Diagnostic Evaluation of Symptom Qualification using Serial and Parallel Diagnostics
Beijering F.J*. M.D
Meerstraat 48 A, 1941 JC, Beverwijk, The Netherlands.
*Corresponding Author: Frank J. Beijering, Meerstraat 48 A, 1941 JC, Beverwijk, The Netherlands.
Received Date: 14 April 2023
Accepted Date: 24 April 2023
Published Date: : 27 April 2023
Citation: Beijering F.J. (2023) Diagnostic Evaluation of Symptom Qualification using Serial and Parallel Diagnostics. Curr Res Cmpl Alt Med 7: 174. DOI: https://doi.org/10.29011/2577-2201.100074
Abstract
Diagnoses play a pivotal role in medical care. They consolidate information, enable clear communication, and serve as the basis for scientific research. The medical field is vast, with thousands of symptoms indicating various medical conditions. Additionally, the diagnostic process for infectious diseases is relatively clear and based on the identification of a certain set of symptoms. Symptoms with a common cause form a pattern that aids in the diagnosis. Retrospectively, in the medical school environment, replicating the success of treating infectious diseases in situations of metabolic disease cases has been attempted. However, the model for infectious diseases does not match that for metabolic diseases. Thus, we argue that, in addition to a serial- pattern identification approach, using a parallel approach to symptom identification, even after the diagnosis has been made, should be considered. Herein, we distinguish between serial and parallel diagnostic methods, with the aim of enhancing the interface between regular and integrated medicine. The distinction in qualitative symptom evaluation between the different branches of medicine forms the basis of integrated medicine.
Keywords: Analogy; Serial; Parallel; Diagnostics; Cluster; Clinical reasoning
Abbreviations: DESQ- Diagnostic Evaluation Symptom Qualification; IBD- irritable bowel disease; CAS- complex adaptive systems; RCTs- randomized controlled trials
Introduction
In recent centuries, several epidemics have occurred in the Western world, including cholera, typhoid, diphtheria, tuberculosis, poliomyelitis, whooping cough, puerperal fever, acquired immunodeficiency syndrome, and coronavirus disease [1]. Patients with these diseases require professional care with both short- and long-term effects. In modern medicine, the treatment of infectious diseases focuses on combating their causes [2]. However, the scope of treatment also includes the self-healing potential of the patient, which has not been emphasized.
A focus on the use of modern medicine to combat diseases is understandable when public health is at stake. In this context, urgent and effective actions are necessary to treat life-threatening diseases.
In medical science, analytical methods are primarily used to clarify phenomena and identify the underlying cause of illness. In recent decades, cognitive psychology has increasingly been used in the field of medical diagnosis [3,4]. Generally, diseases are classified as either infectious or metabolic. Regarding infectious diseases, the diagnostic process is clear; there is a clear cause, a microorganism, leading to characteristic symptoms. Thus, this diagnostic model involves consistency. Moreover, while the diagnostic process for metabolic diseases is similar to that for infectious diseases, definitive causes must still be determined in practice. In terms of this report, its aim is to distinguish between serial and parallel diagnostic methods, and ultimately enhance the interface between regular and integrated medicine.
Material and Methods
Literature Analysis
The Corpus Hippocraticum describes two schools of thought from ancient Greece: whether the symptoms of diseases should be considered from the point of view of their cause (the concept of rationalism) or whether the perspective of empiricism should be used to view a (naturally) varying pattern of symptoms that can occur in a patient.
A PubMed search using terms such as serial or parallel diagnostics yielded no results. Thus, the terms used and the approach to diagnosis described in this article are not available in the current literature; they will be explained in subsequent sections.
According to Balogh et al. [5], diagnosis has been described as both a process and a classification scheme, or a “pre-existing set of categories agreed upon by the medical profession to designate a specific condition.” According to our understanding, a diagnosis is a collection of symptoms, implying a cyclic process of information gathering and hypothesis formation.
Mamede and Schmidt [6] state that “post-hoc analyses of diagnostic errors have, in fact, suggested that flaws in clinical reasoning, rather than lack of knowledge, underlie cognitive diagnostic errors and were associated with intuitive judgments and could be repaired by analytical reasoning.” They stipulated that when reflection was performed while verifying a diagnosis, diagnostic accuracy substantially increased relative to nonanalytic diagnostic reasoning. In their review, reflection was described as a deliberate consideration of a diagnosis previously generated through intuitive reasoning to examine the grounds that support it [6].
The diagnostic process has been thoroughly explored in cognitive psychology studies [7]. Additionally, study designs have changed over the decades owing to different perspectives, and the diagnostic process is tied to cognitive research [8].
However, previous studies have ignored the diagnostic procedure, including which symptoms are used for the diagnosis and the impact on the resulting decision.
Moreover, Croskerry [3] defined “metacognition” as an approach of stepping back from an immediate problem to examine and reflect on the deliberation process. This moment of deliberate consideration was also described by Mamede et al. [9].
We observed substantial differences in the evaluation of different types of therapies. Some diseases have a short course, while others persist for a long period or even for life. In this research, we explored whether the type of diagnosis influences the therapy provided.
Proposing DESQ, Diagnostic Evaluation Symptom
Qualification
Specific symptoms should be selected for diagnosis. Thus, a system termed Diagnostic Evaluation Symptom Qualification (DESQ) would be useful and can serve as an inventory before decision-making. Kim et al. also corroborated this idea [10], stating that symptoms should be broadened to include both subjective (self-reported) and objective (observed) features. The value of individual symptoms has become increasingly important. In the DESQ, all symptoms are recorded according to their cause (e.g., cardiac failure, edema, and cyanosis). Additionally, using another paradigm, symptoms are rubricated in parallel (non- causal) positions, and those not sharing a cause should be recorded separately (e.g., pain in the left eye, eczema, and arthritis).
To clarify or explain processes in disease phenomena, the method of thinking must be coherent with the etiology of the disease in question. This indicates that medical scientists should have a particular interest in the fact that the disease process and etiology are inherently logical. However, when the disease develops atypically and not according to logical pathways (e.g., sweating as a symptom of Parkinson’s disease and migraine as a symptom of Crohn’s disease), discrepancies between the disease as a problem and the potential for problem solving, which should be expected from logical methods of thinking, are reasons for substantial confusion [1]. This insight partly explains the problem at the core of chronic disease. If the disease does not develop according to a typical pathway, a logical approach is not always the best solution.
In the following sections, we discuss clinical reasoning, serial and parallel diagnostic methods, that is, the analogy between infectious and internal diseases, and diagnosis from the point of view of phenomenology.
Clinical Reasoning
The success of infectious disease treatment through the extensive use of antibiotics has proven to be of great importance in medical reasoning overall, and particularly in diagnosis [11]. This success led clinicians to follow the same diagnostic pattern for metabolic diseases, that is, a group of symptoms was considered to have one common cause. A lack of symptoms can lead to doubts about the diagnosis because it is assumed that the symptoms are directly and serially causal. This serial pattern can be visualized as a chain of connected lights on a Christmas tree. Failure of one “bulb” interrupts the “current” through the chain and affects the diagnosis. Another metaphor is a tent in which sticks hold up the roof. One can receive shelter regarding the isolation of the concerning symptoms (shelter in the tent; symbol in Figure 1).


Figure 1: The tent symbolizes a serial composition of symptoms above a barcode representing a parallel collection of symptoms.
Pathognomonic symptoms (e.g., the characteristic rash of measles or rubella) play an important role in symptom evaluation. Laboratory test results are similarly interpreted (e.g., collagenase 1 levels in rheumatoid arthritis) [12]. When interpreting laboratory data, one or more internal variables are used as indicators of the underlying cause of the external symptoms. An abnormal biochemical value is assumed to be representative of the disease or symptom [13]. For instance, type 2 diabetes mellitus is diagnosed using a single parameter; the glucose level is accompanied by a loss of information regarding the rest of the patient. Recently, Parkinson’s disease has been diagnosed based on changes in the patient’s voice dialogue.
The serial image above is a metaphor in which a tent is supported by sticks, which function to support the “diagnosis” (Figure 1).
The tent erected on the foundation of the barcode illustrates a “holy entrance” approaching the top as the ultimate cause. The tent collapses if one stick is missing.
The barcode represents the independence of individual symptoms. This parallel arrangement of individual symptoms in the DESQ facilitates Bayes probability calculations for Prognostic Factor Research [14].
In the last two decades, systems biology has been recognized as the foundation for integrated medicine. Personalized medicine is of central importance in systems biology.
Van der Greef et al. [15] provided an example to illustrate how the diagnostic process follows different routes, depending on the clinician’s worldview. They compared Western and Chinese medicine approaches for rheumatoid arthritis. In Chinese medicine, a diagnosis is made based on factors termed as “cold” and “heat,” which are related to the patient’s genetic makeup. The differences in subtypes distinguished through Chinese medical approaches can be explained using Western chemical concepts through molecular differences.
A heuristic method using the DESQ is also applicable. We consider a diagnosis in Chinese medicine based on “heat” and “cold” to be a parallel diagnostic method, where the symptoms are considered independent. Therefore, the use of both serial and parallel diagnostic systems allows clinicians to adapt the diagnostic process according to the situation.
Therapeutic Consequences
The diagnosis determines the choice of medication. It also represents an overlap between empirical and rationalistic processes. The result of rationalistic (analogical) thinking is that among the symptoms presented during internal (non-infectious) illnesses, clinicians search for a serial pattern in these symptoms of patients with metabolic diseases of unknown causes.
The actual cause of an infectious disease is addressed with antagonistic treatment, whereas for metabolic diseases, only the suspected cause is addressed. Therefore, in internal diseases, treatment only modulates (pharmacologically) the so-called cause. Hence, treatment must be continued. As the cause is not eliminated, metabolic diseases become more chronic. When the infectious disease model does not agree with the underlying (non- linear) disorder, serious dissonance may result.
To meet the scientific requirements of repeatability and consistent outcome, the treatment drug must be repeated.
Unfortunately, the above is a negative side of the need for scientific verification using the hypothetical-deductive method.
A low hemoglobin level (internal variable) is considered to be the cause of anemia, although the underlying factors that lead to this abnormal value are often not sought and found [16]. However, such a system is not pragmatic. Similarly, in the case of hypothyroidism, a low thyroxine level is often regarded as the cause instead of a biochemical factor. Although the thyroid gland has many biochemical connections with other endocrine organs, which in turn are part of a network of complex feedback mechanisms, these are not always sought, and diseases such as Graves’ disease are only treated with hormone supplementation [24]. Irritable bowel disease (IBD) is considered a chronic condition because its actual cause is unknown. In these examples of serial diagnostic reasoning, it can be seen that iron supplementation often has short-lived benefits, anemia recurs frequently, and thyroid hormone supplementation is sometimes required for life. Lastly, Horniblow et al. [17] elucidated the unwanted epigenetic role of iron supplementation in IBD (see Discussion).
Analogy Within the Commonly Used Diagnostic Method
The serial diagnostic method is characterized by the fact that the absence of symptoms leads to uncertainty in the diagnosis. The intrinsic relationship among symptoms (linked owing to their association with a presumed cause) can be seen as a serial pattern. In serial diagnostics, the collection of symptoms that serve for rational (causal) understanding should be built up to a diagnosis, and a problem arises in the absence of (pathognomonic) symptoms.
An infectious disease comprises a group of symptoms with identifiable microbes as a common cause. The symptoms show a recognizable pattern [18].
Examples:
Infectious condition: The chain of the routine symptom pattern is as follows:
Diphtheria: Tonsillitis - Exudate tongue - Foetor ex ore - Swollen lymph nodes
Meningitis: Neck stiffness - Nausea - Vomiting - Hypersensitivity and sound
Coronavirus: Fever - Dry cough - Sore throat - Vomiting - Neuropathy - Petechiae
Internal condition: The chain of the symptom pattern routinely encountered is
Hypothyroidism: Constipation - Dry skin - Bradycardia - Low Triiodothyronine (T3) - Loss of hair - Weight gain
M. Parkinson: Tremor, Bradykinesia - Constipation - Micrographia - Insomnia - Apathy
Metabolic Syndrome: Obesity - Hypertension - Dyslipidemia - Insulin resistance
Infectious diseases show how symptoms are intrinsically related, regardless of the circumstances. If any of the symptoms are missing, diagnosis is less likely.
Similarly, in internal diseases, diagnosis is based on a set of symptoms, where the absence of a single symptom invalidates the diagnosis.
We believe that the routinely used diagnostic method has characteristics analogous to those of the model for infectious disease diagnosis. According to Holyoak and Koh [19], the infectious chain has diverse features that are causally relevant to goal attainment and considered structural (vs. surface) similarities. Finding a cause provides a structure to syntactic elements [20].
Before ascertaining the cause, the approach for infectious disease treatment was phenomenological. A pattern was identified only after repeatedly gathering information on symptoms, which allowed for serial processing.
Determining the pattern of infectious disease as the source and the pattern of the typically used diagnostic process as the target, revealed that both processes have unique features with a structural similarity, which is responsive to retrieval in the mapping process of the two chains. Thus, both elements of the infectious (source) and internal (target) chains serve as retrieval cues in a content-addressable memory system, which represents a structural similarity that is stored during the mapping (structural comparison) process and provokes an analogy during the diagnostic approach. We infer that under semantic-related constraints [21], the diagnostic method for internal diseases needs a cause similar to that of infectious diseases.
According to Gentner [22], analogies should appeal to different domains. Gentner used the example of an electric battery and reservoir or solar system and molecular structure to illustrate the different domains.
Clinically, both approaches involve a collection of symptoms. Herein, the analogy is not about the domain but about the method.
Parallel Diagnostics
It is important to reflect on parallel thinking. In the context of reduction of diagnostic error, one can think of metacognition [8], which is a reflective approach to problem solving that involves stepping back from the immediate problem to examine and reflect on the thinking process (phase 2 in dual-process thinking) [3,23].
With a parallel diagnostic pattern, there is no fixed relationship between the effect and cause. Multiple problems or symptoms can coexist, such as those in parallel circuits. Similarly, failure of one light bulb does not affect the other light bulbs, and a tent can have enough sticks to remain standing. Contributing to a diagnosis, multiple organs and systems can be involved simultaneously, although the symptoms may develop consecutively over time.
As a rule of thumb, serial diagnostics uses the “if not this, then neither that” approach, while parallel diagnostics follows the “you can go along here but also along there” approach. Thus, we can explain why the typically used serial diagnostic approach is monistically rather unapproachable, and integrative medicine with the parallel approach is more feasible for communication.
For instance, in homeopathy, sulfur can be used to treat various symptoms, including hair loss, calluses on the feet, and dark nevi. Symptoms like leucorrhea, arthritis, and coldness, which are also treated with sulfur, can manifest in various conditions. These symptoms have no common cause except that they can be interconnected. This explains their parallel state.
In Chinese medicine, patterns are distinguished by the influence of Yin and Yang, which in Western terms correspond to ortho-sympathetic and para-sympathetic. The meridian point, Ni-3, can be used for menstrual pain, neurasthenia, cystitis, and pharyngitis. Spleen 6 can be used to treat dysmenorrhea, diarrhea, and neurasthenia [24]. For diagnosis, the “Ba Gang” uses the variables heat-cold, deficiency-excess, inside-outside, and Yin- Yang, depending on the patient’s composition.
In the traditional Chinese medicine diagnostic system “Bianzheng Lunzi,” Crohn’s disease is associated with damp and hot intestines. To treat diarrhea, stomach meridians 21 and 25 can be used, and to treat blood stasis, points to move blood, including spleen 6 and 10 and liver 3 [25], can be used. This approach is based on the five-element theory, which provides many independent points of entrance for treatment that are parallel and not connected to one another. They are not serial because each pattern has a different combination of points based on the polarity principle. Parallel thinking accommodates the acupunctural approach, in which the excess or deficiency of Yin and Yang operates as a determining symptom.
Differences between serial and parallel diagnostics can also be observed in patients with Parkinson’s disease. Within the symptom cluster observed in this condition, a pattern similar to that of infectious diseases is recognizable.
Parkinson’s disease is characterized by the following serial symptoms: tremor, bradykinesia, constipation, and micrographia. Additionally, the following parallel symptoms are observed: sweating, stomach pain, pruritic eczema, and phlebitis. These symptoms cannot be deduced from neurological conditions and originate from alterations in metabolic pathways that lead to various neurological, gastrointestinal, and immunological disorders [26]. Balancing dopamine levels in patients with Parkinson’s disease seems insufficient to restore health. Additional symptoms like sweating, stomach pain, pruritic eczema, and phlebitis may be caused by disruption of an underlying common bioregulatory system, as described in a previous report [27]. Such a system connects widely separated organs. It is plausible that the parallel symptoms indicate the ultimate neurological condition (toxin metastasis via leukotrienes).
A holistic view encompassing all symptoms pays particular attention to parallelism.
Consideration and Ontology of Parallel versus Serial versus Course Methods
Although serial-parallel ideology is still a new concept, parallelism has already been studied. A recent study [28] involved the term “symptom clusters” and the development of a questionnaire that helped determine the treatment for premenstrual syndrome based on the symptoms observed. The identification of individual symptoms that are not considered causally related demonstrates parallelism.
In the context of symptom clusters, we must refocus on literature. Plsek and Greenhalgh [1] were dissatisfied with their inability to account for surprise, creativity, and emergent phenomena. They reported on a new science of complex adaptive systems (CAS) and shared their specific understanding of CAS. Signaling the complexity of health care, they abandoned the machine metaphor, proposing that CAS has “fuzzy edges” that allow for nonlinearity with internalized rule sets. Miaskowski et al. [29], who favor pioneering symptom clusters, call the new frontier in symptom management research a cutting-edge science. Symptom cluster management research should be conducted in tandem with research on single symptoms.
Miaskowski et al. [30] described a group of symptoms in patients receiving chemotherapy (e.g., pain, fatigue, and sleep disturbance) as a symptom cluster, where treating a single symptom might have crossover effects that reduce the severity of other symptoms in the cluster. These clusters occur in a variety of chronic conditions such as human immunodeficiency virus infection, co-occurring disorders, heart diseases, and renal failure. Dorsey et al. [31] announced the genesis and development of a consortium-studying symptom science in a precise era using common data elements. Breazeale et al. [32], in their study of traumatic orthopedic injuries, stipulated that membership in symptom cluster profiles shows what future research could look like.
According to Zhu et al. [33], there is a concept of symptom science in oncology nursing in which symptom clusters are closely observed. For instance, loss of appetite, changes in taste, nausea, and vomiting appear shortly after the initiation of chemotherapy. Moreover, they concluded that “overall, symptom clusters and symptom networks are two crucial paradigms in symptom science.”
These ideas remain debatable (showing considerable interest in symptoms). Thus, it appears that DESQ has already been implemented, as it is a common practice. Zhu et al. also defined symptom networks as causal networks of mutually enforcing symptoms using a network analysis.
With regard to the serial-parallel concept, it is not forbidden to use the causal principle when entering the parallel domain. Symptoms can be interrelated or investigated in relation to their causes.
It is important to note that diverse research aims to improve health and diagnosis. The serial-parallel theory respects the fuzzy edges, and its main goal is to ensure that this concept is applicable for the differential diagnosis of both infectious and metabolic diseases and can be used to prevent diseases from progressing to chronic states. The serial-parallel theory provides room for understanding that, in addition to serial diagnostic methods, other approaches can and should contribute.
The selective symptom collection (DESQ) characteristic of parallel diagnostics also underpins Bayes’ calculation of the likelihood ratio of separate symptoms. This contributes to research on prognostic factors. The Bayes method focuses on evidence-based medicine and the uncertainty associated with the pieces of evidence. The proposed models are primarily used for the diagnosis of different diseases with partial evidence [34]. The parallel diagnostic method involving mutually independent symptoms appears to be utilitarian. Notably, the term “parallel” does not mean “next to serial.” The term is based on the application and evaluation of symptoms that are not intrinsically related to one another and have no limiting common cause. The fact that it co-exists with serial diagnostic methods is useful in the overall medical field.
Nevertheless, it should be mentioned that a serial-oriented diagnosis can be advantageous for chronic diseases, just as the parallel-oriented method can be advantageous for acute conditions on an empirical basis.
Phenomenology
Observing morphological evidence of serial and parallel structures from a phenomenological paradigm, we rediscovered the serial-parallel model in terms of analogy in form, function, and anatomy. The use of anatomical terms is strongly linked to clinical reasoning [35]. Studies have illustrated the relevance of anatomy in medical education and reveal that teaching essential anatomy is significantly undervalued [36,37].
The form and function unit in biology is a useful reference to illustrate the natural appearance of the venous system and the anatomical context of serial and parallel functional structures [38].
Likewise, the natural appearance of the venous system is a useful reference for form and function units, depicting the anatomical context of serial and parallel functional structures as well.
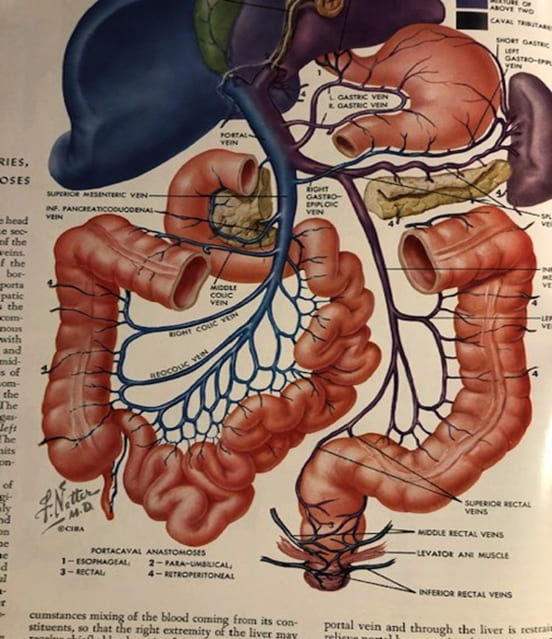
Figure 2: Venous drainage of the intestines.
Figure 2 shows the venous drainage of blood from the intestines. This detailed illustration also reveals the venous anastomotic network of the intestines. In the mesentery, morphological evidence is seen of serial and parallel structures, which gradually merge where no actual separation can be seen. Additionally, evolution results in morphological exaptation, a well- established biological phenomenon that is a product of intentionally guided variation [38]. Notably, a change in structure must be accompanied by a change in function; the veins show a unity of form and function. When the largest surface along the intestine is drained, parallelism prevails through multiple collaterals. In terms
of the flow ratio (from much to small, great to little; reductionism), the transition gradually occurs from the parallel intake of smaller vessels to conical areas with a larger diameter but serial in form and structure. Vice versa, the arterial flow comes from serial tubes dispearsing themselves to a (anastomotic) parallel network to provide optimal infusion. We can see a similar temporal course in the diagnostic proces, a coming and going from serial to parallel.
The serial-parallel pattern implicates a naturally occurring anatomical functional structure. This indicates that serial-parallel patterns alternate with functional adaptation. It concerns the analogy between form and (abstract) function within the serial- parallel concept. Thus, the serial-parallel model has a functional anatomical basis. With metacognitive comprehension, serial- parallel anatomy can be extrapolated to the level of diagnosis.
With this phenomenological view, we acknowledge that the passage from serial to parallel has a transient deconstructive character, but thereafter, there is adequate reconstruction of the total symptoms.
Results
The infectious disease model and the analogous use of this model for metabolic diseases do not agree with the more appropriate model for evaluating underlying regulatory disorders that result in parallel symptoms. Thus, chronicity results, in part, from the medication administered for treatment. Furthermore, serial diagnostic methods consider each disease as a separate entity. In parallel diagnostic methods, various symptoms are considered to exist simultaneously. This is the focus of a holistic view; serial and parallel symptoms go hand in hand.
Referring to Norris and Cutler [39], we aimed to answer the questions “More why, less how: What we need from models of cognition” and “What would be the use of the serial-parallel concept?” This concept is necessary to understand that the current medical scenario, in which multimorbidity is common, has complex problems [40]. With population aging, the time that people live with disabilities and chronic diseases is increasing, and almost three-quarters of adults in developed countries have multiple chronic conditions [41]. It has been shown that 60% of the US population reportedly has at least one chronic disease, whereas 42% have multiple conditions [42].
An overview of parallelism can be useful for metacognition [3], where following the strict causal principle implicates our genetic constitution as the ultimate etiology of the disease and the target of treatment.
Since metabolic diseases are treated chronically in the same way as mono-causal infectious diseases, as the analogy shows, in addition to the serial pattern, it is justified to recognize a parallel pattern of symptoms that do not find a place in the serial diagnostic process.
The multitude of parallel symptoms that remain after a serial diagnostic result is obtained explain why randomized controlled trials (RCTs) are difficult to use as the sole gold standard of evidence for chronic conditions [43,44]. RCTs use a serial diagnostic method to search for one cause only, and parallel (individual) symptoms are not considered. Bias is at play in the phase of symptom collection, as well as during pharmacological elaboration. Thus, RCTs cannot evaluate all symptoms, resulting in obscuration of vital information. The mere application of serial diagnostic methods explains the many side effects of the regular approach in the treatment of chronic diseases. For example, medically unexplained symptoms have parallel symptom patterns that far exceed the scope of the serial diagnostic method.
Discussion
A discussion about the serial-parallel concept must credit epigenetics, serving as an interface between the environment and genome. Metabolic diseases not only develop due to inborn errors, but are also acquired metabolically, specifically from lifestyle- related habits, including diet, obesity, tobacco smoking, alcohol consumption, environmental pollutant exposure, psychological stress, and night-shift work. Furthermore, the chronic use of medication as a basic lifestyle for millions of people has rarely been considered, and the impact of drugs on epigenetic control has been underestimated. However, a change has been observed. Csoka and Szyf [44] described various drugs with known or postulated epigenetic effects. For example, ß-blockers are associated with, among other effects, alterations in lipid and glucose metabolism, and statins cause extensive gene expression alterations in target organs. Horniblow et al. [17] reported that an excess of unabsorbed iron in the colon of patients receiving iron to treat anemia is related to IBD. Iron mediates epigenetic activation and alters gene expression with significant hypomethylation of the epigenome.
Whether the working mechanism is magneto-dynamic (homeopathy), electrophysical (acupuncture), or chemico-physical (Western medicine), diagnosis must accommodate the method of symptom collection. It is unlikely that an alternative method can be evaluated based on the hypothetical-deductive method of regular diagnosis. Furthermore, methodological choices and vested interests can undermine the credibility of individual RCTs [43,44]. In the parallel pattern, the cause is unknown; however, the symptoms can be significant and interrelated. They form an individualized pattern that fits the vision of integrated medicine, which is based on an individual complaint pattern and approach (personalized medicine). The meaning of personalized medicine seems ambiguous; it has been used to refer to holistic medicine as well as therapy (i.e., in oncology) based on gene alleles.
Conclusions
One aim of this report was to demonstrate that using diagnostic approaches other than the typically Hypothetical- dedutive used method can be advantageous; the serial model has limitations that can lead to chronicity. The parallel approach opens new possibillities, a way out of the causal constrain.
The iatrogenic and epigenetic side effects of medications should always be considered [45]. Moreover, it is unrealistic to require studies on the effects of alternative medical approaches to be designed in the same manner as those on approaches using a serial method when there is significant chronicity. Should we think of Socrates saying, “No one errs willingly”? [46].
The DESQ, the distinction in qualitative symptom use among different treatment methods, forms the basis of integrated medicine. It is also clear that synthetic a priori serial diagnostics are preferred for acute diseases (hidden in the tent); however, synthetic a posteriori parallel diagnostics (bare view) are more suitable for chronic conditions. Serial and parallel functions are inherent in the biological and pathological functioning of humans and should therefore be reflected in the diagnostic procedure. As a concept, the serial-parallel diagnostic model finds itself in the context of discovery. To make progress in terms of justifying this claim, we need the proper scientific application of the discussed models.
Acknowledgement
The author is grateful to Francois Weber for enthusiastic support.
References
- Plsek PE, Greenhalgh T (2001) Complexity science: the challenge of complexity in health BMJ 323:625-628.
- Coulter HL (2001) Divided legacy: a history of the schism in medical Vol. 2. Berkeley: North Atlantic Books.
- Croskerry P (2003) Cognitive forcing strategies in clinical decisionmaking. Ann Emerg Med 41:110-120.
- Gilhooly KJ (1990) Cognitive psychology and medical diagnosis. Appl Cognit Psychol 4:261-272.
- Balogh EP, Miller BT, Ball JR (2015) Improving diagnosis in health Washington, DC: National Academies Press.
- Mamede S, Schmidt HG (2017) Reflection in medical diagnosis: a literature review. Health Prof Educ 3:15-25.
- Schmidt HG, Mamede S (2020) How cognitive psychology changed the face of medical education research. Adv Health Sci Educ Theory Pract 25:1025-1043.
- Norman GR, Monteiro SD, Sherbino J, Ilgen JS, Schmidt HG, et al., (2017) The causes of errors in clinical reasoning: cognitive biases, knowledge deficits, and dual process Acad Med 92:23-30.
- Mamede S, Schmidt HG, Rikers RM, Penaforte JC, Coelho‐Filho JM (2007) Breaking down automaticity: case ambiguity and the shift to reflective approaches in clinical Med Educ 41:1185-1192.
- Kim HJ, McGuire DB, Tulman L, Barsevick AM (2005) Symptom clusters: concept analysis and clinical implications for cancer nursing. Cancer Nurs 28:270-282.
- Cook MA, Wright GD (2022) The past, present, and future of Sci Transl Med 14:eabo7793.
- Petrow PK, Hummel KM, Schedel J, Franz JK, Klein CL, et , (2001) Expression of osteopontin messenger RNA and protein in rheumatoid arthritis: effects of osteopontin on the release of collagenase 1 from articular chondrocytes and synovial fibroblasts. Arthritis Rheum 43:1597-1605.
- Vasan RS (2006) Biomarkers of cardiovascular disease: molecular basis and practical Circulation 113:2335-2362.
- van der Greef J, van Wietmarschen H, Schroën J, Wang M, Hankemeier T, et , (2010) Systems biology-based diagnostic principles as pillars of the bridge between Chinese and Western medicine. Planta Med 76:2036-2047.
- Rutten L, Miglani A, Gold P, Manchanda RK, Chakraborty M, et al., (2022) Generalizability of homeopathic prognostic factor research outcome in COVID-19 treatment: comparison of data. Homeopathy 111:157-163.
- Midgley JEM, Toft AD, Larisch R, Dietrich JW, Hoermann R (2019) Time for a reassessment of the treatment of hypothyroidism. BMC Endocr Disord 19:37.
- Horniblow RD, Pathak P, Balacco DL, Acharjee A, Lles E, et , (2022) Iron-mediated epigenetic activation of NRF2 targets. J Nutr Biochem 101:108929.
- Baron S (1996) Medical 4th ed. Galveston, TX: University of Texas Medical Branch at Galveston.
- Holyoak KJ, Koh K (1987) Surface and structural similarity in analogical Mem Cognit 15:332-340.
- Lee HS, Holyoak KJ (2008) The role of causal models in analogical J Exp Psychol Learn Mem Cogn 34:1111-1122.
- Oden GC (1978) Semantic constraints and judged preference for interpretations of ambiguous Mem Cogn 6:26-37.
- Gentner D (1983) Structure-mapping: a theoretical framework for Cogn Sci 7:155-170.
- Berry DC (1983) Metacognitive experience and transfer of logical Q J Exp Psychol 35:39-49.
- Konig G, Wancura I, Hawlik F (1981) Neue chinesische Akupunktur: Lehrbuch und Atlas mit naturwissenschaftlichen Wilhelm Maudrich.
- Ross Zang fu. London: Churchill Livingstone; 1985.
- Nagamani S, Sahoo R, Muneeswaran G, Sastry GN (2019) Data science driven drug repurposing for metabolic In: Roy K, editor. In silico drug design: repurposing techniques and methodologies. Cambridge, MA: Academic Press 191-227.
- van Wijk R (2004) Basic bioregulation system in search of a new bio- energetic concept of health TIG volume 21 | 22 I Part 3.
- Klein-Laansma CT, Jong M, von Hagens C, Jansen JPCH, van Wietmarschen H, et al., (2018) Semi-individualized homeopathy add- on versus usual care only for premenstrual disorders: a randomized, controlled feasibility J Altern Complement Med 24:684-693.
- Miaskowski C, Dodd M, Lee K (2004) Symptom clusters: the new frontier in symptom management J Natl Cancer Inst Monogr 17-21.
- Miaskowski C, Barsevick A, Berger A, Casagrande R, Grady PA, et , (2017) Advancing symptom science through symptom cluster research: expert panel proceedings and recommendations. J Natl Cancer Inst 109.
- Dorsey SG, Griffioen MA, Renn CL, Cashion AK, Colloca L, et al., (2019) Working together to advance symptom science in the precision Nurs Res 68:86-90.
- Breazeale S, Dorsey SG, Kearney J, Conley S, Jeon S, et al., (2021) Symptom cluster profiles following traumatic orthopedic injuries: a Res Nurs Health 44:268-278.
- Zhu Z, Xing W, Hu Y, Wu B, So WKW (2022) Paradigm shift: moving from symptom clusters to symptom networks. Asia Pac J Oncol Nurs 9:5-6.
- Dehghani M (2009) A cognitive model of recognition-based moral decision making ([doctoral dissertation]. Northwestern University).
- Boerwinkel DJ, Waarlo AJ, Boersma K (2010) A designer’s view: the perspective of form and function: educational research. J Biol Educ 44:12-18.
- Sbayeh A, Qaedi Choo MA, Quane KA, Finucane P, McGrath D, et , (2016) Relevance of anatomy to medical education and clinical practice: perspectives of medical students, clinicians, and educators. Perspect Med Educ 5:338-346.
- Vorstenbosch MA, Kooloos JG, Bolhuis SM, Laan RF (2016) An investigation of anatomical competence in junior medical Anat Sci Educ 9:8-17.
- Larson G, Stephens PA, Tehrani JJ, Layton RH (2013) Exapting Trends Ecol Evol 28:497-498.
- Norris D, Cutler A (2021) More why, less how: what we need from models of Cognition 213:104688.
- Mangin D, Heath I, Jamoulle M (2012) Beyond diagnosis: rising to the multimorbidity BMJ 344:e3526.
- Hajat C, Stein E (2018) The global burden of multiple chronic conditions: a narrative Prev Med Rep 12:284-293.
- Hayes TON, Gillian S (2020) Chronic disease in the United States: A worsening health and economic crisis. American Action Forum 1-12.
- Aakster CW (2009) Shifting views on the Golden Standard [yearbook].
- Krauss A (2021) Assessing the overall validity of randomised controlled International Studies in the Philosophy of Science 34:159-182.
- Csoka AB, Szyf M (2009) Epigenetic side-effects of common pharmaceuticals: a potential new field in medicine and Med Hypotheses 73:770-780.
- Penner T (2018) Inequality, intention, and ignorance: Socrates on punishment and the human Democracy, justice, and equality in ancient Greece: historical and philosophical perspectives. Berlin, Heidelberg, Germany: Springer Verlag 83-138.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.