Conquering Mt. Everest: 222 Apnea Dives to 20 m Depth: A Detailed Case Report
by Olaf Schedler1*, Jochen D Schipke2, Sven Dreyer3
1Bavaria Klinik Kreischa, Abteilung Sportmedizin, An der Wolfsschlucht 1-2, D-01731 Kreischa, Germany
2Research Group Experimental Surgery, University Hospital Düsseldorf, Moorenstrasse 5, D-4022 Düsseldorf, Germany
3Hyperbaric Oxygen Therapy, University Hospital Düsseldorf, Moorenstrasse 5, D-40225 Düsseldorf, Germany
*Corresponding author: Olaf Schedler, Bavaria Klinik Kreischa, Abteilung Sportmedizin, An der Wolfsschlucht 1-2, D-01731 Kreischa, Germany
Received Date: 20 December 2024
Accepted Date: 24 December 2024
Published Date: 26 December 2024
Citation: Schedler O, Schipke JD, Dreyer S (2024) Conquering Mt. Everest: 222 Apnea Dives to 20 m Depth: A Detailed Case Report. Ann Case Report. 9: 2141. https://doi.org/10.29011/2574-7754.102141
Abstract
"Everesting" became a new endurance sport in which runners or cyclists ascend a cumulative elevation of 8,848 m on a defined route on a mountain. Freediving on Mt. Everest is also considered a discipline.
This new world record was achieved in an in-door pool by an athlete who descended and resurfaced 222 times on a 20-m dive in just under 13 hrs.
While Everesting runners or cyclists face minimal environmental hazards, our athlete faced such hazards like water temperature and pressure. Other influences involved the diving response, apnea, and submersion-induced blood volume shift.
For apneaists who engage in prolonged repetitive apnea dives, the many measured variables during this competition will contribute to further enhancing the safety of their demanding activity.
Introduction
The first event described as "Everesting" was by George Mallory, grandson of George Mallory, who disappeared on Mt. Everest, now a hundred years ago. This event became a new endurance sport in which athletes ascend a cumulative elevation of 8,848 m on a defined but freely chosen route on a mountain. The routes have thus far been completed by cyclists or runners [1]. The competition must be completed within maximally one day. E-bikes, tandems, and recumbent bicycles are not allowed for Everesting.
In cycling Everesting, a total elevation of 9,009 m was achieved over a period of 10 h and 30 min and a distance of 195 km. The ascent of the approximately 7 km long individual stretch reached up to 12%. In running, a height of 9,033 m was reached after 18 h and 34 min covering a total distance of 62 km. In virtual Everesting, spinning bikes are used, and athletes climb to the height of 8,854 m in the fitness center, covering a total distance of 209 km in 12 h and 19 min with gradients between 4 and 12%.
Freediving on Mt. Everest is also considered a discipline. The previous world record holder was the American Lance Lee Davis, who in 2020 dove 148 times to a depth of 30.5 m in the Pacific off Los Angeles, taking 14 h and 28 min to do so.

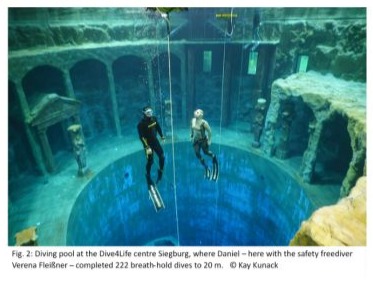
Daniel Weißhoff was nearly 1.5 h faster on January 12, 2024, after diving 222 times in apnea to a depth of 20 m and resurfacing in the diving pool at Siegburg's Dive4Life (Figure 1).
The record attempt of Free dive Everesting was accompanied and recognized by the 'Record Holders Republic' - Registry of Official World Records (no author listed, 2020).
Ordinary divers face many simple questions. What qualified the Berlin athlete for a world record? How did he manage the pressure equalization repeatedly? Why didn't he crush his nose? How did he deal with diver's diuresis? Was he chilled at the end? But also, more challenging questions arise, such as how did his cardiovascular system react to the 222 submersions, and above all: Why didn't the repetitive dives lead to pulmonary oedema or decompression sickness? All these questions will be answered below.
Athlete / Methods
Daniel, the Berlin athlete, ignited his passion for freediving at the age of 22 after a trial session at the ‘Berlin Diving Club’. He reduced his workload as a biotechnical assistant by half, dedicating more and more of his time to his hobby and his freediving school, the ‘Freediving Centre Germany’. Here, the highly decorated freediving instructor works alongside six other instructors.
Over time, Daniel continued to improve his performance: achieving a maximum static apnea of 6:38 min, becoming the 2021 German vice champion in the discipline of ‘Constant Weight Bifins in the lake’, and the German champion in the discipline of ‘Constant Weight in the lake’.
At the time of the world record, Daniel was 40 years old. With a height of 1.71 m and a body mass of 69 kg (20% body fat), this results in a normal range BMI of 23.6 kg/m².
Methods
Dive site
At the Dive4Life Centre (Siegburg, Germany) (Figure 2), divers enjoy a 20-m deep diving pool with a water temperature of 24°C. The surrounding spacious, dive-related facilities, maintain an air temperature of 26°C.
Equipment
To counteract cooling, a 5.5-mm Salvimar full-body neoprene suit with a hood was used. Buoyancy was balanced with 2.5 kg of neck weights and 1 kg of weight on the waist belt. Neoprene socks helped prevent chafing from the Leader fin carbon fibre fins on the feet.
For equalizing pressure during descent, the Frenzel manoeuvre [2], preferred by free divers, was repeated 222 times, and during each descent, it was repeated 13 times. With a total of 2,900 compressions of the nostrils, there was a risk of chafing, particularly in the nose-mouth area. Therefore, after every 25 dives, masks were alternated, each providing a different fit around the upper lip and nose.
The equipment also included a sports watch (Garmin, Descent G1), which was worn together with a chest strap. It documented the number of dives along with the duration of the competition for the later world record. At the same time, it also recorded heart rate, diving depth, and water temperature.
Protocol
The world record attempt started at 8:00 a.m. and ended 12 h, 57:09 min later. Daniel took 222 deep breaths at the surface. Then he actively dove headfirst and resurfaced actively at 20 m after a somersault. Each apnea dive lasted 45 s, followed by a surface pause of 2:15 min (Figure 3). According to this pattern, 25 dives formed a block of 75 min. A 15-min break followed each block.

During these breaks, Daniel stayed dry and used them for eating, drinking totalling six litters and visiting the ceramics department. Remarkably, to avoid major fluctuations in fluid balance, he also drank something after every five dives.
Perhaps most importantly, during the breaks, Prof. Dr. Olaf Schedler an expert in Maritime Medicine and Chief Physician at Bavaria Klinik Kreischa, Abteilung Sportmedizin conducted examinations to detect possible competition-related injuries. In an emergency, the experienced anaesthesiologist and emergency physician could have provided first aid. Two other aspects related to safety: During the dives, Daniel was always connected to a guide line via a lanyard. Additionally, two safety freedivers alternated multiple times during the 13 h to secure the athlete to approximately 10 m depth each time.
Measurements
During the 15-min breaks, the core body temperature was measured using infrared thermometry over the tympanic membrane. Additionally, the transcutaneous oxygen partial pressure (tcpO2) (TINA 4, Radiometer, Copenhagen; DK), tissue perfusion at depths of 3 and 7 mm (O2C, LEA Medizintechnik Giessen, DE), and non-invasive blood pressure were measured. Oxygen saturation (SO2) and perfusion index (PI) were recorded using pulse oximetry, 3-channel ECG signal, heart rate, and non-invasive blood pressure were displayed on a standard monitor (Life Scope, BSM 6501, Nihon Kohden, JPN).
Calculations
Cardiac output. A non-invasive continuous cardiac output (CCO) measurement method relies on the SpO2 pulse contour analysis coupled with pulse wave transit time (PWTT). In this approach, PWTT is determined as the interval between the R-wave of the ECG and the minimum of the SpO2 waveform [3].
Results
Two weeks prior to the competition, the biometric measurements of the Berlin athlete were as follows: Total lung capacity: 6.6 L, vital capacity at 5.1 L, and residual volume 1.5 L. Additionally, the calculated Tiffeneau index equalled 85%. The ECG showed sinus rhythm and a resting heart rate of 63 min-1. During a stress ECG, 99% of the target heart rate (HR) of 180 min-1 was reached, followed by a normal recovery. This value corresponds to a maximal V̇O2 of 30 - 35 ml/min/kg, or 2.24 L/min. With these values, a good muscular performance of 260 W was determined. Thus, Daniel's performance level was at 140%.
During the spiroergometry, at a HR of 72 min-1, the V̇O2 was measured at 340 ml/min, and at 93 min-1, the V̇O2 had increased to 870 ml/min. The V̇O2max was determined to be 2.58 l/min.
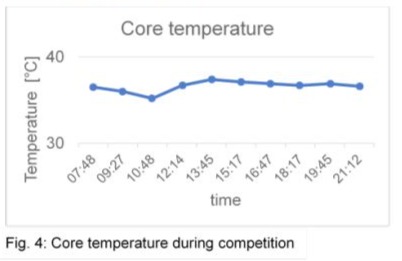
Core temperature
The core temperature measured through the ear canal remained constant at an average of 36.8°C, with one exception at 35.2°C early during the competition (Figure 4).
Transcutaneous pO2
As a result of repeatedly increased ambient pressure, the tcpO2 initially rose from 83 mmHg to 163 mmHg, then stabilized, remaining relatively unchanged with an average of 130 mmHg throughout the subsequent course (Figure 5).

Perfusion index and relative subcutaneous microcirculation
At the beginning of the competition, the perfusion index (PI) was 7.04, then significantly decreased to 0.85, and with 1.08 remained essentially unchanged until the end of the competition.
The relative blood flow at a depth of 3 mm (202 arbitrary units; a.u.) was slightly greater than at a depth of 7 mm (177 a.u.) at the beginning of the measurement. During the competition, significant reductions in subcutaneous microcirculation occurred, paralleling the changes in the PI, reaching approximately 25% of the baseline values (Figure 6).

Oxygen saturation
The superficial (3 mm) tissue oxygen saturation (SO2) in the post-capillary perfusion area was significantly reduced during the competition compared to the baseline (p<0.05, t-test), reaching baseline values shortly after the end of the competition. Between the 100th dive and the 150th dive, the superficial SO2 increased above the SO2 in deeper tissue layers (7 mm), indicating thermogenic regulation.
The decrease in SO2 in the post-capillary venous perfusion area indicated hydrostatic vasocompression, which was caused by the decrease in haemoglobin amount.
The amount of haemoglobin in the deep tissue layers increased between the 150th and the 200th dive, only to subsequently decrease. After the end of the competition, the baseline value was practically reached again (Figure 7).

Cardiovascular system
Arterial blood pressure
Bevor the competition, arterial blood pressures were relatively high at 147/86 mmHg and initially increased by up to 15%. Subsequently, they moderately decreased, so that by the end, the pressures were nearly identical to those at the beginning. Although they were slightly elevated on average due to physical exertion, at 140/94 mmHg, they were within the range of values measured beforehand, lying between Daniel's resting values (110/85 mmHg) and his values at maximal exertion (200/80 mmHg) (Figure 8).

Heart rate during apnea dive
The HR measured with the sports watch increased immediately after diving and remained elevated shortly after surfacing. During the surface interval, it returned to the baseline level (Figure 9).

Example: In the 1st block of 25 dives, HR during dive 1 ranged between 90 at the surface and 115 min-1 on the bottom. These values remained nearly unchanged during dive 25, with 92 and 110 min-1, respectively (Figure 10, left). In block 9, approximately after 12.5 h of competition, during dives 200 and 222, surface HR had decreased to 80 min-1 and had on the bottom increased to 120 min-1 during the dives Figure 10, right).

Heart rate during competition, stroke volume, and cardiac output
HR at the beginning of the competition was 97 min-1. As the competition progressed, HR decreased and fluctuated around 75 min-1 (Figure 11, top).
The stroke volume was calculated from the calculated cardiac output and HR. Since these two measures had an almost parallel course, the stroke volume changed only slightly during the course of the competition and was 91 ml at the beginning and 101 ml at the end of the competition (Figure 11, middle).
The pulse wave transit time (PWTT) only insignificantly varied during the competition. The calculated cardiac output was thus increased in parallel with the HR at the beginning (9 L/min) and was decreased by 22% (7 L/min) at the end of the competition (Figure 11, bottom).

Lung
The predetermined total lung capacity was 6.6 L. The vital capacity remained nearly unchanged before and after the competition, at 5.1 versus 4.9 L. In addition to this static measure, the FEV1, as a dynamic measure, was only slightly reduced (4.1 L versus 3.9 L). The maximum expiratory flow rate after the competition was even significantly above the target value of 8.8 L/s, at 9.1 L/s.
Discussion
This detailed case report on a world record in free-dive Everesting begins by presenting the unique characteristics of the world record holder. Subsequently, a series of physiological data collected before, during, and after the competition follows, addressing the current gap in data for long-duration free-dive competitions. Given that high-performance sports inherently involve risks, this report also delves into this aspect, particularly focusing on barotrauma and decompression sickness.
The most important message of this case report is that the athlete successfully completed the competition without any dive-related injuries or issues, thanks to his personal qualities and meticulous preparation.
Personal qualities
Daniel's physical qualities for a world record attempt were described during a comprehensive diving medical examination at the beginning of 2024 as follows: age- and weight-related very good muscular performance (3.8 W/kg), very good cardiac adaptation, and normal recovery course.
Preparations
Preparation for the world record involved two aspects: endurance performance and handling apnea.
Endurance: The athlete commenced endurance training in September 2023. Over the course of four months, he dedicated himself to enhancing his fundamental fitness level through consistent swimming and apnea-diving sessions (3 h / week), alongside enduring several-hour rides on the racing bike. Significant achievements included a notably low resting heart rate (HR) (62 min-1) and achieving maximum physical performance at 140% of the target value. Furthermore, his body fat percentage stood at a mere 20% of his total body weight, reflecting Daniel's lean physique.
Daniel's low HR can also be explained, at least in part, by yoga. Although he did not regularly practice breathing techniques and meditation for four months, he incorporated the "Five Tibetans" as a mini yoga and morning routine [4].
Preparations also included test dives. It started with 50 dives at the Dive4Live pool. Later, 100 dives were completed, and even later, 150. The same protocol as for the world record attempt was always followed after 25 apnea dives, a longer break on dry land was scheduled. During these breaks, photos of Daniel's skin were taken to detect possible marbling, which could indicate a mild form of DCS: neither did the skin itch nor did it show marbling.
Apnea: Nutrition is also part of the preparation in the apnea world. Those who eat a lot need a lot of oxygen for metabolism. Eating less means less oxygen is consumed. Therefore, the ambitious athlete fasts before an apnea competition. Some athletes even start fasting long before the competition. Advantage: reduced V̇O2 due to decreased energy metabolism. Disadvantage: lower heat production. Result: Feeling cold even in summery temperatures. However, up to 10% lower V̇O2 at 1°C lower temperature [5].
Daniel naturally paid attention to his diet. He also knew that among fats, proteins, and carbohydrates, the latter are burned most efficiently. Therefore, although he did not strictly follow a diet, he focused on complex carbohydrates. Sugar and sweets (simple sugars) were avoided because they only provide energy very briefly, causing fluctuations in blood sugar levels.
Physiological variables over time course
Core temperature regulation is critical, as exposure to cold conditions can impact various physiological and cognitive functions. Studies have shown that cold environments can decrease muscle strength [6], impair cognitive performance [7], and affect hand motor function [8].
One former study highlights the efficacy of wearing a 2-3 mm wet suit in providing sufficient thermal protection for trained young males [9]. While 7-mm neoprene suits will offer enhanced insulation, they may also constrain the diver's flexibility, especially during 222 times complex maneuvers.
In light of these considerations, Daniel’s choice of a 5-mm wet suit represents a prudent compromise. This decision effectively balanced thermal insulation while preserving the diver's mobility, resulting in minimal fluctuations in core temperature throughout the entire competition.
The tissue perfusion (relative flow) measured by tissue spectrometry in both the subcutaneous (3 mm depth) and muscular (7 mm depth) tissue was reduced from the start of the competition until the end of the competition.
Since the measurements were taken quickly after 25 dives but not directly during the dive, the determination of tissue perfusion is a valid parameter of the effects of repeated apnea diving.
Pulse oximetry provides valuable information with O2 saturation (SO2) and the perfusion index (PI) in all situations in which hypoxic conditions are feared [10]. Both variables had decreased after the start of the competition, but remained constant as the competition progressed. However, the lowest PI value achieved during the competition was 0.85, which was clearly within a described reference range (0.3 to 10.0) [11].
The transcutaneous partial pressure of oxygen (tcpO2), which was measured at the ball of the hand, i.e. a representative, peripheral current area, can be used to determine the proportion of dissolved oxygen and can therefore be used to determine the partial pressures of a gas mixture (Dalton's law). Once the partial pressures of the gas mixture of the breathing air were known, the tcpO2 allowed direct conclusions to be drawn about the pN2.
As the tcpO2 remained elevated over the entire duration of the competition, N2 saturation could not have occurred during the 222 apnea dives. The ratio of three to one for the length of the surface interval compared to the apnea duration was therefore a correct decision. The 15-minute pause 'on the dry' also helped to reduce any N2 load that may have occurred.
The normobaric tcpO2 fluctuates between 50 and 90 mmHg [12]. The increased tcpO2 value after the start of the competition indicates that the oxygen physically dissolved in the tissue had increased. If SO2 does not decrease further during the competition, it means that O2 supply and O2 consumption have reached an equilibrium, which was made possible by the physically dissolved oxygen. In other words, a portion of the dissolved oxygen is sufficient to meet a substantial portion of the O2 demand in the present apnea dives, even though the microcirculation is restricted and the precapillary blood contains less haemoglobin bound oxygen.
Arterial blood pressure
Chronic arterial blood pressures of 150/90 mmHg are typically indicative of mild hypertension. In this context, the acutely elevated pressures can be attributed to the impending competition. The stability of this variable throughout the competition, alongside other cardiovascular parameters, indicates a harmonious equilibrium between physical exertion and the cardiovascular system, which was consistently maintained during the event.
Heart rate during dives
Shortly after immersion, the diving response typically triggers a reduction in HR, known as diving bradycardia [13]. This bradycardia persists as long as the diver remains at rest. However, in Daniel's case, the demanding nature of his dive, involving maneuvers such as diving actively headfirst from the surface and resurfacing actively, executing roll terms, and finning, resulted in increased physical activity that overlapped with the diving response.
Initially, a ‘resting’ HR of 90 min-1 was established at the surface to increase upon descending to 115 min-1 at the bottom during the first dives. Remarkably, these values remained relatively stable even after 13 h of competition. Towards the end of the competition, surface HR had decreased to 80 min-1, while bottom HR had increased to 120 min-1.
These 222 fluctuations in HR lasting approximately only 45 s, illustrate the efficient functioning of the autonomic nervous system and the heart's ability to adapt to changes in demand, reflecting a robust cardiovascular response.
Heart rate during competition
Daniel's resting HR ranges between 50 and 60 min-1. At the beginning of the competition, his HR was relatively high for an endurance-trained athlete, at 97 min-1, but this can be well explained by the central innervation before the start of a competition [14]. As the competition progressed, his HR decreased and settled around 75 min-1 (Figure x, above).
Both the HRs during the single dives and throughout the competition remain well within physiological values, especially considering that the athlete reaches a HR of 170 min-1 at maximum exertion.
Cardiac output
Several minimally invasive methods for measuring cardiac output (CO) have been developed as alternatives to thermodilution with pulmonary artery catheterization. One such alternative is the estimated continuous CO (esCCO) method which has been shown to reliably track directional changes in CO [3] and exhibit strong correlation with echocardiography data for measuring CO [15].
In this study, the esCCO method provided reasonable values for actual CO, which closely paralleled changes in HR. For instance, at the beginning of the competition, both CO and HR were relatively high and both decreased over the course of the competition. This suggests that the repetitive immersions, coupled with blood shifting into the thorax, had no apparent negative effect on pulmonary circulation, particularly on the right ventricle, and did not induce diving-induced oedema [16].
A note on stroke volume should be added. Our calculations based on CO and HR revealed relatively high values of approximately 90 mL. Indeed, such values can occur when considering the increased intrathoracic blood volume after immersion, which can lead to enlarged ventricular filling [17].
Physical Exertion
During the apnea dives, an average HR of 93 min-1 was recorded, with a predetermined V̇O2 of 870 ml/min at this HR. By calculating the V̇O2 for the 45-s dive, it was determined to be 680 ml/min, indicating a moderate physical exertion of approximately 2.5 METs, equivalent to 70 W.
This level of exertion comfortably resides within the scope of oxidative metabolism, mitigating the risk of acidosis.
For comparison: In cycling Everesting competitions, athletes typically expend more than 8,000 kJ over an average duration of 12:25 h, achieving a mean power output of almost 200 W.
Barotrauma
Ears. Approximately half of all scuba divers have experienced barotrauma of the ears, with about one-third encountering barotrauma of the paranasal sinuses [18]. Specifically, barotrauma of the middle ear stands out as the most prevalent type among divers, posing a significant threat to dive safety [19]. While inner ear barotraumas are also noteworthy, they are comparatively less frequent [20].
Nevertheless, breath-hold divers who experience inner ear barotrauma due to diving to depths of 10 m require immediate treatment [21]. These incidents are likely attributable to the initial failure of pressure equalization during rapid descents. In cases where equalization is forcefully attempted, a substantial pressure wave can impact the middle ear, potentially leading to the rupture of one of its two windows [22].
To mitigate such risks, Daniel employed proactive measures, such as performing the Frenzel manoeuvre, equalizing pressure 13 times during his descents to 20 m. Thus, he executed this manoeuvre almost 3,000 times during his descents, demonstrating a commitment to safety.
Lungs. The increasing ambient pressures pose a significant challenge to breath-hold deep divers due to the limited flexibility of the thorax, which inhibits the required deformation as per Boyle-Mariotte's law. Consequently, negative-pressure pulmonary barotrauma, commonly known as lung squeeze, often manifests with acute haemoptysis following dives to considerable depths [23,24]. In addition, research indicates that breath-hold dives to 20 m with expanded lung volumes can impede venous return and consequently CO [25], which also applies to glossopharyngeal insufflation (=lung packing) [26].
In the case of our athlete in this report, his total lung capacity (TLC) measured 6.6 L, with a residual volume (RV) of 1.5 L. Applying Boyle and Mariotte's law, Daniel's TLC would theoretically compress to 2.2 L at the depth of 20 m, still above his RV. However, Daniel only inhaled approximately 60% of his vital capacity (VC), meaning he added only 4.1 L to the 1.5-L RV, resulting in a volume of 5.6 L which at 20 m depth is equivalent to 1.9 L, still surpassing his RV.
In essence, by inhaling only 60% of his VC, Daniel effectively regulated his breathwork, maintaining venous return largely unaffected and averting the risk of pulmonary barotrauma.
Decompression sickness
Nearly 60 years ago, Paulev reported entirely unexpected cases of decompression sickness following breath-hold diving [27]. Much later, DCS has been reported to occur for the Japanese pearl divers (Amas) after repetitive dives to shallow waters [28]. In an even older review, Amas were also mentioned alongside with competitive breath-hold divers and underwater fishermen [24]. In that latter article, relations between depths and durations of dives and the length of surface intervals were presented. At that point in time, breath-hold divers were seemingly at risk to undergo a DCS, in case the surface interval was shorter than twice of the breath-hold dive duration.
The ratio of 1 to 3 between apnea duration and surface interval and used by our athlete is derived from a comprehensive apnea textbook authored by Natalia Molchanova [29]. Renowned for her exceptional abilities and commitment to safety, Molchanova amassed an impressive record of 41 world records and 23 gold medals throughout her illustrious career as an apnea icon. However, tragedy struck during a routine practice dive to a depth of 35 m near Formentera Island (ES), where she disappeared beneath the waves, this time without the security of a guide line and lanyard.
Presumably, fast tissues became partially saturated initially during the 45-s breath-hold dive presented, but had sufficient time to desaturate during the 2:15-min surface interval. The absence of DCS symptoms during the preparatory dives, including those indicative of mild DCS, and the lack of any DCS symptoms even long after the end of the competition, suggest that the slow tissues were not oversaturated either.
Concluding remarks
In the apnea diving scene, numerous world records have been set across various disciplines, including static and dynamic apnea both in lakes and open seas. This case highlights a remarkable world record for repetitive apnea dives (222 times at 20 m depth), totalling nearly 13 hours of competition. Notably, extensive measurements were conducted and permitted to demonstrate that the heart can adjust its rate from 80 min-1 at the surface to 120 min-1 at depth during a 45-s apnea dive, effectively overriding the diving response. Additionally, during the 15-min breaks after every 25 dives, although oxygen supply to deeper tissues was reduced, it appeared compensated by increased physically dissolved oxygen. Another impressive finding – also presented for the first time is the well-preserved circulatory system despite significant blood shifts into the thoracic cavity during each of the 25 consecutive dives. Despite variable filling of pulmonary vessels and atria, arterial pressures and heart rate remained largely constant, and the estimated cardiac output via pulse wave velocity even decreased throughout the competition. The absence of barotrauma to the ears and lungs on one hand, and decompression injuries on the other, is particularly noteworthy because both professional apnea divers like Amas and Haenyos, as well as apnea underwater hunters, can align their diving behaviour with the findings presented here.
Epilog
One might ask the question what drives people to endure as long as possible on a pole or to eat as many hot dogs as they can in 10 min. Water-affine individuals crawl as fast as possible through the English Channel, while others swim breath-holding as far as possible beneath ice. Daniel chose to attempt a world record in Free dive-Everesting. He succeeded and remained healthy.
How did he manage to complete 222 dives to 20 m and resurface in 13 h without any apparent damage? One answer is that he carefully considered every aspect of this unusual competition as part of a larger project. This includes physical fitness as well as mental preparation, both of which were meticulously cultivated beforehand. The planning of the entire competition and on-site organization at Dive4Life were nearly perfect, and extensive safety measures were in place. However, none of these five aspects would have led to success without one crucial factor: remarkable endurance to dive 222 times. The authors firmly believe that the absence of any of these aspects would have prevented success or even would have resulted in an accident. And: Increasing self-esteem could be a reasonable answer to the above question.
References
- No author listed. (2024, January 26). Everesting. Wikipedia.
- Meyer M. F, Knezic K, Jansen S, Klünter H. D, Pracht E. D, et al (2020). Effects of freediving on middle ear and eustachian tube function. Diving and Hyperbaric Medicine, 50: 350–355.
- Yamada T, Tsutsui M, Sugo Y, Sato T, Akazawa T, et al (2012). Multicenter Study Verifying a Method of Noninvasive Continuous Cardiac Output Measurement Using Pulse Wave Transit Time: A Comparison with Intermittent Bolus Thermodilution Cardiac Output. Anesthesia & Analgesia, 115: 82–87.
- Kilham C. (2011). The five Tibetans: Five dynamic exercises for health, energy, and personal power. Healing Arts Press.
- Jorjani P, & Ozturk S. S. (1999). Effects of cell density and temperature on oxygen consumption rate for different mammalian cell lines. Biotechnology and Bioengineering, 64: 349–356.
- Bergh, U, & Ekblom, B. (1979). Physical performance and peak aerobic power at different body temperatures. Journal of Applied Physiology, 46: 885–889.
- Davis F. M, Baddeley A. D, & Hancock T. R. (1975). Diver performance: The effect of cold. Undersea Biomedical Research, 2: 195–213.
- Clark R. E. (1961). The limiting hand skin temperature for unaffected manual performance in the cold. Journal of Applied Psychology, 45: 193–194.
- Ofir D, Yanir Y, Eynan M, & Arieli Y. (2019). Evaluating the thermal protection provided by a 23 mm wet suit during fin diving in shallow water with a temperature of 1620 degrees C. Diving and Hyperbaric Medicine, 49: 266–275.
- Li S, Zhang M, Long X, & Wang X. (2022). Relative perfusion index: An objective, quantitative and noninvasive method for evaluating the severity of keloids. Lasers in Surgery and Medicine, 54: 1071–1081.
- Lima P. A, Beelen P, & Bakker J. (2002). Use of a peripheral perfusion index derived from the pulse oximetry signal as a noninvasive indicator of perfusion: Critical Care Medicine, 30: 1210–1213.
- Ercengiz, A, & Mutluoglu, M. (2019). Hyperbaric, Transcutaneous Oximetry. In StatPearls. StatPearls Publishing.
- Elia, A, Gennser, M, Harlow, P. S, & Lees, M. J. (2021). Physiology, pathophysiology and (mal)adaptations to chronic apnoeic training: A state-of-the-art review. European Journal of Applied Physiology, 121:1543–1566.
- Gaehtgens, P. (1994). Das Kreislaufsystem. In Lehrbuch der Physiologie (pp. 135–181). Georg Thieme Verlag.
- Feissel M, Aho L. S, Georgiev S, Tapponnier R, Badie J, et al (2015). Pulse Wave Transit Time Measurements of Cardiac Output in Septic Shock Patients: A Comparison of the Estimated Continuous Cardiac Output System with Transthoracic Echocardiography. PLOS ONE, 10: e0130489.
- Bove, F. (1996). Cardiovascular problems and diving. SPUMS Journal, 26: 178–186.
- Ferrigno M, Hickey D. D, Liner M. H, & Lundgren C. E. (1986). Cardiac performance in humans during breath holding. Journal of Applied Physiology (Bethesda, Md.: 1985), 60:1871–1877.
- Schipke, J. D, Cleveland, S, & Drees, M. (2018). Sphenoid sinus barotrauma in diving: Case series and review of the literature. Research in Sports Medicine (Print), 26: 124–137.
- Lindfors O. H, Räisänen-Sokolowski A. K, Suvilehto J, & Sinkkonen S. T. (2021). Middle ear barotrauma in diving. Diving and Hyperbaric Medicine, 51:44–52.
- Azizi M. H. (2011). Ear disorders in scuba divers. The International Journal of Occupational and Environmental Medicine, 2: 20–26.
- Kreso A, & Grdinić B. (1992). [Inner ear injuries in breath-holding divers]. Lijecnicki Vjesnik, 114(9–12), 251–253.
- Scarpa A, Ralli M, De Luca P, Gioacchini F. M, Cavaliere M, et al (2021). Inner Ear Disorders in SCUBA Divers: A Review. The Journal of International Advanced Otology, 17: 260–264.
- Kalemoglu M, & Keskin O. (2006). Hemoptysis and breath-holding diving. Military Medicine, 171: 606–607.
- Schipke J. D, Gams E, & Kallweit O. (2006). Decompression sickness following breath-hold diving. Research in Sports Medicine (Print), 14:163–178.
- Ferrigno M, Hickey D. D, Liner M. H, & Lundgren C. E. (1987). Simulated breath-hold diving to 20 meters: Cardiac performance in humans. Journal of Applied Physiology (Bethesda, Md.: 1985), 62: 2160–2167.
- Schipke J. D, Eichhorn L, Behm P, Cleveland S, Kelm M, et al (2019). Glossopharyngeal insufflation and kissing papillary muscles. Scandinavian Journal of Medicine & Science in Sports, 29: 299–304.
- Paulev, P. (1965). Decompression sickness following repeated breath-hold dives. Journal of Applied Physiology, 20: 1028–1031.
- Kohshi K, Tamaki H, Lemaître F, Morimatsu Y, Denoble P. J, et al (2021). Diving-related disorders in commercial breath-hold divers (Ama) of Japan. Diving and Hyperbaric Medicine Journal, 51:199–206.
- Molchanova N. (2021). Fundamentals of diving with breath holding. Educational and methodical manual on freediving Molchanova Natalia. Eurasia Express.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.