Constrictive Pericarditis on the Basis of Recent Infectious Tuberculosis with Concomitant Situs Inversus: A Case Report
by Mascha von Zeppelin1*, Nobel Thaqi1, Robert Stöhr2, Thomas Walther1, Fabian Emrich1
1Department of Cardiovascular Surgery, Goethe University Frankfurt, University Hospital Frankfurt, Germany
2Department of Cardiology, Goethe University Frankfurt, University Hospital Frankfurt, Germany
*Corresponding author: Mascha von Zeppelin, Department of Cardiovascular Surgery, Goethe University Frankfurt, University Hospital Frankfurt, 60596 Frankfurt/Main, Germany
Received Date: 02 April 2026
Accepted Date: 09 April 2026
Published Date: 10 April 2026
Citation: Zeppelin MV, Thaqi N, Stöhr R, Walther T, Emrich F (2026) Constrictive Pericarditis on the Basis of Recent Infectious Tuberculosis with Concomitant Situs Inversus: A Case Report. Ann Case Report. 11: 2589. DOI: https://doi.org/10.29011/2574-7754.102589
Abstract
Background and Clinical Significance: Infectious tuberculosis remains a serious disease even today and has become increasingly important in medicine in recent years. Constrictive pericarditis, caused by active tuberculosis, is still a potentially life-threatening disease. Coincidence with situs inversus totalis is very rare, although it does not influence the disease. We report on a 23-year-old eritrean patient with recent tuberculosis, which manifested itself pericardially, with simultaneous situs inversus.
Case Presentation: We report on a 23-year-old patient with recent tuberculosis, which manifested itself pericardially, with simultaneous situs inversus. He underwent a pericardiectomy via median sternotomy, followed by a thoracotomy. He was discharged in stable condition with plans for continued outpatient care.
Conclusion: Active tuberculosis remains a disease of increasing relevance today. Surgical pericardectomy can be an effective treatment strategy for infectious constrictive pericarditis.
Keywords: Pericarditis constrictiva; Infectious Tuberculosis; Perikardectomy
Introduction
Despite advances in modern medicine, pericarditis remains a potentially life-threatening condition associated with diastolic dysfunction [1]. Normally, the heart is enveloped by the non-elastic pericardium, which consists of a parietal and a visceral layer. Inflammatory remodeling processes in constrictive pericarditis lead to fibrosis and calcification, which reduces elasticity.
Although the majority of cases are idiopathic or viral in origin, bacterial causes are among the rarest etiologies, accounting for approximately 3-7% of all cases [2]. Situs inversus totalis is described in the literature with an incidence of one birth in 5,000 to 20,000 [3]. Although no coincidence between the two clinical diseases is described in the literature, the occurrence of both diseases is even rarer
Case Presentation
We present a 23-year-old patient with infectious pericarditis due to tuberculosis, with concomitant situs inversus totalis. He is from Eritrea and had been living in Germany for one and a half years. The patient stated that he had never been ill before and lived in a stable environment. His medical history included pain in the flank region for two weeks, as well as respiratory-dependent chest pain and cough with whitish sputum. The patient was referred to our clinic with polyserositis, right-sided pleural effusion, and a circular pericardial effusion of up to 1.7 cm end-diastolic (Figure 1).
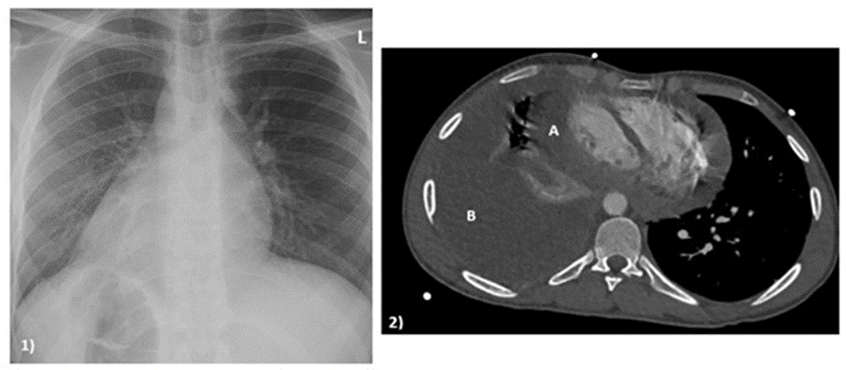
Figure 1: preoperative diagnostics. 1) X-ray in october 2025; 2) Computertomography in december 2025; A: thickened pericardium with effusion component; B: massive pleural effusion.
There were slightly elevated laboratory signs of inflammation and a febrile body temperature. The microbiological results did not reveal any evidence of pathogenes, in particular no evidence of tuberculosis. Only the Quantiferon test was slightly positive. Echocardiography revealed constrictive pericarditis with a dilated inferior vena cava and no respiratory variability. Furthermore, there was early inflow across the mitral valve during inspiration by 20-25%, as well as an increase in early inflow across the tricuspid valve by over 45%. In view of the symptoms, a pericardectomy was indicated (Figure 2).
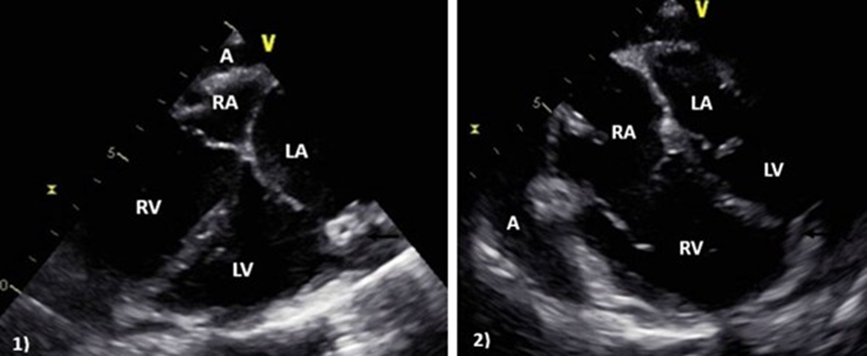
Figure 2: Intraoperative echocardiography; A: pericardial effusion, RA: right atrium, RV: right ventricle, LA: left atrium, LV: left ventric
le; in these images, the pronounced echogenicity caused by pericarditis is clearly visible.
After placing safety wires via the right groin, the procedure was performed via median sternotomy without the use of a heart-lung machine. The pericardium was then opened. This revealed pronounced adhesions and granulomas of the pericardium and myocardium. Macroscopically, the granulomas were in an early stage of the disease. We performed an anterior pericardectomy, which extended to the phrenic nerves on both sides. To avoid postoperative diaphragmatic elevation, a safety margin of approximately 1 cm was maintained on both sides. We sent samples of the removed material to histology and microbiological examination for polymerase chain reaction (PCR) testing and detection of bacteria and fungi. Intraoperatively, pleural effusions were found on both sides, with chambered portions on the right side. After inserting drains, the thorax was closed in a standardized manner (Figure 3).
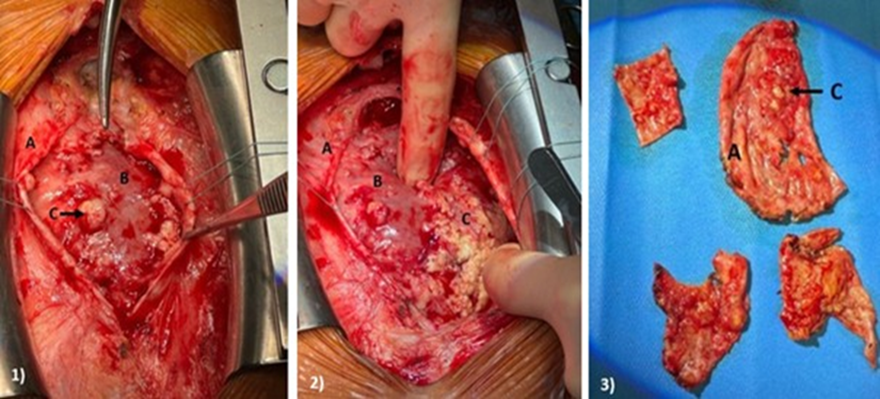
Figure 3: Intraoperative images: 1 and 2: Intrathoracic view after median sternotomy; 3: Pericardium after resection; A: Pericardium; B: Myocardium; C: Granulomas.
The patient recovered quickly and was extubated within four hours after the procedure. In the short term after the procedure, the chambered pleural effusion on the right side closed, resulting in mediastinal displacement. With Computer tomography (CT) radiological evidence of pleural empyema, emergency right-sided empyema evacuation with decortication and adhesiolysis was performed (Figure 4).
Subsequently, evacuation of a left-sided empyema was carried out using thoracoscopic technique. The postoperative course was uneventful, and the patient was discharged in stable condition with plans for continued outpatient care.
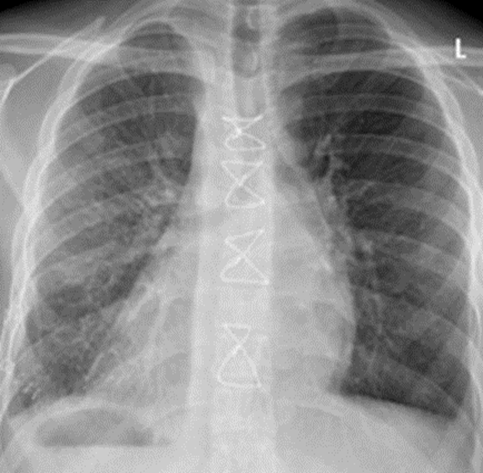
Figure 4: Postoperative X-ray after successful treatment.
Initial conventional microbiological cultures remained negative. Histopathological examination revealed active inflammation with focal formation of necrotizing epithelioid cell granulomas. However, molecular biological diagnostics ultimately identified the causative pathogen, allowing targeted antimicrobial therapy to be initiated in accordance with the antibiogram.
Discussion
The source of infection remains unclear in a patient who has been living in Germany for almost two years, far away from refugee shelters or similar facilities. A previous infection with an outbreak of the disease after several years seems rather unlikely.
Conclusion
This case highlights pericardectomy as an effective therapeutic option in severe infectious pericarditis and underscores the critical role of molecular diagnostic testing in contemporary clinical practice.
Declarations
Abbreviations:
The following abbreviations are used in this manuscript:
CT: Computer tomography; LA: Left atrium; LV: Left ventricle; PCR: Polymerase chain reaction; RA: Right atrium; RV: Right ventricle.
Contributors: M.v.Z. and F.E: conceptualization, methodology, formal analysis, inves-342 tigation, writing-original draft preparation. M.v.Z. and F.E.: data curation and visualization. N.T., R.S. and T.W.: writing-review and editing. T. W. and F. E.: supervision. All authors have read and agreed to the published version of the manuscript
Competing interests: None
Patient consent for publication: Informed consent was obtained from the patient, consent form available upon request / Not applicable.
Ethics approval and consent to participate: Ethical approval for this publication by IRB at Kern Medical / Not applicable
Availability of data and materials: Not applicable
Funding: This research received no external funding.
References
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, et al. (2016). 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 37: 2129-2200.
- Adler Y, Charron P, Imazio M, Badano L, Barón-Esquivias G, et al. (2015). 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC)Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 36: 2921-2964.
- Koç A. (2021). Situs inversus totalis. Anästhesiologie & Intensivmedizin; 62: S211-S220.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.