Case Report : Pneumomediastinum and Subcutaneous Emphysema Following Septorhinoplasty
by Hamad Mohammed Al Jaber, Hekmet Bugrein*, Mohamed Hamid, Sarah Mufid
PHI Group, PHI Medcare, Qatar
*Corresponding author: Hekmet Bugrein, PHI Group, PHI Medcare, Qatar
Received Date: 15 January 2025
Accepted Date: 20 January 2025
Published Date: 22 January 2025
Citation: Al Jaber HM, Hamid M, Bugrein H, Mufid S (2025) Case Report : Pneumomediastinum and Subcutaneous Emphysema Following Septorhinoplasty. J Surg 10: 11232 https://doi.org/10.29011/2575-9760.011232
Abstract
A 28 year-old male presented with h/o chronic nasal blockage and nasal deformity, underwent septorhinoplasty under general anesthesia. The surgery was uneventful, but on postoperative day one, the patient developed severe right-sided chest pain and difficulty breathing, accompanied by right axillary pain. Examination revealed weak breath sounds and reduced chest movement on the right side. Frontal CXR demonstrates streaky linear lucencies in the superior mediastinum tracking down the mediastinal borders bilaterally consistent with pneumomediastinum. Subcutaneuous emphysema and a small apical right pneumothorax are noted as well.This report discusses an unusual case of postoperative emphysema in a young male, emphasizing the importance of prompt recognition and management.
Keywords: Chest pain; Postoperative complications; Septorhino plasty,pneumomediastinum; Subcutaneousemphysema
Introduction
Septorhinoplasty is a commonly performed procedure for functional and cosmetic nasal corrections. While generally safe, complications can occur. This report discusses an unusual case of post septorhinoplasty Pneumomediastinum and subcutaneous emphysema, which are significant complications that can arise following surgical procedures. These conditions can present with various respiratory symptoms and require prompt diagnosis and management. Clinical History
A 28 year-old male, had a history of chronic nasal obstruction and a cosmetic nasal deformity, leading to the decision for an elective septorhinoplasty. His medical history was unremarkable, with no previous surgeries or significant comorbidities reported., underwent septorhinoplasty under general anesthesia. The surgery was uneventful, but on postoperative dayone, the patient developed severe right-sided chest pain and difficulty breathing, accompanied by right axillary pain. Examination revealed weak breath sounds and reduced chest movement on the right side [1-4].
Surgical Procedure
The septorhinoplasty was performed under general anesthesia. The surgical procedure includes: Infiltration Of Xylocaine Adrenaline (5 cc),Transcolumellar incision, elevation of flap, subperichondrial dissection of septum, deviation CD and AP. Rasping and excision of hump. excision of bony deformities, L strut septoplasty, Spreader Graft, Caudal Fixation Of The Septum, tip rhinoplasty Columellar Strut,supratip graft lateral osteotomy closure by vicryl rapid Nasal splint dressing, The procedure was straightforward, with no intraoperative complications. Postoperatively, the patient was monitored in the recovery room and subsequently discharged to the ward after stable observations.
Postoperative Course: On recovery room GC good vital signs stable on postoperative day one, the patient developed: moderate to Severe right axillary and right sided chest pain, Difficulty breathing, With Right axillary pain.Spo2 monitored and it was 96 % in room air .Respiratory rate: Elevated, Chest auscultation
revealed weak breath sounds on the right side, Reduced chest movement was noted on the right side, These clinical signs raised suspicion for possible respiratory complications.
Diagnostic Imaging
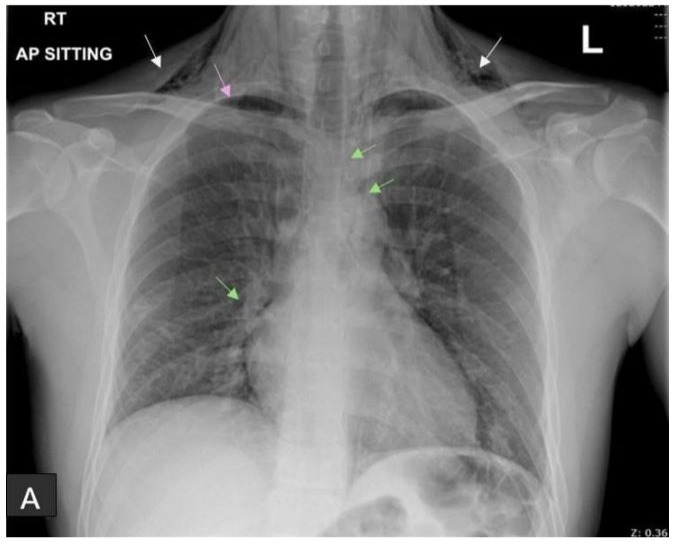
A frontal chest X-ray was obtained, which demonstrated: Streaky linear lucencies in the superior mediastinum tracking down the mediastinal borders bilaterally, indicative of pneumomediastinum.Subcutaneous emphysema noted in the cervical and upper thoracic regions. A small apical right pneumothorax.
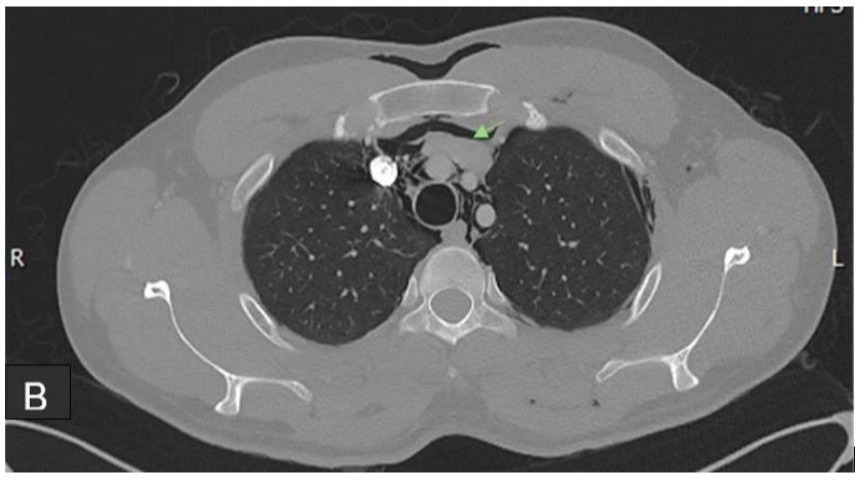
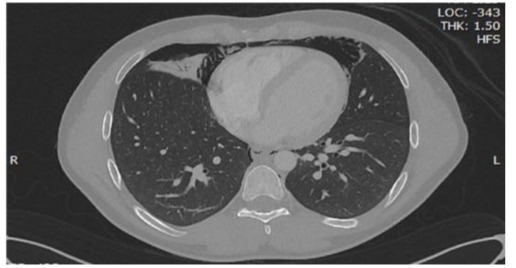
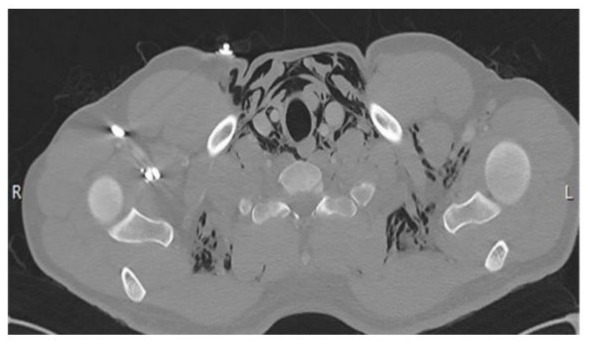
To further assess the extent of the air accumulation, a non-enhanced axial CT scan of the chest was performed: Non-Enhanced Axial CT of the Chest reveled:
Axialcuts of NECT chest demonstrate free air surrounding the major vessels , trachea and the heart, reveals extensive soft tissue emphysema with, small bilateral minimal pneumothorax is identified more right sided than left.

Thoracic aorta and its major branches appear fairly obesified with the contrast
Diagnosis
The findings from both imaging studies were consistent with:
- Pneumomediastinum
- Subcutaneous emphysema
- Small bilateral more right-sided pneumothorax.
Management
Given the patient’s stable hemodynamics and the small size of the pneumothorax, a conservative management approach was initiated, which included:
Oxygen Therapy: Supplemental oxygen was provided to improve oxygenation.
Monitoring: Continuous surveillance of vital signs and respiratory status was conducted.
Pain Management: Analgesics were prescribed to manage discomfort.
Observation: The patient was educated on potential symptoms of respiratory distress and was observed in the surgical ward.
Over the following days, the patient showed clinical improvement, with gradual resolution of chest pain and respiratory distress. Follow-up imaging was performed, showing a decrease in free air and improvement in lung expansion. The patient was discharged on postoperative day four, after achieving significant symptomatic relief and with improved imaging findings. He was given instructions for follow-up care and the need to report any return of respiratory symptoms.
Discussion
This case underscores the need for close postoperative care and thorough evaluation of respiratory symptoms in surgical patients, and early detection of relevant symptoms such as chest pain and dyspnea in the postoperative period is crucial for timely diagnosis and management. In most cases, conservative management is effective, as seen in this patient.
Conclusion
While septorhinoplasty is generally considered safe, rare complications such as postoperative Pneumomediastinum and subcutaneous emphysema can occur as rare complications. Surgeons and anesthesiologists should should maintain a high index of suspicion for respiratory complications in patients presenting with chest pain and dyspnea after nasal surgery ,Early detection through clinical examination and imaging, along with prompt and appropriate management, can lead to favorable outcomes.
Declaration of Conflictit of Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Acknowledgment: We would like to thank the PhiMedcare
Inpatient Clinical staff in high professional work and on centered patient care providing
References
- MostSP (2006) Analysisofoutcomesafterfunctionalrhinoplastyusinga disease-specific quality-oflife instrument. Arch Facial Plast Surg 8:306-309.
- Chiu CL, Ong GS (2000) Subcutaneous emphysema andpneumomediastinum after endotracheal anaesthesia.AnnAcad MedSingapore 29: 256-258.
- KennedyDW (1985) Functionalendoscopicsinussurgery:Technique.Archives of Otolaryngology - Head and Neck Surgery 111: 643-649.
- MimanMC,OzturanO,DurmusM,etal. (2001) Cervicalsubcutaneousemphysema:Anunusualcomplicationofadenotonsillectomy.PaediatrAnaesth 11: 491-493.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.