Cosmetic Surgery A Three-Dimensional Model Study on Beauty Standards for Cheekbones in Both Sexes
by Emile Huybrecht, Kurt Barbé, Maurice Y. Mommaerts*
European Face Centre, Vrije Universiteit Brussel, Universitair Ziekenhuis Brussel, Brussels, Belgium
*Corresponding Author: Maurice Mommaerts, European Face Centre, UZ Brussel, Laarbeeklaan 101, 1090 Brussels, Belgium
Received Date: 23 June 2025
Accepted Date: 27 June 2025
Published Date: 30 June 2025
Citation: Huybrecht E, Barbé K, Mommaerts MY (2025) Cosmetic Surgery A Three-Dimensional Model Study on Beauty Standards for Cheekbones in Both Sexes. J Surg 10: 11363 https://doi.org/10.29011/2575-9760.011363
Abstract
The aim of this study was to determine whether a ‘beautiful’ malar morphology is gender-specific and whether volume/projection play a role in aesthetic perception. Models of one female and one male face, selected in a two-stage process, were three-dimensionally printed. One hundred assessors were asked to identify the male and female faces based on cheekbone morphology. Using design software, the malar bones were transposed from male to female and vice versa. The assessors were again asked to identify the male and female faces. Next, volume and projection were added/reduced to create a series of four models for each sex. The assessors were asked to evaluate these for facial harmony in the malar area on a visual analogue scale. The original female and male models were wrongly classified by only 3% and 2% of the assessors, respectively. Regarding the transposed models, 96% of the female faces with male malar contours were classified as masculine, while 91% of the male faces with female malar contours were classified as feminine. In the evaluation of volume/projection, the original malar prominences scored significantly higher than the altered ones. A clear preference for more volume and projection in the female model was observed among the study assessors. Less volume and projection were preferred in the male model.
Keywords: 3D Printing; Cheek; Esthetics; Malar Bone; Questionnaires; Sex; Surveys
Introduction
In White European individuals, a distinct malar prominence is often considered a sign of beauty and youth. However, objective evaluation of the cheekbone is hindered by the lack of anthropometric and cephalometric landmarks along its curves. The ‘perfect’ shape of a malar prominence has never been determined. Renaissance artists coined the term ‘pommette’ to help depict an ideal malar prominence on a two-dimensional canvas. Historically, makeup artists have highlighted the highest point of the malar prominence with rouge to enhance its appearance. The projection of the malar prominence can be surgically increased using onlay, osteotomy, and filler techniques [1-12]. Osteotomies use the pre-existing shape of the malar bone, whereas implants and injectables can be more readily customized. However, the ‘perfect’ shape and volume remain a matter of aesthetic preference [13-22].
This study aimed to determine whether a ‘beautiful’ malar morphology is gender-specific and whether volume/projection plays a role in aesthetic perception using a 3D model simulation.
Materials and Methods
Assessors
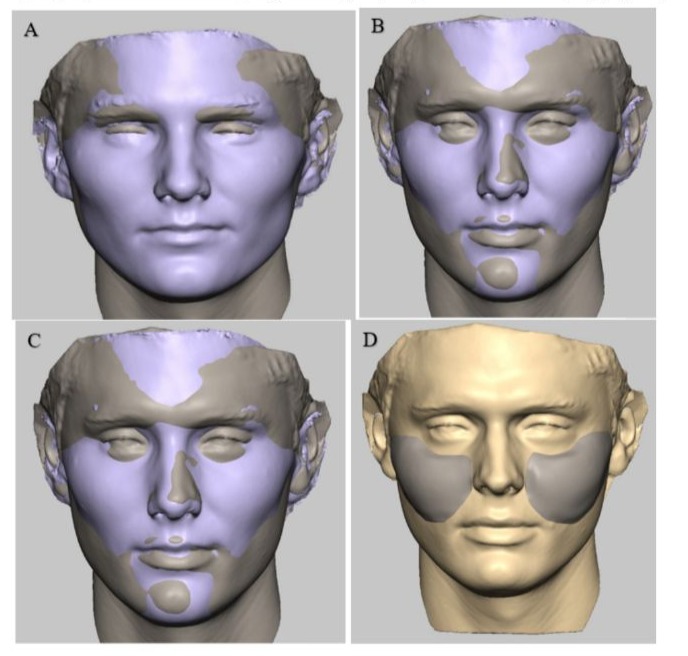
One hundred assessors (50 male, 50 female) were randomly recruited from among the hospital staff on a first-come, first-served basis. The inclusion criterion for participation was voluntary agreement to evaluate 12 models. The study was exempt from ethics committee approval because no human subjects were directly involved. Model Subjects and Optical Face Scanning. To recruit a ‘typical’ gender-specific face, six hospital staff members at the study institution (three male, three female) were selected by 43 co-workers. These 43 co-workers (unknown male/female ratio) were not involved in the model assessments; they selected the six staff members based on personal encounters and visual inspection. The six members of staff verbally consented to having their facial photographs taken. A photographic set (full-face frontal and profile views) of the six subjects was further evaluated by a panel of 12 departmental co-workers (all White, randomly selected, eight female and four male) to determine the most harmonious subject to represent each sex. The selected male and female subjects (one of each; both White) underwent an optical face scan using a handheld 3D scanner (Eva, Artec, Luxembourg); the scans were stored in Stereolithography (STL) file format. The subjects verbally consented to having the optical scans taken and used for this specific research project. Modification of STL Files to Transpose Male Cheekbones to the Female Face and Vice Versa. The STL files were edited with precision voxel 3D sculpting and modeling software (Geomagic Sculpt; 3D Systems, Rock Hill, SC, USA) to exchange the malar projections between the selected male and female subjects. After correction for sexual dimorphism (the male facial index is 112% of the female), matching of the male and female faces was performed using a function called ‘positioning registration.’ The malar prominences were then exchanged between the male and female subjects, resulting in four models: Female Original (FO), Female Masculinized (FM), Male Original (MO), and Male Feminized (MF) (Figure 1).
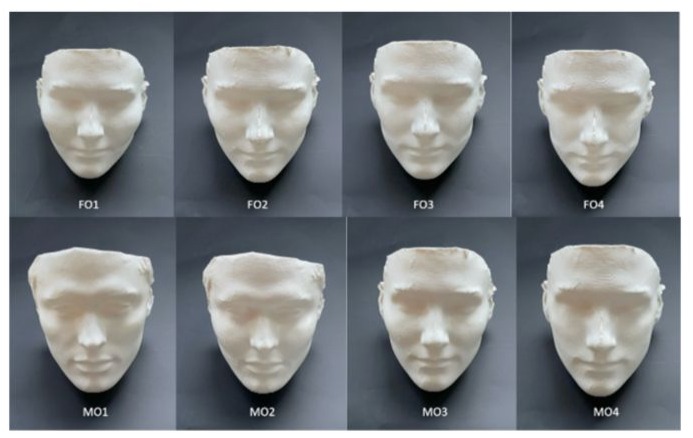
Using the same software, the original models (FO and MO) were cloned with size differences in the malar projections. The differences were calibrated with fixed steps using a standardized grid to augment and reduce the malar prominence in both the lateral and anteroposterior directions, resulting in four models for each sex: female original 1, 2, 3, and 4 (FO1, FO2, FO3, and FO4) and male original 1, 2, 3, and 4 (MO1, MO2, MO3, and MO4) (Figure 2). O1 represented an augmented malar prominence, O2 the original prominence, O3 a reduced prominence, and O4 a further reduced prominence.
Multiple functions such as ‘de-feature,’ ‘smooth area,’ and ‘fill area’ were used to eliminate borders and make each 3D model look as natural as possible. Each 3D model was saved and exported as an STL file.
Physical Model Setup
A 360° visual examination of highlights and shadows in the 3D models was conducted to gain more realistic impressions than a 2D representation on a computer monitor. Hence, all STL files (FO, FM, MO, MF, FO1, FO2, FO3, FO4, MO1, MO2, MO3, and MO4) were imported into MakerBot Desktop software (MakerBot Industries, Brooklyn, NY, USA) and 3D-printed using the MakerBot Replicator 2 Desktop Fused Deposition Model (FDM) 3D printer. The models were printed in polylactic acid using rafts, supports, a layer height of 0.2 mm, an extruder temperature of 230°C, and on a 55% scale to allow for improved manual handling. The assessors were shown each white model on a table with a black background, starting with the FO, FM, MO, and MF group (evaluation of gender specificity), followed by the FO1, FO2, FO3, FO4, MO1, MO2, MO3, and MO4 group (evaluation of volume/projection). They were allowed 30 seconds to evaluate each model and answer the corresponding question. The evaluation was performed in a single session, in a silent room, and without the presence of third parties or exchanges of opinion. To prevent pattern bias during the assessment, the sequence of appearance of the models was randomized.
Questionnaires
After informed consent was obtained, the survey began with questions about the assessor’s age, gender, sexual orientation, and highest level of education attained (high school certificate, bachelor’s degree, or master’s degree). All recorded data remained anonymous. In addition to these demographic data, the survey consisted of three questions. The initial question was asked to sensitize the assessor to subsequent questions focusing on the malar region.
Question 1: How important would you score the malar region in assessing the beauty of one’s face on a Visual Analogue Scale (VAS) from 0 (unimportant) to 10 (very important)? This was noted as the ‘zygoma score.’
Question 2: You will see four models, one by one, in a randomized sequence. Would you define each of these models as rather masculine or feminine? No indication of the possible sex distribution of the models was provided.
Question 3: You will see eight models, one by one, in a randomized sequence. Score each of them on a VAS from 0 (unattractive) to 10 (very attractive). Randomization of the models was performed using random sequencing software (https://www.randomizer.org), which generated a random number sequence from 1 to 4 for question 2 and from 1 to 8 for question 3.
Data Transformation and Statistical Analysis
Every assessor was asked to rate each cheekbone of the two sexes in a randomized order, and a repeated-measures model was employed to assess within-group differences. Additionally, the influence of the assessor’s gender and highest level of education on the scoring was assessed. The gender and highest level of education of the assessors were unpaired groups, so the data were analyzed using a mixed model. A mixed model is a statistical model containing both fixed and random effects. A mixed-model statistical analysis was also used to check for the presence of an interaction between zygoma gender and type of malar prominence, as well as a second interaction between the gender of the assessor and that of the cheekbone. The presence of the first interaction implies that scoring of attractiveness as a function of volume depends on the gender of the model. The presence of the second interaction implies that men and women score the same and opposite genders differently. Additionally, it was checked whether the zygoma score, highest level of education, gender, and/or sexual orientation of the assessor confounded the scoring by including these variables as main effects for possible correction. A detected violation in homoscedasticity during the repeated scoring by the assessors indicated a potential learning effect, so a Greenhouse–Geisser correction was used for each repeated-measures variable. A residual analysis to study the normality of the residuals of the mixed model was performed using a probability–probability graphical assessment. Further, a descriptive analysis was used to describe the false classification of sex, since no scores were assigned for the evaluation of sex. Complete descriptive data are not reported here but are available upon request. The statistical analyses were performed using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA).
Results
Assessor Demographics
A total of 100 assessors participated and successfully completed the survey. Of these, 50 were female (mean age: 36.3 years, range: 19–63 years) and 50 were male (mean age: 38.2 years, range: 21–70 years). The racial distribution consisted of 97 White participants, two Asian participants, and one Black participant. The average completion time for the evaluation was 6 minutes and 11 seconds. Overall, 62% of the assessors were younger than 40 years of age. Regarding educational attainment, 41% had a high school certificate, 26% held a bachelor’s degree, and 33% had a master’s degree. Five assessors (5%) identified as having a homosexual orientation. However, due to the low sample size, sexual orientation was not included as a confounding variable. The statistical analysis only considered differences due to highest level of education attained, gender, age, and zygoma score.
Statistical Model and Confounder Selection
To prevent overfitting, a forward selection approach was employed. This stepwise regression analysis began with an empty model, sequentially adding variables in order of statistical significance. The Akaike information criterion (AIC) was minimized to determine the final model. The selected confounders were:
- Gender (P < 0.01) for its interaction with model gender.
- Highest level of education (P < 0.01) as a main effect.
- Age (P > 0.05), which was excluded due to lack of significance.
- Zygoma score (P > 0.3), also excluded from the final model.
The mixed-model analysis was corrected for gender and highest level of education, while age and zygoma score were removed from the model due to statistical insignificance.
Importance of the Malar Region (Question 1)
Assessors rated the importance of the malar region in facial beauty on a visual analogue scale (VAS) ranging from 0 (unimportant) to 10 (very important). The mean zygoma score was 4.87 out of 10. However, no significant influence of zygoma score on the evaluation of 3D models was found (P = 0.343).
Gender Classification of Cheekbones (Question 2)
When evaluating the original models (FO and MO):
- Only 3 out of 100 assessors incorrectly classified the FO model (female original).
- Only 2 out of 100 assessors incorrectly classified the MO model (male original).
- For the transposed models (FM and MF):
- 96% of assessors classified female faces with male malar contours as masculine.
- 91% of assessors classified male faces with female malar contours as feminine.
Evaluation of Volume and Projection (Question 3)
The interaction between gender and malar prominence type is illustrated in Figure 3.
- The original malar prominences (FO2 and MO2) systematically received the highest scores:
- FO2: Mean score = 7.0
- MO2: Mean score = 6.8
- In the female group, the modified models FO1, FO3, and FO4 received significantly lower scores (P < 0.001):
- FO1: Mean score = 3.3
- FO3: Mean score = 3.8
- FO4: Mean score = 2.5
- In the male group, the modified models MO1, MO3, and MO4 were scored higher than their female counterparts:
- MO1: Mean score = 4.7
- MO3: Mean score = 5.4
- MO4: Mean score = 4.7
Scores systematically decreased with greater deviation from FO2 and MO2, indicating a clear preference for the original malar prominence over augmented or reduced projections.
Influence of Gender and Educational Level on Scoring
Additional analyses revealed:
- Models of the opposite sex received significantly higher scores (P = 0.007).
- Highest level of education had the greatest influence on scoring, but no interactions were observed between education level and either malar prominence type or model gender.
- Assessors with a high school diploma assigned significantly higher scores than those with a bachelor’s degree (P < 0.01).
- Assessors with a master’s degree scored in between these two groups.
- Since no significant interactions were detected between education level and gender or malar prominence type, this trend applied consistently across all models.
Discussion
Gender-Specific Malar Prominence
Defining the ideal gender-specific malar prominence remains complex. Many studies have attempted to describe the ideal area of maximal projection, but few have validated these descriptions based on aesthetic preference and gender traits [18,26-28]. Determining ‘aesthetic appreciation’ is best conducted through panel surveys incorporating both laypeople and professionals, utilizing a Likert scale or Visual Analogue Scale (VAS) for scoring. In this study, both laypeople and professionals assessed malar prominences using fused deposition 3D-printed models. The advantage of this approach is the ability to view the malar prominence from all angles (360°) rather than relying on a Two-Dimensional (2D) computer display. Conventional 2D photoshopping techniques lack the ability to accurately simulate depth and projection, making 3D models a superior method for evaluating malar aesthetics.
The Role of Malar Prominence in Gender Classification
The results indicated that assessors considered the malar region an important feature for distinguishing male from female faces. When the female malar shape was replaced with the male counterpart (and vice versa), assessors readily identified these changes, reinforcing the notion that malar morphology plays a key role in gender perception. Although this study did not establish an idealized female or male cheekbone, it confirmed that cheekbone morphology is strongly associated with gender perception.
Influence of Volume and Projection on Aesthetic Scoring
Interestingly, greater volume and projection in female cheekbones did not necessarily result in higher attractiveness scores. The altered female models with increased volume and projection received lower VAS scores, which suggests that larger malar prominences are not always perceived as more beautiful. In contrast, reducing the volume and projection of male cheekbones led to higher scores, indicating that less prominent cheekbones were preferred for male models. The study findings suggest that aesthetic preferences for malar projection differ between males and females. Strong, defined cheekbones are traditionally considered attractive in men, yet excessive prominence did not enhance attractiveness scores in this study. Similarly, while well-defined cheekbones are often associated with femininity, excessive augmentation in female models resulted in a decline in attractiveness ratings.
Impact of Malar Modifications on Perceived Beauty
- Female models with excessive or reduced malar projections received significantly lower VAS scores (mean scores: 3.3, 3.8, and 2.5 for FO1, FO3, and FO4, respectively).
- Male models with modified cheekbone projections were less affected by volume alterations and scored closer to their original form.
- The further reduced female malar prominence model (FO4) received the lowest VAS score (2.5), categorizing it as borderline unattractive.
- Male cheekbone alterations had a less pronounced effect on attractiveness scores, indicating that male facial attractiveness may be less dependent on malar prominence than female facial aesthetics.
Study Limitations and Future Research Directions
This study does not establish a universal guideline for malar augmentation procedures but does provide evidence that ideal cheekbone morphology is gender-dependent. The findings highlight the need for patient-specific planning in facial aesthetic interventions.
Future research should:
- Investigate the ideal location of maximal projection in male and female cheekbones.
- Further explore the relationship between malar projection, facial harmony, and overall attractiveness.
- Assess cultural and ethnic variations in malar prominence preferences.
References
- 1. Layoun W, Guyot L, Richard O, Gola R (2003) Augmentation of cheek bone contour using malar osteotomy. Aesthetic Plast Surg 27: 269-274.
- 2. Bettens RM, Mommaerts MY, Sykes JM (2002) Aesthetic malar recontouring: the zygomatic sandwich osteotomy. Facial Plast Surg Clin North Am 10: 265-277.
- Jones RH, Ching M (1995) Intraoral zygomatic osteotomy for correction of malar deficiency. J Oral Maxillofac Surg 53: 483-485.
- Salyer KE (1994) Malar augmentation using lamellar split osteotomy. J Craniofac Surg 5 :116-123.
- Gasparini G, Saponaro G, Moro A, Boniello R, Cervelli D, et al (2010) Zygomatic sagittal split osteotomy: a novel and simple surgical technique for use in midface corrections. J Craniofac Surg. 21: 1872-1875.
- Nout E, Cesteleyn LL, van der Wal KG, van Adrichem LN, Mathijssen IM, et al (2008) Advancement of the midface, from conventional Le Fort III osteotomy to Le Fort III distraction: review of the literature.Int J Oral Maxillofac Surg 37: 781-789.
- Mommaerts MY, Abeloos JV, De Clercq CA, Neyt LF (1995) The ‘sandwich’ zygomatic osteotomy: technique, indications and clinical results. J Craniomaxillofac Surg 23: 12-19.
- O’Hara KL, Urrego AF, Garri JI, O’Hara CM, Bradley JP, et al (2006) Improved malar projection with transconjunctival hydroxyapatite granules. Plast Reconstr Surg 117: 1956-1963.
- Reda-Lari A (2008) Augmentation of the malar area with polyacrylamide hydrogel: experience with more than 1300 patients. Aesthet Surg J 28: 131-138.
- Metzinger SE, McCollough EG, Campbell JP, Rousso DE (1999) Malar augmentation: a 5-year retrospective review of the silastic midfacial malar implant. Arch Otolaryngol Head Neck Surg 125: 980-987.
- Sevin K, Askar I, Saray A, Yormuk E (2000) Exposure of high-density porous polyethylene (Medpor) used for contour restoration and treatment. Br J Oral Maxillofac Surg 38: 44-49.
- Mole B (1992) The use of Gore-Tex implants in aesthetic surgery of the face. Plast Reconstr Surg 90: 200-206.
- Marianetti TM, Cozzolino S, Torroni A, Gasparini G, Pelo S (2015) The “beauty arch”: a new aesthetic analysis for malar augmentation planning. J Craniofac Surg 26: 625-630.
- Hinderer UT (1975) Malar implants for improvement of the facial appearance. Plast Reconstr Surg. 56: 157-165.
- Powell NB, Riley RW, Laub DR (1988) A new approach to evaluation and surgery of the malar complex. Ann Plast Surg 20: 206-214.
- Fonseca RJ, Marciani RD, Turvey TA (2008) Oral and maxillofacial surgery. 2nd ed. St Louis, MO: Saunders/Elsevier; 2008. p. 189-210.
- Wilkinson TS. Complications in aesthetic malar augmentation (1983) Plast Reconstr Surg 71: 643-649.
- Prendergast M, Schoenrock LD (1989) Malar augmentation: patient classification and placement. Arch Otolaryngol Head Neck Surg 115: 964-969.
- Mladick RA (1991) Alloplastic cheek augmentation. Clin Plast Surg 18: 29-38.
- Nocini PF, Boccieri A, Bertossi D (2009) Gridplan midfacial analysis for alloplastic implants at the time of jaw surgery. Plast Reconstr Surg123: 670-679.
- Terino EO (1992) Alloplastic facial contouring: surgery of the fourth plane. Aesthetic Plast Surg 16: 195-212.
- Arnett GW, Jelic JS, Kim J, Cummings DR, Beress A, et al (1999) Soft tissue cephalometric analysis: diagnosis and treatment planning of dentofacial deformity. Am J Orthod Dentofacial Orthop1 16: 239-253.
- Peck H, Peck S (1970) A concept of facial esthetics. Angle Orthod 40: 284-318
- Becking AG, Tuinzing DB, Hage JJ, Gooren LJ (2007) Transgender feminization of the facial skeleton. Clin Plast Surg 34: 557-564.
- Bruce V, Burton AM, Hanna E, Healey P, Mason O, et al (1993) Sex discrimination: how do we tell the difference between male and female faces? Perception 22: 131-152.
- Hinderer UT. Profileplasty (1971) The International Microform Journal of Aesthetic Plastic Surgery Card 1: No. 1.
- Wilkinson TS (1983) Complications in aesthetic malar augmentation. Plast Reconstr Surg 71: 643-649.
- Silver WE (1986) The use of alloplastic materials in contouring the face. Facial Plast Surg 3: 81-98.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.