that 32 (53.3%) of the individual patients declare that they were women, and 28 (46.7%) of the individual patients were men. These data are presented in more detail in the table 1 and graph 1, as below.
|
Gender |
Number of individual patients |
Percentage % |
|
Female |
32 |
53.3 |
|
Male |
28 |
46.7 |
Table 1: Distribution of patients included in the study in relation to gender.
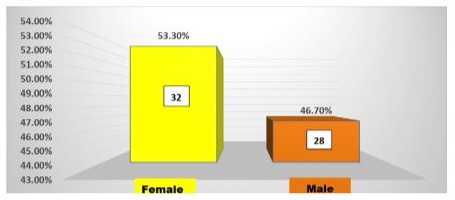
Graph 1: The distribution of patients included in the study in relation to gender.
|
Gender |
Presence of TMJ pain |
P-values |
|
Female |
166 (78.7 %) |
|
|
Male |
45 (21.3%) |
Table 2: The distribution of patients included in the study in relation to gender according to TMJ pathology.
• Absolute value and % in brackets; £=is the value of P according to the chi-square test.
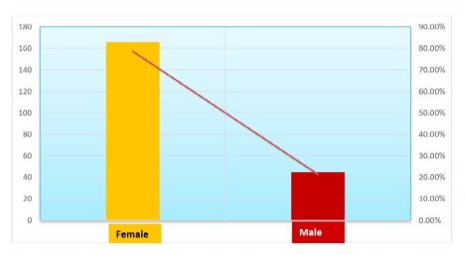
Graph 2: The distribution of patients included in the study in relation to gender according to TMJ pathology.
The symptoms of patients with Otorhinolaryngological pathology were pain in the ears and the area around them, Tinnitus, Dizziness, etc. From our study, it results that about 36 (60%) of the individual patients have declared that they have earaches, while 24 (40%) of the individual patients have declared that they have not earaches, which data are presented in table and graph 3.
|
Ears pain |
Number of individual patients |
Percentages % |
|
Yes |
36 |
60 |
|
No |
24 |
40 |
Table 3: Distribution of patients included in the study regarding earaches.

Graph 3: The distribution of patients included in the study regarding earaches.
Another symptom that differentiates the pathologies of earaches is Tinnitus, and from the data collected in our study it is shown that 22 (36.7%) of the individual patients declared that they were affected by Tinnitus, while 33 (55%) of the individual patient did not have this symptom and 5 (8.3 %) individual patients declared that they had Tinnitus with lower audition.
|
Tinnitus symptoms |
Number of individual patients |
Percentages % |
|
Tinnitus |
22 |
36.70% |
|
no Tinnitus |
33 |
55% |
|
Tinnitus with lower audition |
5 |
8.30% |
Table 4: Distribution of patients included in the study regarding the presence of Tinnitus.
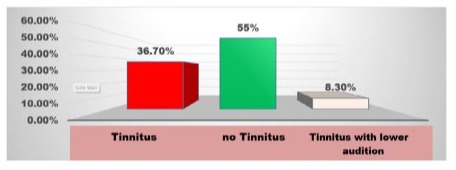
Graph 4: Distribution of patients included in the study regarding the presence of Tinnitus.
The study included individual patients who, in addition to the above symptoms, also complained of headaches. Thus, from the table and graph 5, it can be seen that 17 (28.3) individual patients had complained of constant headache.
|
Headache |
Number of individual patients |
Percentages % |
|
Yes |
17 |
28.30% |
|
No |
43 |
71.70% |
Table 5: Distribution of patients included in the study regarding headache.
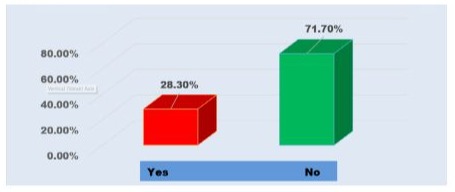
Graph 5: Distribution of patients included in the study regarding headache.
Brainstorming and loss of balance were other important symptoms that individual patients had declared in the distributed questionnaire, and the data of these symptoms are presented in table and graph 6.
|
Brainstorming |
Number of individual patients |
Percentages % |
|
|
Yes |
15 |
25% |
|
|
No |
43 |
75% |
Table 6: Distribution of patients included in the study regarding brainstorming.
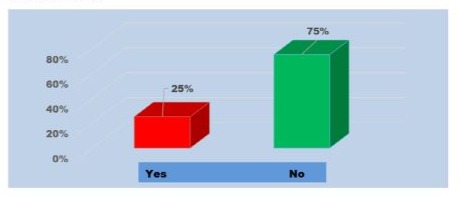
Graph 6: Distribution of patients included in the study regarding brainstorming.
Earaches can appear at different ages, starting from the youngest age of 6 years and continuing to the older ages, going to 78 years old, which data collected according to the questionnaire distributed among patients and which are shown in the table and graph 7.
|
Variables |
Yes |
No |
P-values |
|
Individual patients 6-43 years |
15 (41.7%) |
4 (16.7%) |
|
|
Individual patients 43-78 years |
21 (58.3%) |
20 (83.3%) |
P=0.041£ |
Table 7: Relationship between age and earaches.
- Absolute value and percentage in brackets; £ value of P according to the chi-square test.
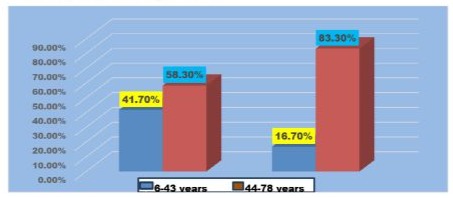
Graph 7: The relationship between age and earaches.
Table and graph 7 show the relationship between age and earaches. From the results of the study, it can be seen that there is a statistically significant relationship as P=0.041
Tinnitus can appear at any age, which our study also shows, since according to the value of P=0.275, it is shown that there is no statistically significant relationship between these two variable variables.
|
Variables |
Tinnitus |
No Tinnitus |
Tinnitus with lower |
Vlera e P |
|
Individual patients 6-43 years |
8(36.4%) |
11(33.3%) |
0(0.0%) |
|
|
Individual patients 44-78 years |
14(63.6%) |
22(66.7%) |
5(100%) |
P=0.275£ |
Table 8: Relationship between age and Tinnitus.
- Absolute value and percentage in parentheses, £ p-value according to the chi-square test
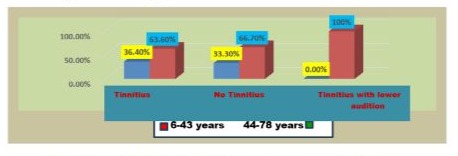
Graph 8: The relationship between age and Tinnitus.
Headache as shown in the table and graph 9 can also appear at any age. Based on the statistical analysis according to the SPSS system (improved version 21), it is clear that there is no significant statistical relationship between age and headache as the values of P=0.813, the data of which are reported as below
|
Variables |
Yes |
No |
P-values |
|
Individual patients 6-43 years |
5 (29.4%) |
14 (32.6%) |
|
|
Individual patients 4478 years |
12 (70.6%) |
29 (67.4%) |
P=0.813 £ |
Table 9: Relationship between age and headache.
- absolute value and percentage in parentheses, £ p-value according to the chi-square test
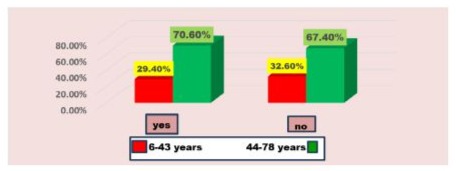
Graph 9: The relationship between age and headache.
Brainstorming and losses of subconscious and equilibrium were other important symptoms that individual patients have declared in the distributed questionnaire, and the data of these symptoms are presented in table and graph 10, and, as seen from these above data, there is no statistically significant relationship between age, and losses of subconscious and the equilibrium.
|
Variables |
Yes |
No |
P-values |
|
Individual patients 6-43 years |
2(13.3%) |
17(37.8%) |
|
|
Individual patients 44-78 years |
13(86.7%) |
28(62.2%) |
P=0.078£ |
Table 10: Relationship between age and brainstorming and losses of subconscious and equilibrium.
- absolute value and percentage in parentheses, £ p-value according to the chi-square test
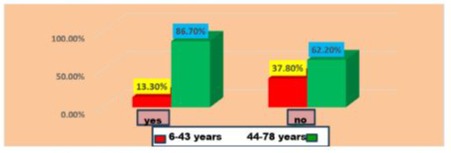
Graph 10: Relationship between age and brainstorming and losses of subconscious and equilibrium.
It is important and clearly expressed according to the data collected from our study and which are shown in the table and graph 11, that pain in the ears of individual patients is manifested and reflected in both genders included in the study, as in that women and men as well.
|
Variables |
Yes |
No |
P-values |
|
Female |
21(58.3%) |
11(45.8%) |
|
|
Male |
15(41.7%) |
13(54.2%) |
P=0.342£ |
Table 11: Relationship between gender and earaches.
- absolute value and percentage in parentheses, £ p-value according to the chi-square test
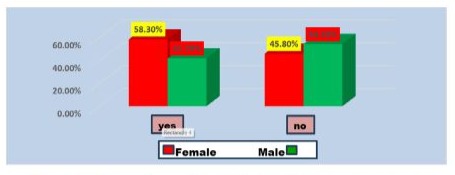
Graph 11: The relationship between gender and earaches.
Referring on the statistical analysis according to the SPSS system (improved version 21) it is clear that there is no statistically significant relationship between age and ear pain since the values of P=0.342, the data of which are reported as above.
Oftentimes, the individual patients of both sexes have also presented the presence of headache symptoms, the data of which are shown in table and graph 12.
|
Variables |
Yes |
No |
P-values |
|
Female |
10(58.8%)* |
22(51.2%) |
|
|
Male |
7(41.2%) |
21(48.8%) |
P=0.592£ |
Table 12: Relationship between gender and headache.
*absolute value and percentage in parentheses, £ p-value according to the chi-square test

Graph 12: The relationship between gender and headache.
From the results of the study, it is noted that there is no statistically significant relationship since the values of P=0.592. We made the differential diagnosis with the group of individual patients with TMJ dysfunction. To check the 211 students, of which 166 (78%) were female, while 45 (21.3%) were male, data presented in table and graph 2 in this study and material as seen on the page 4.
The symptoms of individual patients with TMJ dysfunction are: a] joint pain when the mandible moves; b] difficulty in opening the mouth. (these data are presented in table and graph 2 in this study).
From the data presented in the tables and graphs, it can be seen that the size of the mouth opening in 12 (25.5%) of the individual patients of the studied cases was 20-29 mm, while in 35 (74.5%) of the individual patients the mouth opening was 30-39 mm.
From the results of the study, it is noted that there is a statistically significant relationship since the values of P<0.001.
In these patients, the symptoms of pain around the ear area, TJM dysfunction and Tinnitus were studied. From the results of the study, it is noted that there is no statistically significant relationship between these phenomena since the values of P=0.20.
Discussion
The primary goal of this study case report is to describe managing of the complications and pains that were felt around the ear area, compared the symptoms that are felt around the ear area in cases of ear disease, with those symptoms that are felt in a resting position of TMJ. In the case of TMJ dysfunction, these complications and pains are felt when the lower jaw (the mandible) its moves.
The correlation between hearing symptoms and disorders in the TMJ have not been documented even today by research authors, but it is still a debatable problem [1].
The differential diagnosis of this disease with TMJ dysfunction is made through these symptoms: 1] Absence of pain during jaw movement; 2] Lack of jaw movement limitation. 3] Absence of mouth opening difficulties.
We studied the presence of symptoms of ear pain, headache, tinnitus, fainting, etc. in 60 individual patients who were presented to the Otorhinolaryngology department at UHC in Tirana. From the results of the study, it is noted that 32 (53.3%) were women, while 28 (46.7%) were men.
The predominant symptom of the individual patients with Otorhinolaryngological pathology was earaches like Tinnitus, Dizziness etc., which according to the data of our study was found and determined in 36 (60%) of the patients.
The most important factor that distinguishes pain in the ear from pain in the TMJ, the research authors point out according to references [8-10], is whether it occurs at rest or when the lower jaw, mandible is moving.
We performed the differential diagnosis of ear pathology with a group of 211 individual patients examined with the symptom of pain, from which it was observed that 35 (74.5%) of all cases of individual patients, who had difficulty opening the mouth from the dimensions 30-39 mm.
Among the most important symptoms of TMJ dysfunction, the author Okesan [3] points out in his study, is the difficulty in opening the mouth, and for 37 individual patients these data in our study are presented in graph 2. From these data in the study, it is noted that there is a statistically significant relationship between pain and difficulty opening the mouth, this is explained by the values of P<0.001.
Headache occurs at any age. From the data of our study, according to the table and graph 9, it is observed that the affected ages are between 6-78 years old. From these data of our study and the contemporary literature, it can be observed that there is a statistically significant relationship between headache and the age of patient individuals as the values of P=0.813 [8].
The treatment of patients with ear pain, tinnitus, dizziness was carried out by a specialist doctor in the Department of Otorhinolaryngology at UHC in Tirana. Medicaments such as: glucosamine, chondroitin and hyaluronic acid, are used for their treatment, while the prosthetic treatment includes the use of relaxing, stabilizing-repositioning splints, which the individual patients who underwent this treatment have kept for a period of time from 6-12 months, time which returns to normal the movement of the mandible without the pains and symptoms mentioned above.
Conclusions
At the end of our Study Case Report (scr) based on the collected data, as result of managing the patients with differential diagnosis of Otorhinolaryngological disease, as well as with TemporoMandibular Joint (TMJ) dysfunction was concluded as follows:
1] About of 60 patients treated with ear pathology, 36 (60%) of the cases had severe pain in this area-region.
2] The symptom of pain was also observed in the group of patients with TMJ dysfunction in 35 (74.5%) of the studied cases.
3] The results of the study showed that pain in the ear appears at any age from 6-78 years old, as there is no statistically significant relationship between headache and the age of the individual patient as the values of P=0.813.
4] According to the results of our study, it is noted that there is a statistically significant relationship between pain and difficulties in opening the mouth among patients with dysfunction, since the values of P<0.001.
Financial support & Authors Contribution: This research study case report was funded by the Private Dental Clinic “Qafmolla” in cooperation with “Albanian Eyes Center”, Associated Prof. Ali Tonuzi, Tirana, Albania, where both authors are member and staff partners.
Conflict of interest: In this Study Case Report have not nothing to be declared.
Department and Institution Where Work Was Done: The data collecting referred in our study case report are reported by research register of “QAFMOLLA” Private Dental Clinic managed by Prof. Dr. Ruzhdie Qafmolla, as well in cooperation with “Albanian Center of Eyes”, managed by Associated Prof. Ali Tonuzi, Tirana, Albania.
Declaration of Figures’ Authenticity: All tables and graphs submitted are created and processing by the authors, whom confirm that these data are original with no duplication and have not been previously published in whole or in part in other journals abroad.
Acknowledgement: Both authors of manuscript thank Dr. Luan Qafmolla for obligation and regulation of our manuscript according the guidance of AJCR&R journal, as well as for contacting with editorial board of journal. Also, acknowledgements for Prof. Dr. Ruzhdie Qafmolla and Associated Prof. Ali Tonuzi and his Albanian Eyes Center for the contribution in data base and treatment of patients in respective clinics.
References
- Qafmolla R, et al. (2013) “Gnathology”, Tirana 240-250.
- Lobbezo F, et al. (1997) “Do bruxism and TMJ disorders have a cause and effect relationship”. J Orofac Pain 11: 15.
- Okesan PJ (2003) “Management of TMJ disorders and Occlusion” 108-122.
- Dwarkin FS (2006) “Psychological and psychosocial assessment TMD-s. An Evidence based approach to diagnosis and treatment” 203-217.
- Macaluse GM (1998) “Sleep bruxism is a disorders related to periodontic to periodic are users During sleep”? J Dent Res 65-77.
- Olesen J (2004) “The International Classification of Headache Disorders” edition 2nd, 1: 1-50.
- Meril LR (2006) “Differential diagnosis of ORL pain, TMD-s; an evidence based approach to diagnosis and treatment” 299-317.
- Graff Radford SB (1991) “Headache problems that can present as toothache”. Dent Clin North Am 55: 155-170.
- Greene CS, et al. (1995) “Clinical diagnosis of Orofacial Pain”, Journal Orofacial Pain 9: 7-9.
- Lund JP (2001) “Pain and movement from basic to clinical Management” Chicago Quintessence 151-163.
- Current Diagnosis and Treatment in Otolaryngology Head and Neck Surgery 2008 2nd Edition.
- Temporomandibular Disorders; Priorities for Research and Care 2020.
- Temporomandibular Joint Disorders. Principles and current Practice 2021.
- Anatomy and Pathophysiology of Temporomandibular Joint 2022; 1535-1550
- Bruno Bordoni; Matthew Varacallo; “Anatomy, HEAD and Neck, Temporo-Mandibular Joint” 2021; 23-27.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.