“Cut As You Go” Technique Versus T-Technique for Impacted Mandibular Molars with Piezo Surgery: A Comparative Study”
by Renato Isufi*, Aurora Isufi, Ramazan Isufi, Tanita Daci, Belisa Kalefi
Depratment of Oral and Maxillofacial Surgery, Isufi Royal Dental, Tirana, Albania
*Corresponding author: Renato Isufi, Depratment of Oral and Maxillofacial Surgery, Isufi Royal Dental, Tirana, Albania
Received Date: 28 July 2025
Accepted Date: 04 August 2025
Published Date: 06 August 2025
Citation: Isufi R, Isufi A, Isufi R, Daci T, Kalefi B (2025) “Cut As You Go” Technique Versus T-Technique for Impacted Mandibular Molars With Piezo Surgery: A Comparative Study J Surg 10: 11402 https://doi.org/10.29011/2579760.011402
Abstract
The study explores the effectiveness of two different tooth extraction techniques for impacted mandibular third molars: the “Cut as you go” technique and the traditional T-shape technique. The primary hypothesis investigated is whether the “Cut as you go” technique reduces operative time and postoperative pain compared to the T-shape method. The study included 32 patients aged between 16 to 63, who underwent tooth extractions at University Dental Clinic and Isufi Royal Dental Clinic in Tirana Albania. The study revealed that the operative time was indeed shorter for the “Cut as you go” technique, averaging 20 minutes per operation compared to 25 minutes for the traditional method. Additionally, postoperative pain, measured by the Visual Analog Scale (VAS), was generally lower in the experimental group, suggesting the “Cut as you go” technique may improve patient comfort and satisfaction. The study also highlights gender differences in pain perception, though these differences were not statistically significant. Statistical analyses showed a strong positive correlation between operative time and VAS scores, with a more pronounced linear relationship in the experimental group. Overall, the “Cut as you go” technique not only proved to be faster, but also seemed to offer greater patient satisfaction and potentially fewer complications compared to traditional methods.
Keywords: Cut as you Go Technique; Dental Surgery; Impacted Third Molar; T Technique
Background
Methods for tooth extraction have been used since prehistoric times as part of rudimentary folk medicine practices. The first documented extractions are attributed to Hippocrates, who referred to dental interventions in his writings on pathology and medical treatment. This tradition was later continued by Aristotle, who even developed specialized forceps, which he described in his work “Mechanics”[1]. It was Walter Harris who proposed the use of incision for difficult tooth extractions in his pamphlet on oral infections [2]. And in the same period, the Dutch physician Kornelis van Soolingen stated that dental extractions are procedures that should be performed by physicians and not by barbers or charlatans [3]. Precise techniques for the extraction of third molars began to develop at the end of the 18th century, and in 1903, the National Dental Association published, for the first time, a manual on the removal of third molars. In 1918, an American dentist named Kells published an article describing the method for extracting third molars.[4]. In 1926, George B. Winter, a professor at the School of Dentistry at the University of Washington, published “The Principles of Extraction of Impacted Mandibular Third Molars,” which became the contemporary manual of its time [5]. Meanwhile, the oral surgeon Kurt H. Thoma from Switzerland proposed the term “odontotomy” for the surgical removal of a tooth [6]. In 1933, it was the surgeon William Fry who first described the technique of bone splitting using a chisel, which consisted of placing a chisel on the distal aspect of the molar, parallel to the external oblique ridge [7]. Harold C. Klipatrick was the first to compare the use of a chisel, a slow-speed bur (40,000 rpm), and a high-speed bur (200,000 rpm). His study concluded that the high-speed bur resulted in a better postoperative healing period [8]. In 1960, Guillermo Ries-Centeno published “El Tercer Molar Inferior Retenido”, in which he described all the surgical approaches for the removal of impacted mandibular third molars [9] n 1971, Lucian Szmyd described various techniques for sectioning mandibular third molars to facilitate their extraction [10]. The extraction of mandibular third molars is a more complex surgery compared to other molars due to their position, bony obstruction, tooth angulation, and the limited surgical field [11]. The extraction procedure begins with the elevation of the mucoperiosteal flap, removal of the bone surrounding the crown of the tooth, sectioning of the tooth, extraction of the tooth, and postoperative management. Typically, following this procedure, patients experience pain, edema, trismus, and bleeding, which can affect their quality of life [11]. To avoid complications and to facilitate the patient, many improvements have been made for the removal of impacted third molars such as flap modifications, different methods of tooth sectioning, and various suturing techniques. Tooth sectioning is a very important step in the removal of horizontally impacted third molars. Proper tooth sectioning reduces the need for excessive bone removal, the duration of surgery, and postoperative complications.
Objective
The aim of this study is to compare the operative time and postoperative pain during and after the removal of impacted third molars in the mandible using T tooth sectioning technique and the “Cut as you go” technique.The hypothesis of the researchers is that the “Cut as you go” sectioning method will shorten the operative time and reduce postoperative pain compared to the existing tooth sectioning methods especially T Shape. The specific aims of this study are to compare the operative time, the measurement of postoperative pain using the Visual Analog Scale (VAS), quality of life using the PoSSe scale.
Materials and Methods
This study included patients aged 16-63 years with impacted mandibular third molars to be extracted at the University Dental Clinic and Isufi Royal Dental Clinic during the period 2024-2025. The average age of the sample was 28 years and the standard deviation 11.8.The average duration of the intervention in minutes was 20 minutes for the experimental group and 25 minutes for the control group. From the study, 32 patients met the inclusion criteria. All patients were operated on by the same surgeon.
Inclusion Criteria in the Study
- Horizontally impacted teeth
- Mesioangular impacted teeth
- Good general health condition
- Normal mouth opening
Patients Were Excluded from the Study If
- They had local or general contraindications for tooth extraction,
- The roots of the teeth were not fully formed,
- Pericoronitis.
Variables in the Study: Operative time was measured from the beginning of the incision until the suturing. Postoperative pain was measured with the VAS scale from 0-10. Patient satisfaction was measured on the 3rd and 7th day after the intervention by marking a straight vertical linen a VAS scale. The variables included age, gender, and the tooth according to Winter’s classification. Patients were divided into two groups: the experimental group and the control group. In the experimental group, the “Cut as you go” tooth sectioning technique was used (n = 17 patients), while in the control group (n =15 patients), other tooth sectioning techniques were used. All patients were informed about the study and signed the consent form.
The data were subjected to statistical analysis using the SPSS software, version 29. The average age in the experimental group was 24 years, with a lower age limit of 16 years and an upper limit of 33 years, compared to the average age in the control group which was 34 years with a lower limit of 21 years and upper limit of 63 years. The age structure in the experimental group is more homogeneous, which implies more consistent results in this group. A more heterogeneous age structure implies other health problems that indirectly affect the VAS-score values. Precisely to avoid the effect of confounding variables such as age or gender, the data were standardized for the variable age and gender, and statistical techniques such as Pearson correlation coefficients and Linear Regression were used. Below, the effect of gender on VASscore values is examined for both groups through cross-tabulations (Table 1).
|
Experimental group versus
control group |
Total |
||||
|
Male |
Female |
||||
|
Experimental Group |
Visual Analog0020Scale |
0 |
0 |
3 |
3 |
|
1 |
2 |
5 |
7 |
||
|
2 |
0 |
4 |
4 |
||
|
3 |
1 |
2 |
3 |
||
|
Total |
3 |
14 |
17 |
||
|
Control Group |
Visual Analog Scale |
0 |
0 |
2 |
2 |
|
1 |
3 |
2 |
5 |
||
|
2 |
2 |
4 |
6 |
||
|
3 |
1 |
0 |
1 |
||
|
4 |
1 |
0 |
1 |
||
|
Total |
7 |
8 |
15 |
||
Table 1: VAS-score* by gender (Cross-tabulations).
In the control group, the majority of female patients (n=4) reported an operative pain level of 2, while the majority of male patients (n=3) reported an operative pain level of 1. As for the experimental group, both female and male patients reported an operative pain level of 1. Thus, in the experimental group, females more frequently reported a lower VAS-score, whereas in the control group, males reported higher pain levels (VAS-score 3-4). In the experimental group, there were no patients with VAS > 3, whereas in the control group, there were two patients with high VAS-scores (3 and 4). This suggests a possible difference in pain perception according to gender between the two groups, indicating a potential positive effect of the experimental treatment. However, according to the Chi-square coefficient, these differences between the two groups and genders are not statistically significant (p > 5%) (Table 2).
|
Experimental group versus
Control group |
Value |
df |
Asymptotic Significance
(2-sided) |
|
|
Experimental Group |
Pearson Chi-Square |
2.583a |
3 |
0.461 |
|
Likelihood Ratio |
3.649 |
3 |
0.302 |
|
|
Linear-by-Linear Association |
0.235 |
1 |
0.628 |
|
|
N of Valid Cases |
17 |
|
|
|
|
Control Group |
Pearson Chi-Square |
4.821b |
4 |
0.306 |
|
Likelihood Ratio |
6.359 |
4 |
0.174 |
|
|
Linear-by-Linear Association |
1.885 |
1 |
0.17 |
|
|
N of Valid Cases |
15 |
|
|
|
Table 2: Chi-Square Test.
As for the distribution between the two groups by gender; in the experimental group, the female gender clearly dominates, compared to the control group, where the gender distribution is somewhat more balanced between females and males (Graph 1 and 2).
Graph 1: “Gender distribution of patients in the Experimental Group”.
Graph 2: “Gender distribution of the patients in Control Group.
In the statistical analysis between the two groups, the question arises: Does the duration of the intervention affect the level of pain reported by patients (VAS-score)? For this, the Pearson correlation coefficient was used, two-tailed test (Table 3).
|
Operative
time (in minutes) |
Visual
Analog Scale |
|||
|
Experimental |
Operative
time (in minutes) |
Pearson
Correlation |
1 |
.693** |
|
|
Sig.
(2-tailed) |
|
0.002 |
|
|
Group |
N |
17 |
17 |
|
|
|
Visual
Analog Scale |
Pearson
Correlation |
.693** |
1 |
|
|
Sig.
(2-tailed) |
0.002 |
|
|
|
|
N |
17 |
17 |
|
|
Control
Group |
Operative
time (in minutes) |
Pearson
Correlation |
1 |
.642** |
|
Sig.
(2-tailed) |
|
0.01 |
||
|
N |
15 |
15 |
||
|
Visual
Analog Scale |
Pearson
Correlation |
.642** |
1 |
|
|
Sig.
(2-tailed) |
0.01 |
|
||
|
N |
15 |
15 |
||
Table 3: Intervention Time and VAS-Score Correlation.
The table shows that for the experimental group, there is a strong positive correlation (r = 0.693), statistically significant (p = 0.002), between the duration of the intervention in minutes and the level of pain (VAS-score), which implies that with the increase in the duration of the intervention, it is expected that the level of operative pain will also increase. Similarly, for the control group, the correlation is positive (r = 0.642) and statistically significant (p = 0.01), but weaker compared to the experimental group (Graph 3).
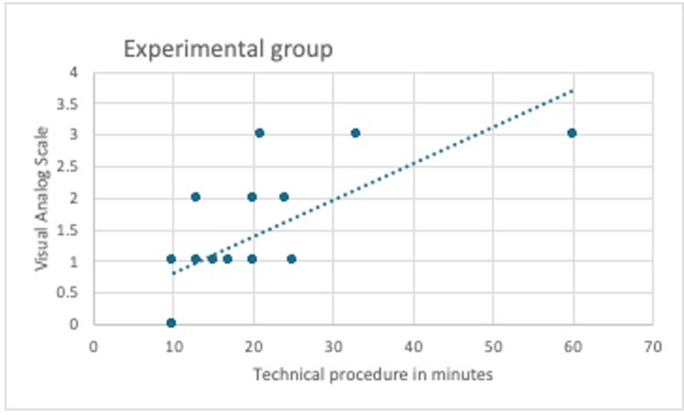
Graph 3: Linear correlation line in the experimental group.
The relationship between operative time and VAS-score showed a more linear pattern in the experimental group, suggesting a clearer association. If we compare the two techniques on comparative levels, the mean VAS-score for the experimental group results in an average of 1.4, whereas for the control group it averages 1.6. Part of the analysis also included the question of whether there is a statistically significant difference in the mean VAS-score between the two groups. For this purpose, the Student’s t-test for two independent samples was used (Cut technique versus traditional technique).
Surgical Technique
The teeth were extracted under local anesthesia (4% articaine with 1:100000 epinephrine), followed by a sulcular incision from the mesiobuccal part of the second molar to 1.5 cm distally along the mandibular ramus. Careful elevation of the mucoperiosteal flap was performed. With a high-speed bur under irrigation with saline solution or with piezosurgery, bone around the crown of the tooth was removed up to the enamel-cementum junction. Then, using a high-speed contra-angle handpiece and a carbide bur, the tooth was sectioned under irrigation with physiological saline. In the experimental group, the upper part of the crown was first sectioned halfway through its depth with a horizontal cut; then the upper crown segment was fractured using a straight elevator. Afterwards, the lower part of the crown was further sectioned using the bur, creating an imaginary line at the bottom of the tooth that serves as a barrier to protect the nerve. The bone is not drilled beyond this depth. The crown segment is then fractured and removed with the elevator. Once the crown is sectioned, a straight elevator is used to check for movement of the root block by placing the tip between the bone and the tooth. If the root block moves, extraction is attempted with the elevator. If no movement occurs, the roots are sectioned in the middle, and the straight elevator is used again to check for luxation by inserting the tip between the bone and the root. If luxation occurs, the root that is positioned higher is removed first, followed by the lower one. If there is no luxation, the upper root segment in the visible area is sectioned and removed, followed by the removal of the lower root with the elevator, and finally, the upper root is removed with a triangular elevator (Figure 1).
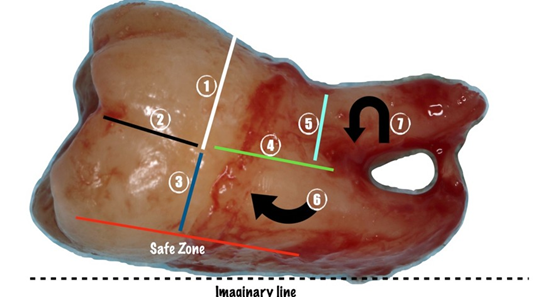
Figure 1: “Cut as you go” technique.
In the control group, tooth sectioning was performed in a T-shape, according to the technique described in the literature (study reference no. [12]) (Figure 2).
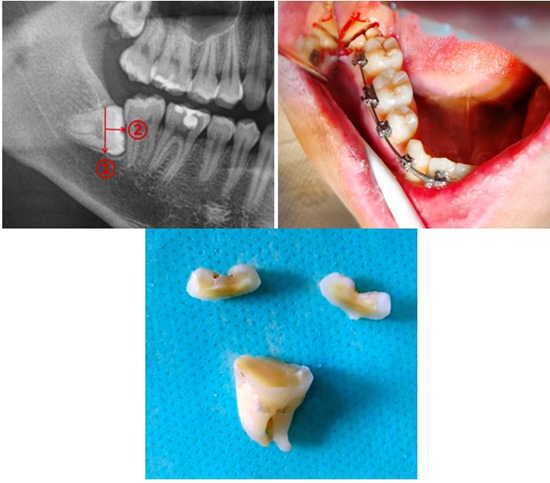
Figure 2: Demonstration of the T-shape technique by the author (He et al., Horizontal Third Molar Removal by T-Shaped Sectioning, J Oral Maxillofac Surg 2024).
After the extraction of the tooth, the bone edges were smoothed, the socket was irrigated with 0.9% saline solution, a hemostatic sponge was placed, and suturing was performed using 4.0 sutures.
Results
In this study, 32 patients underwent extraction of mandibular third molars, of whom 17 patients underwent extraction using the “Cut as you go” tooth sectioning technique, and in 15 patients the tooth was extracted using the T-shape technique. Referring to the level of patient satisfaction on the 3rd and 7th postoperative days for both techniques, we observe an increase in patient satisfaction from day 3 to day 7 for both techniques. Specifically, the ranking of satisfaction levels on the 3rd day in the control group starts from 6 and above, with levels 8 and 9 being predominant, averaging a value of 8.2 on the 3rd day (Graph 4).
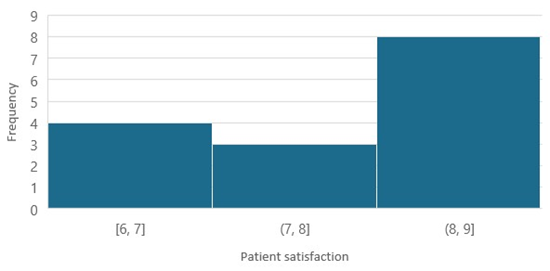
Graph 4: Patient satisfaction on 3rd day, Control Group.
Whereas in the experimental group, with an average patient satisfaction score of 8.5, there is also the presence of levels 9 and 10 of satisfaction, which are absent in the control group (Graph 5).
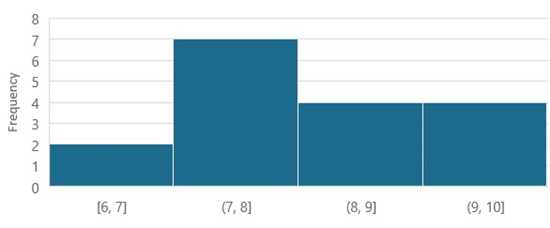
Graph 5: Patient satisfaction on 3rd day, Experimental Group.
In both groups, an increase in operative time corresponds to an increase in pain intensity, but statistical analysis confirms that the stronger effect is observed in the experimental group (“Cut as you go” technique) compared to the control group (traditional technique). The study found that men and women experienced pain differently, and in the group that received “Cut as you go technique”, showed a positive effect, meaning that this technique helped reduce pain or improve pain experience more effectively, suggesting that the treatment had a beneficial impact, especially when considering gender differencies. The Student’s t-test for two independent groups suggested a potentially clinically significant difference in VAS-score values between the two groups, but the small sample size limits the generalizability of the result. While the level of patient satisfaction increases for both groups on the 7th day, levels 9 and 10 of satisfaction clearly dominate in the experimental group (Graphs 6,7).
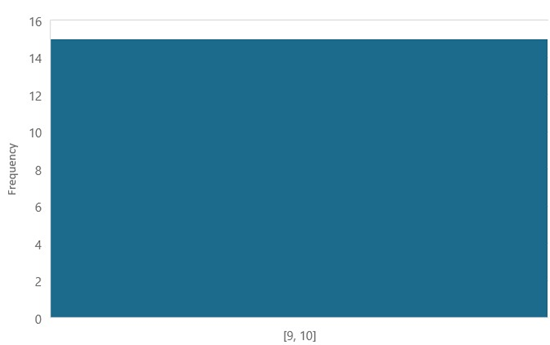
Graph 6: “Patient satisfaction on day 7, Experimental Group.
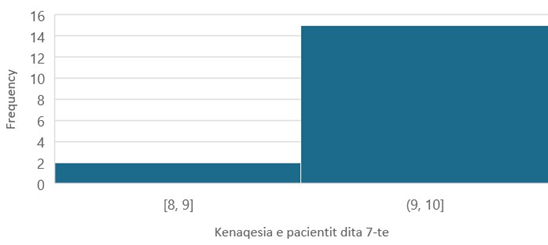
Graph 7: “Patient satisfaction on day 7, Control Group.
The average duration of the intervention in minutes was shorter for the experimental group (20 minutes) than for the for the control group (25 minutes). Also the average of VAS-score for each group is lower in the experimental group than the control group, suggesting that shorter operative time may contribute to less postoperative pain, particularly in the group treated with the “Cut as you go” technique. Therefore, surgical technique not only affects operative ease but also impacts patient comfort postoperatively. The linear correlation between operative time and VAS-score was stronger in the experimental group ( r=0.69) than in the control group (r=0.64), indicating a more pronounced linear relationship.
Discussion
The procedure of removing mandibular third molars is greatly influenced by the size, shape, and position of the roots. Our study aimed to compare two different tooth sectioning techniques in terms of duration, intraoperative pain, and postoperative satisfaction. To avoid postoperative complications in the removal of third molars, various authors have described different techniques for third molar extraction. Among all techniques, those involving tooth sectioning with a bur with the support of piezosurgery have proven to be less invasive, with shorter operative times and fewer postoperative complications [13] Tooth sectioning is performed with a bur or piezo surgery to facilitate disimpaction. In classical techniques, the crown is sectioned first, followed by root sectioning, and various authors have studied the advantages of these approaches [14-15]. There are many studies related to the extraction of impacted teeth. In a study by Liao et al., the removal of the third molar is performed using only a single incision. In one of his studies, Zeng J. [16] states that he designed an innovative digital technique for tooth sectioning, which proved to be successful and predictable in the removal of third molars. Meanwhile, the author Wang et al. [17] proposed a technique involving the sectioning of the tooth into three parts. The main advantage of the “Cut as you go” technique is that it makes the extraction procedure less complex and gives the surgeon more freedom of action, without strictly adhering to predefined sectioning cuts. Another benefit of the “Cut as you go” technique is that it increases surgical safety. By preserving a very small segment of the tooth without cutting it with a bur and instead fracturing it with an elevator, the technique provides More assurance that the inferior alveolar nerve will not be damaged. Typically, the operative time for third molar extraction depends on the depth of impaction, the complexity of the procedure, the difficulty of the surgery, and the experience of the surgeon. We hypothesized that the “Cut as you Go” technique would shorten the operative time and reduce postoperative pain compared to traditional tooth sectioning methods. In our study, the operative time was shorter in the experimental group than in the control group, suggesting that flexibility in sectioning simplifies the extraction. Our study also showed that operative time is directly related to postoperative pain. Patient satisfaction was good in both groups, which we believe is related to the use of piezosurgery. The results of this study showed that in no case was there any damage to the inferior alveolar nerve. However, this study is not without limitations. One limitation is that all surgeries were performed by a single surgeon. Another limitation is the small number of cases included in the study. that real effects may exist, but a larger sample size would be necessary to obtain statistically significant results.
Conclusion
In conclusion, the “Cut as you Go” technique is faster and gives the surgeon greater freedom of action than the “T” technique, while reducing postoperative complications and increasing patient satisfaction.
References
- Aristotle. Minor Works (1936) Cambridge, MA: Harvard University Press
- Gualteri H. In: Acute treatment of diseases of children with various observations, Cramer & Perachon; 1727.
- Grooss KS (1990) In: Cornelis Solingen: A Seventeenth-Century Surgeon and His Instruments, Netherlands: Leiden:Museum Boerhaave
- Kells CE (1918) Impacted lower third molars. Dental Cosmos. 60: 101107.
- Winter GB (1926) Principles of Exodontia as Applied to the Impacted Mandibular Third Molar. A Complete Treatise on the Operative Technic with Clinical Diagnoses and Radio-graphic Interpretations. St. Louis, MO: American Medical Book Comp.
- Thoma KH (1932) The management of malposed inferior third molars.J Dent Res. 12: 175-208.
- Fry ËK (1933) The third molar. Br Dent J. 54: 385-388.
- Kilpatrick H (1958) Removal of impacted third molars utilizing speeds up to 200,000 R.P.M. Oral Surg Oral Med Oral Pathol. 11: 364-369.
- Ries Centeno GA (1960) The Impacted Lower Third Molar. Buenos Aire, Argentina: El Ateneo
- Szmyd L (1971) Impacted teeth. Dent Clin North Am. 15: 299-318.
- Zhang Y, Chen X, Zhou Z, et al (2021) Effects of impacted lower third molar extraction on periodontal tissue of the adjacent second molar. Ther Clin Risk Manag 17: 235-247.
- He et al (2024) Horizontal Third Molar Removal by T-Shaped Sectioning. J Oral Maxillofac Surg
- Jain N, Thomas S, Prabhu S, et al (2016) Influence of tooth sectioning technique and various risk factors in reducing the IAN injury following surgical removal of an impacted mandibular third molar. Oral Maxillofac Surg 20: 149-156
- Agarwal SS, Xavier F, Rao S, Galhotra V (2023) Does the tooth sectioning method impact surgical removal of the distoangular impacted mandibular third molar? J Oral Maxillofac Surg 81: 318-328
- Szalma J, Vajta L, Olasz L, Lempel E (2019) Tooth sectioning for coronectomy: How to perform? Clin Oral Investig 23: 519-527
- Zeng J, Jiang Y, Liu Y, Hu Y, Guo C et al (2023) Research on a novel digital tooth sectioning guide system for tooth sectioning during mandibular third molar extraction: An in vitro study. J Stomatol Oral Maxillofac Surg 124: 101383
- Zheng X, Lin X, Wang Z (2020) Extraction of low horizontally and buccally impacted mandibular third molars by three-piece tooth sectioning. Br J Oral Maxillofac Surg 58: 829-833.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.