“Campaign Staggering” a Way to Bridge Resources Gaps in Supplemental Immunization Activities-Lagos State 2018 Measles Vaccination Campaign’s Experience
Chimaobi Ihebuzor 2# , Avuwa Joseph Oteri 1*# , Samuel Bawa 3 , Adejoke Oladele Kolawole 2 , Boubacar Dieng 4 , Anne Eudes Jean Baptiste 3 , Bolanle Orefejo 5 , Nneka Onwu 2
1 Nigeria Governors Forum, Abuja, Nigeria
2 National Primary Health Care Development Agency, Abuja, Nigeria
3 World Health Organization, Country Office, Abuja, Nigeria
4 Technical Assistance Consultant, Gavi, The Vaccine Alliance, Nigeria
5 UNICEF, Lagos Field Office, Nigeria
# These authors contributed equally to this work
*Corresponding author: Avuwa Joseph Oteri, Nigeria Governors Forum, Abuja, Nigeria
Received Date: 15 November, 2022
Accepted Date: 24 November, 2022
Published Date: 29 November, 2022
Citation: Ihebuzor C, Oteri AJ, Bawa S, Kolawole AO, Dieng B, et al. (2022) “Campaign Staggering” a Way to Bridge Resources Gaps in Supplemental Immunization Activities-Lagos State 2018 Measles Vaccination Campaign’s Experience. J Community Med Public Health 6: 270. DOI: https://doi.org/10.29011/2577-2228.100270
Abstract
Introduction: The availability of qualified Health Workers (HW) and Cold Chain Equipment (CCE) has been one of the major challenges faced in all countries implementing Supplemental Immunization Activities (SIAs) including Nigeria. This challenge has been found to contribute to the country’s inability to reach the set targets. This paper describes how Lagos state staggered its 2018 measles vaccination campaign to mitigate the resources gaps of health workers and cold chain equipment. It also highlights the effectiveness of staggering as it relates to campaign outcome, looking at the number of children reached during the campaign. Methods: The microplanning process was followed by a 2 (two) step verification of the states micro-plans. These processes helped Lagos state to identify gaps in qualified health workers and CCEs. Data was analyzed and presented using MS Excel and Statistical Package for Social Sciences version 20 (SPSS). Results: Findings showed inadequate health workers and CCEs across all LGAs in the state to implement the SIAs at the same time. A total of 8,948 health workers were required to reach the target population. For CCEs a total of 752 cold boxes, 9050 vaccine carriers, and 90,448 ice packs (0.3/0.4 & 0.6) were required. However, only 3,769 health workers, 640 cold boxes, 4985 vaccine carriers, and 56,971 icepacks (CCEs) were available for the 2018 MVC in the state. This left a gap of 44 cold boxes, 4065 vaccine carriers and 33477 ice-packs. Following the staggering of the campaign where the measles vaccination campaign was implemented in phases (phase 1 and phase 2), the shortfall was reduced. The outcome of the campaign in terms of the number of targeted children reached when compared to previous measles vaccination shows modest improvement. Conclusion: The staggering approach introduced by the National Measles Technical Coordinating Committee during the 2017/2018 measles vaccination campaign helped Lagos state in reducing the gap in required qualified health workers and CCE needed for a quality vaccination campaign. In the same vein, more children were reached in the 2018 measles vaccination campaign when compared to previous campaigns.
Keywords: Supplemental immunization activities; Staggering; Qualified health workers; Cold chain equipment
Introduction
The United Nations Sustainable Development Goals (SDGs), also known as Global goals were countries’ commitments toward the ending hunger, protecting the planet, and ensuring that by 2030 all people enjoy peace and prosperity. Reduction of measles mortality will contribute to the attainment of SDG3 which aims to end preventable deaths of newborns and children under 5 with all countries striving to reduce neonatal mortality to at least as low as 12 per 1,000 live births and under-5 mortality to at least as low as 25 per 1,000 live births amongst other indicators by 2030 [1,2].
Measles is one of the key contributors to child mortalities, especially in South Asia and Sub Saharan Africa [3]. The measles vaccine was among the antigens introduced in Nigeria’s Expanded Program on Immunization (EPI) schedule in 1979, and it is administered to children 9 months of age. Since then, coverage of the first dose of Measles Containing Vaccine (MCV1) through the routine immunization program has been fluctuating and also very suboptimal to provide the needed herd immunity to prevent its transmission among children [4].
The World Health Organization and United Nations Children Fund Estimates of National Immunization Coverage (WUENIC) for Nigeria from 2009 to 2017 for MCV1 coverage averaged 49.4% [5]. The National Immunization Cluster Survey (NICS) of 2016 - 2017 coverage for MCV1 prior to the 2017/2018 measles vaccination campaign was 42%. However, variation exists across zones and states with Lagos state having an average coverage of 88% in the 2016 - 2017 NICS [6]. It is worth noting that at the time the 2017/2018 measles vaccination campaign was carried out in Nigeria; was yet to introduce a measles second dose in her routine immunization schedule. Measles second dose has been shown to improve seroconversion for children, which ultimately takes care of primary vaccine failure [7]. The SIA that targeted a wider age group (9-59 months) offered the second dose opportunity to reduce the buildup of susceptible due to poor routine and primary vaccine failure.
As previously mentioned, persistently low MCV1 coverage and relatively low SIAs coverages in the measles follow-up campaigns (74% in 2013 and 84.5% in 2015) have resulted in a low population immunity profile that has allowed increased transmission of measles virus among children. The low immunity profile was the basis for the 2017/2018 nationwide measles mass vaccination campaign. Also of note is that as of 2017/2018 measles vaccination campaign, Nigeria had not introduced the measles second dose into her routine immunization schedule missing the opportunity of increasing the immunity of the children against the measles virus.
Nigeria adopted the WHO African Regional office 2011 measles elimination goal by the year 2020. One of the major targets in achieving the 2020 goal is the attainment of ≥ 95% coverage in MCV1 at National and subnational levels in both routine immunization and supplemental immunization activities. The approach comprised four key strategies of Supplemental Immunization Activities (SIAs) in the form of catch-up campaigns and follow-up campaigns, case-based surveillance for measles, and routine immunization as the core strategy. Measles outbreak response, measles case based management and vitamin A supplementation were also integrated into the key strategies [8,9].
The 2005/2006 nationwide catch-up campaign targeted 56 million eligible children aged 9 months through 14 years irrespective of vaccination status. This campaign was implemented in two phases; phase one covered the Northern states and was conducted in December 2005, while the second phase involving the Southern states was conducted in October 2006. Since then, Nigeria conducts nationwide follow-up campaigns every two or three years. All the country’s measles vaccination campaigns have adopted the same approach of implementing campaigns in two phases with states in each phase implementing the campaign across all Local Government Areas (LGAs) in the state at once irrespective of available resources.
Lessons learned from those SIAs have shown that implementing campaigns using this strategy did not achieve the desired goals as the teams are usually overstretched within the stipulated days thereby missing some of the targeted population. To implement a quality SIA, adequate human and materials resources – skilled health workers and Cold Chain Equipment (CCE) – are needed. The sub-optimal performance in the previous campaign was attributed to shortage of skilled health workers and inadequate CCEs [10].
To bridge this gap the country introduced innovative strategies in the 2017/18 MVC to improve the performance of states. One of these strategies was changing the two-phase National approach and increasing the number of streams of the campaign to regional levels [11]. At the state level, a staggering approach of the vaccination campaign was adopted in some states to take care of the resources gaps.
Staggering simply refers to the arrangement of events or activities to commence at different times. Staggering of the campaign was necessitated based on the available qualified health workers, cold chain available for implementation as well as human resources for monitoring and supervision of the campaign. Since the 2005/2006 catch-up campaign and the subsequent follow-up campaigns, the 2017/2018 follow-up campaign was the first that staggering was introduced at the state level.
This article describes how Lagos state staggered the implementation of the 2018 measles vaccination campaign and the impact it had on reaching more of the targeted children in the state. We also highlighted the effectiveness of this staggering approach by analyzing previous measles vaccination campaign results and that of the 2018 measles vaccination campaign that was staggered to fill resources gaps.
Methods
Study Setting
Lagos state is the commercial capital of Nigeria, and it is located in the southwestern part of the country. It shares boundaries with Ogun state at the North-East border, Benin Republic in the west, and the Atlantic Ocean in the South. It is a highly commercial town, it has a small landmass but has the highest urban population in Nigeria. Movement in and out of the city is constant as people live in the neighboring Ogun state yet work in Lagos state. Visitors from all over West Africa visit the states because of its commercial activities. According to the National Population Commission, in 2017 Lagos state had a projected population of 12,615,361 people [12]. The state targeted a total of 3,660,480 children 9 months to 59 months for the campaign.
2017/2018 Measles Vaccination Campaign
Microplanning Process
Immunization services be it routine services or the supplemental immunization activities requires a lot of planning to know the available resources – human, financial, storage space, as well as the demographic statistics of the recipients. For cost effectiveness of immunization, one must know the target population [13,14]. Microplanning is a bottom-up process of estimating the resources (human and material) needed for the successful implementation of any activity. The output of any SIA microplanning process should include the requirement and availability for data tools, qualified personnel and functional CCE to reach the target population. The micro plan document will identify the required, available and surplus or gaps of these resources at all levels for proper planning.
The micro-planning process in each ward was facilitated by a Ward Focal Person (WFP) in collaboration with all key stakeholders at the operational level. Micro plans were developed by all 245 implementing wards in the 20 LGAs in Lagos state to ascertain the number of children in the target population to be reached, and human, material and financial requirements for the campaign. Other outputs of the process include the list of settlements, health facilities, special places, Daily Implementation Plans (DIPs) including team movement to special places and settlements without vaccination posts., number of vaccination teams, number of vaccination posts, waste management plans. Identification and selection of vaccination posts is one of the key outputs of the microplanning process and it contributes to the success of the SIAs in general. The major aim of using vaccination posts is to ensure there is a conducive and easily accessible place for the vaccination exercise to take place. According to the 2017/2018 NPSIAs field guide, vaccination posts should be ≤ 1KM from the client. Some other key factors to consider when selecting a site to serve as a vaccination post are each settlement should have a vaccination post, shelter, free flow of clients and health workers. Vaccination posts are either fixed posts or temporary fixed posts. Fixed posts are posts where vaccination exercise will implemented for the entire duration of the campaign. Temporary fixed posts are vaccination posts were vaccinations would take place for a period depending on the target population in the catchment area.
To ensure good quality of the exercise, supervision was undertaken by the state/LGA teams using a paper-based checklist and Open Data Kit (ODK).
Micro-Plan Phase 1 Verification
Following the development of the micro-plans, the next step was the verification process, which was implemented in 2 phases for the micro-plans developed. Micro plan verification is an endprocess activity conducted in 2 phases after micro-plan data has been collated at the state level. Phase 1 of the verification is done at the ward level by the LGA and state verification team comprising government and partners. A random selection of 30% of the wards was conducted for the micro plan phase 1 verification process and all LGAs encompassing these wards were directly assessed by the state verification team comprising the state Government and partners present [15].
Micro-plan Phase 2 Verification
The standard micro-plan phase 2 verification process for the measles SIA required that after reviewing the phase 1 verified micro-plan at the National level, a team of two members of the National Measles Technical Coordinating Committee (NMTCC) is deployed to the state for phase 2 verification purposes and joint decision making on how to resolve the identified issues. Among those issues was deciding how the implementation will be handled by not doing business as usual. The phase 2 verification process used the WHO measles high-risk assessment tool correlated with the state findings during the phase 1 verification process in terms of challenges for choosing the two LGAs where to verify and the four facilities by LGA to go to and complete the process. The phase 2 verification process involves three stages [1] desk review of the microplanning templates, [2] field visit and [3] debriefing of the state policymakers [15]. Epe LGA and Surulere were selected accordingly using the measles high risk assessment tool.
Human resources required for a successful measles follow-up vaccination campaign
According to the 2017/2018 measles vaccination field guide, the estimated workload for a vaccination team is 175 and 125 per day in an urban and rural areas respectively with an average of 150 per team [16].
Cold chain equipment required for a successful measles followup vaccination campaign
The 2017/2018 measles vaccination field guide stipulates the basic minimum cold chain requirement for a successful campaign at the ward and vaccination team level. A ward should have a minimum of 2 cold boxes and each cold box requires 24 0.6 icepacks. For vaccine carriers, each vaccination team requires at least 2 vaccine carriers and 4 icepacks per vaccine carrier [16].
Development of Staggering Plan
Communication for staggering/implementation days
A very robust communication plan contributes to the success of any SIA from the planning to the implementation phase. There were several Advocacy, Communication, Social Mobilization (ACSM) activities implemented during the 2017/2018 measles SIA to sensitize, create demand and increase awareness among the population. During implementation, the town announcer of a vaccination team visited a catchment area on their Daily Implementation Plan (DIP) the evening before the visit of the vaccination team the following day. The visit was to inform clients/caregivers on the place and time of the visit from the vaccination team the following day. This information will also be communicated periodically during the implementation day to support the work of the H2H mobilizers so the staggering date is communicated to them.
National verifiers and the state team reviewed all the LGAs verified microplans for the measles vaccination campaign in the presence of all LGA team members. The microplan template was used to estimate the requirements by the state for the campaign including human resources and CCEs. We estimated the human resource and cold chain equipment required for the campaign in the state using the guidelines of the measles vaccination field guide. We then compared the required human resource and cold chain needs with what was available in the LGAs to identify gaps.
Based on the gaps identified, the LGAs were split into two phases (phase 1 and phase 2) to implement the campaign. LGAs in phase 1 were then paired with LGAs that implemented in phase 2 to support them with their human resources and CCEs to bridge the gaps. Ten LGAs implemented in the first phase while the remaining ten implemented in the second phase.
Quantitative data measure was used to estimate the human resources and cold chain equipment and the vaccination campaign outcome of the 2018 campaign in Lagos State. Data management and analysis were performed using spreadsheets and statistical applications such as MS Excel and Statistical Package for Social Sciences version 20 (SPSS). Simple frequency tables, Cross tabulations, charts and maps were used to present analysis outcomes.
Results
Staggering Plan
Lagos state adopted the inter LGA staggering after the assessment of the available resources (Health workers and CCEs) and the LGAs were paired to support each other during the two phases of the campaign in the state. Table 1 shows the pairing of the LGAs and the implementation days of the measles vaccination campaign. The staggering was discussed at the state level and all the LGA officials were told of the support they are either rendering or receiving from their paired LGAs. Health workers that provided support during the staggering are those licensed to give injection and they worked with the primary owners of the LGA who are conversant with the terrain and developed the daily implementation plans.
|
Phase 1 |
Phase 2 |
|
April 15 th to 22 nd 2018 |
April 22 nd to 29 th 2018 |
|
Agege |
Ifako-Ijaye |
|
Ageromi-Ifelodun |
Apapa |
|
Alimosho |
Ikeja |
|
Ojo |
Badagry |
|
Amuwo-Odofin |
Oshodi/Isolo |
|
Mushin |
Surulere |
|
Lagos Mainland |
Somolu |
|
Ikorodu |
Kosofe |
|
Lagos Island |
Eti-Osa |
|
Epe |
Ibeju Lekki |
Table 1: Pairing of LGAs with implementation dates by phases.
Assessment of fast cold chain equipment
Using the 2017/18 MVC operational field guide, we assessed the adequacy of CCEs in the state across all LGAs to implement the campaign. Following the microplanning process, data showed Lagos state had only 640 cold boxes, 4,985 vaccine carriers and 56,971 ice packs. Each cold box is expected to accommodate 24, 0.6-liter ice packs. Each vaccination team should have 2 vaccine carriers with 4, 0.3/0.4litere ice packs in each vaccine carrier leading to an estimated need of 9,050 vaccine carriers. 90, 448 icepacks were needed for the campaign for the cold boxes and vaccine carriers. 752 cold boxes based on a minimum requirement of 2 cold boxes per ward were needed for the campaign with 18,048, (0.6) liter ice packs (Table 2). However, only 640 cold boxes were available leaving a gap of 112 cold boxes. The state required 4,525 vaccination teams with an estimated 9,050 vaccine carriers (two vaccine carriers per team) needed for the campaign. However, only 4,985 vaccine carriers were available in the state leaving a shortfall of 4,065. On ice packs, 56,971 ice packs were available in the state out of the expected 90,448 icepacks needed for the campaign leaving a deficit of 33,477. The available CCEs, requirement and shortfalls are shown in Table 3.
|
LG As |
Target Population |
Required |
Available |
Shortfall |
Paired LGA |
Available for Paired LGA |
Total Available |
Shortfall After Pairing |
|
Phase One LGAs |
||||||||
|
Agege |
156,862 |
348 |
130 |
218 |
Ifako –Ijaiye |
102 |
232 |
116 |
|
Ajeromi - Ifelodun |
344,868 |
652 |
443 |
209 |
Apapa |
61 |
504 |
148 |
|
Alimosho |
435,421 |
916 |
432 |
484 |
Ikeja |
162 |
594 |
322 |
|
Ojo |
398,129 |
958 |
319 |
639 |
Badagry |
185 |
504 |
454 |
|
Amuwo – Odofin |
98,151 |
264 |
161 |
103 |
Oshodi/Isolo |
360 |
521 |
-257 |
|
Mushin |
284,263 |
616 |
300 |
316 |
Surulere |
100 |
400 |
216 |
|
Lagos Mainland |
110,452 |
296 |
120 |
176 |
Somolu |
151 |
271 |
25 |
|
Ikorodu |
381,129 |
716 |
215 |
501 |
Kosofe |
85 |
300 |
416 |
|
Lagos Island |
55,868 |
200 |
79 |
121 |
Eti- Osa |
95 |
174 |
26 |
|
Epe |
33,524 |
208 |
140 |
68 |
Ibeju Lekki |
87 |
227 |
-19 |
|
Phase Two LGAs |
||||||||
|
Ifako –Ijaiye |
148,781 |
456 |
102 |
354 |
Agege |
130 |
232 |
224 |
|
Apapa |
51,443 |
160 |
61 |
99 |
Ajeromi - Ifelodun |
443 |
504 |
-344 |
|
Ikeja |
115,962 |
316 |
162 |
154 |
Alimosho |
432 |
594 |
-278 |
|
Badagry |
201,649 |
464 |
185 |
279 |
Ojo |
319 |
504 |
-40 |
|
Oshodi/Isolo |
321,084 |
718 |
360 |
358 |
Amuwo – Odofin |
161 |
521 |
197 |
|
Surulere |
165,492 |
526 |
100 |
426 |
Mushin |
300 |
400 |
126 |
|
Somolu |
132,456 |
364 |
151 |
213 |
Lagos Mainland |
120 |
271 |
93 |
|
Kosofe |
120,824 |
360 |
85 |
275 |
Ikorodu |
215 |
300 |
60 |
|
Eti- Osa |
74,557 |
204 |
95 |
109 |
Lagos Island |
79 |
174 |
30 |
|
Ibeju Lekki |
29,565 |
206 |
87 |
119 |
Epe |
140 |
227 |
-21 |
Table 2: Lagos state HW requirements, available, shortfall, and available by LGAs and total number after pairing of LGAs.
|
G |
iostyles |
Cold Boxes (RCWs) |
Ice-Packs |
|||||||||||
|
LGA |
No of Teams |
No Of Wards |
Required Giostyle (2/ Team) |
Available Giostyle |
Giostyle Shortfall |
Rush Available |
RCW Required 2/ Ward |
RCW Available |
Gap |
Required (0.3/0.4 Icepack/Giostyle) 4 |
Rrequired (0.6 Ice-Pack/ RCW 24 |
Total Required |
Total Available |
Ice-Pack Shortfall |
|
Agege |
174 |
13 |
348 |
250 |
-98 |
26 |
30 |
4 |
2784 |
624 |
3408 |
869 |
-2539 |
|
|
Ajeromi/Ifelodun |
326 |
16 |
652 |
323 |
-329 |
32 |
16 |
-16 |
5216 |
768 |
5984 |
2633 |
-3351 |
|
|
Alimosho |
518 |
36 |
1036 |
448 |
-588 |
98 |
72 |
40 |
-32 |
8288 |
1728 |
10016 |
9977 |
-39 |
|
Amuwo Odofin |
132 |
14 |
264 |
100 |
-164 |
28 |
20 |
-8 |
2112 |
672 |
2784 |
1300 |
-1484 |
|
|
Apapa |
80 |
12 |
160 |
105 |
-55 |
24 |
21 |
-3 |
1280 |
576 |
1856 |
1569 |
-287 |
|
|
Badagry |
191 |
20 |
382 |
232 |
-150 |
195 |
40 |
40 |
0 |
3056 |
960 |
4016 |
3074 |
-942 |
|
Epe |
104 |
19 |
208 |
116 |
-92 |
38 |
43 |
5 |
1664 |
912 |
2576 |
2362 |
-214 |
|
|
Eti Osa |
102 |
20 |
204 |
132 |
-72 |
40 |
30 |
-10 |
1632 |
960 |
2592 |
1800 |
-792 |
|
|
Ibeju Lekki |
103 |
12 |
206 |
92 |
-114 |
24 |
19 |
-5 |
1648 |
576 |
2224 |
1270 |
-954 |
|
|
Ifako/Ijaye |
228 |
14 |
456 |
421 |
-35 |
28 |
30 |
2 |
3648 |
672 |
4320 |
4019 |
-301 |
|
|
Ikeja |
158 |
18 |
316 |
411 |
95 |
36 |
22 |
-14 |
2528 |
864 |
3392 |
2556 |
-836 |
|
|
Ikorodu |
358 |
30 |
716 |
421 |
-295 |
87 |
60 |
60 |
0 |
5728 |
1440 |
7168 |
1620 |
-5548 |
|
Kosofe |
180 |
21 |
360 |
297 |
-63 |
42 |
42 |
0 |
2880 |
1008 |
3888 |
4310 |
422 |
|
|
Lagos Island |
100 |
20 |
200 |
141 |
-59 |
40 |
32 |
-8 |
1600 |
960 |
2560 |
3844 |
1284 |
|
|
Lagos Mainland |
148 |
18 |
296 |
158 |
-138 |
36 |
32 |
-4 |
2368 |
864 |
3232 |
2440 |
-792 |
|
|
Mushin |
350 |
19 |
700 |
365 |
-335 |
38 |
25 |
-13 |
5600 |
912 |
6512 |
3128 |
-3384 |
|
|
Ojo |
489 |
15 |
978 |
285 |
-693 |
265 |
30 |
24 |
-6 |
7824 |
720 |
8544 |
2844 |
-5700 |
|
Oshodi/Isolo |
359 |
20 |
718 |
234 |
-484 |
40 |
35 |
-5 |
5744 |
960 |
6704 |
2160 |
-4544 |
|
|
Shomolu |
182 |
16 |
364 |
155 |
-209 |
32 |
32 |
0 |
2912 |
768 |
3680 |
3168 |
-512 |
|
|
Surulere |
243 |
23 |
486 |
299 |
-187 |
46 |
47 |
1 |
3888 |
1104 |
4992 |
2028 |
-2964 |
|
|
Total |
4525 |
376 |
9050 |
4985 |
-4065 |
645 |
752 |
640 |
-112 |
72400 |
18048 |
90448 |
56971 |
-33477 |
Table 3: Lagos state 2017/18 MVC Cold-chain equipment requirements, available and shortfall.
In summary, as shown in table 3, there were shortfalls in all fast CCE equipment required for the campaign across the LGAs in the state. For giostyle, 19/20 (95%) of the LGAs had inadequate vaccine carriers while 12/20 (60%) of the LGAs had shortfall in cold boxes and 18/20 (90%) LGAs had inadequate ice packs.
The staggering of the campaign and pairing of the LGAs helped to reduce the shortfall in CCE as shown in table 4. After pairing the LGAs, 14/20 (70%) LGAs had adequate or excess giostyle, 19/20 (95%) LGAs had adequate or excess cold boxes and 12/20 (60%) LGAs had excess icepacks. For LGAs that still had shortfall of CCEs after the pairing, the state, based on earlier staggering communication to the LGAs, moved CCEs from LGAs with excess to those LGAs. For example, Alimosho despite the support gotten from Ikeja LGA still received giostyle from Agege (a close LGA) to bridge their gap in cold boxes and icepacks.
Recycling of icepacks was jettisoned during the SIAs. To mitigate this problem the state and LGAs ensured regular supply of power (≥ 12 hours) in the LGA cold stores by providing funds for fueling of generator in addition to the power from the national grid. This ensured that there was adequate power supply for baking of ice packs as soon as the vaccination teams closed for the days’ work. Table 4 shows the Cold-chain equipment requirements, availability, shortfall, and available CCEs after pairing of LGAs.
|
LGA |
No of Teams |
No Of Wards |
No of HFs |
Required Giostyle (2/Team) |
Available Giostyle after pairing |
Giostyle Shortfall |
Rush Available |
RCW Required 2/ Ward |
RCW Available after pairing |
Gap |
Required (0.3/0.4 Ice-pack/ Giostyle) 4 |
Rrequired (0.6 IcePack/ RCW 24 |
Total Required |
Total Available |
Ice-Pack Shortfall |
|
PHASE 1 LGAs |
|||||||||||||||
|
Alimosho |
518 |
36 |
5 |
1036 |
779 |
-257 |
147 |
72 |
62 |
-10 |
8288 |
3456 |
11744 |
11277 |
-467 |
|
Ojo |
489 |
15 |
122 |
978 |
517 |
-461 |
30 |
64 |
34 |
7824 |
1440 |
9264 |
5918 |
-3346 |
|
|
Ikorodu |
358 |
30 |
3 |
716 |
718 |
2 |
60 |
60 |
0 |
5728 |
2880 |
8608 |
5930 |
-2678 |
|
|
Mushin |
350 |
19 |
13 |
700 |
664 |
-36 |
38 |
72 |
34 |
5600 |
1824 |
7424 |
5156 |
-2268 |
|
|
Ajeromi/ Ifelodun |
326 |
16 |
86 |
652 |
428 |
-224 |
10 |
32 |
37 |
5 |
5216 |
1536 |
6752 |
4202 |
-2550 |
|
Agege |
174 |
13 |
10 |
348 |
671 |
323 |
26 |
30 |
4 |
2784 |
1248 |
4032 |
4888 |
856 |
|
|
Lagos Mainland |
148 |
18 |
49 |
296 |
313 |
17 |
36 |
64 |
28 |
2368 |
1728 |
4096 |
5608 |
1512 |
|
|
Amuwo Odofin |
132 |
14 |
74 |
264 |
334 |
70 |
15 |
28 |
55 |
27 |
2112 |
1344 |
3456 |
3460 |
4 |
|
Epe |
104 |
19 |
18 |
208 |
208 |
0 |
6 |
38 |
43 |
5 |
1664 |
1824 |
3488 |
3632 |
144 |
|
Lagos Island |
100 |
20 |
41 |
200 |
273 |
73 |
40 |
62 |
22 |
1600 |
1920 |
3520 |
5644 |
2124 |
|
|
PHASE 2 LGAs |
|||||||||||||||
|
Oshodi/ Isolo |
359 |
20 |
130 |
718 |
334 |
-384 |
40 |
55 |
15 |
5744 |
1920 |
7664 |
3460 |
-4204 |
|
|
Surulere |
243 |
23 |
8 |
486 |
664 |
178 |
46 |
47 |
1 |
3888 |
2208 |
6096 |
5156 |
-940 |
|
|
Ifako/Ijaye |
228 |
14 |
79 |
456 |
671 |
215 |
28 |
30 |
2 |
3648 |
1344 |
4992 |
4888 |
-104 |
|
|
Badagry |
191 |
20 |
90 |
382 |
517 |
135 |
220 |
40 |
40 |
0 |
3056 |
1920 |
4976 |
5918 |
942 |
|
Shomolu |
182 |
16 |
42 |
364 |
313 |
-51 |
32 |
32 |
0 |
2912 |
1536 |
4448 |
5608 |
1160 |
|
|
Kosofe |
180 |
21 |
13 |
360 |
718 |
358 |
42 |
42 |
0 |
2880 |
2016 |
4896 |
5930 |
1034 |
|
|
Ikeja |
158 |
18 |
80 |
316 |
411 |
95 |
36 |
62 |
26 |
2528 |
1728 |
4256 |
11277 |
7021 |
|
|
Ibeju Lekki |
103 |
12 |
53 |
206 |
208 |
2 |
24 |
62 |
38 |
1648 |
1152 |
2800 |
3632 |
832 |
|
|
Eti Osa |
102 |
20 |
76 |
204 |
273 |
69 |
156 |
40 |
62 |
22 |
1632 |
1920 |
3552 |
5644 |
2092 |
|
Apapa |
80 |
12 |
615 |
160 |
428 |
268 |
64 |
24 |
37 |
13 |
1280 |
1152 |
2432 |
4202 |
1770 |
Table 4: Lagos state 2017/2018 MVC Cold chain equipment requirements, available and shortfall after pairing of LGAs.
Assessment of Human resources
The 2018 Lagos state measles vaccination campaign microplan estimated a total of 3,660,480 children aged 9 to 59 months to be reached during the campaign. A total of 4,474 vaccination teams over a 6-day period were needed to reach this population. This was arrived at using the work load expected per team per day taking into consideration the urban and rural wards in the state. A vaccination team is made up of 7 team members which include 2 health workers qualified to give injectables who serve as vaccinators. Other members of the vaccination team are; two recorders, one town announcer, one community leader that doubles as the crown controller and one house to house mobilizer.
We reviewed the human resource available in the state by identifying the number of health workers qualified to give injectables (doctors not included) in all Local Government Areas (LGAs) of the state. A total of 3,769 qualified health workers were identified across all 20 LGAs as available for the vaccination campaign. Lagos state unlike most of the states in Nigeria has the highest concentration of qualified health workers (nurses, midwives, community health officers and retired nurses/midwives). However, not all qualified health workers were deployed for the measles vaccination campaign as other services could not be shut down because of the campaign. For example, Mushin LGA that has the Lagos University Teaching Hospital (a tertiary health facility) has over a thousand nurses and midwives but only three hundred were available for the vaccination campaign. From the microplan data, a total of of five thousand, three hundred and ninety eight (5,398) qualified to give injectable health workers were identified across the 20 LGAs, but three thousand, seven hundred and sixtynine (3,769) were found to be available for the measles vaccination campaign. The state was expected to have 8,948 qualified health workers to reach its target population. This left the state with a gap of 5,179 health workers. Table 2 shows the required, available, shortfall and the total number of health workers available after pairing of LGAs in Lagos state. Ojo LGA despite the support from Badagry LGA still had the highest number of Human Resources for Health (HRH) gaps as well as Giostyle so did intra - LGA staggering, where all the available resources were deployed to finish the work in some wards before moving to the remaining wards during the phase one implementation.
The phase one LGAs with a target population of 2,298,667 required 5,174 health workers, 5,398 vaccine carriers, 400 cold boxes and 52,784 ice packs (0.3/0.4 and 0.6). The phase two LGAs had a target population of 1,361,813 required 3,774 health workers, 3652 vaccine carriers, 352 cold boxes and 37664 ice packs (0.3/0.4 and 0.6). The pairing of the LGAs ensured that there was adequate number of health workers to implement the campaign in each phase. However, despite the pairing of the LGAs, there was still a shortage of vaccine carriers.
In terms of the campaign outcome looking at the coverage, 19 of the 20 LGAs in Lagos state had an administrative coverage above 95%. One LGA (Apapa LGA) had 73%. The end process monitoring data however, revealed that all the 20 LGAs had coverages above the set target of 95%. These administrative and the end process monitoring coverage are illustrated in figure 6. The state also had a post-campaign coverage survey of 94%, which was the 9th best-performing state in the country.
Discussion
Nigeria has implemented several measles SIAs and one of the major challenges is the availability of qualified health personnel and CCEs to reach the huge target populations for these campaigns. In the 2017/2018 measles vaccination campaign, the National Primary Health Care Development Agency (NPHCDA) inaugurated the National Measles Technical Coordinating Committee (NMTCC) charged with the responsibility of coordinating and providing technical guidance to the states for a quality campaign. Having identified the gaps in HRH, CCEs, supervisors, and monitors, the campaign was changed from the normal two phases of National campaigns as done in the past into three phases (Figure 1). NMTCC is made up of government and Partner Agencies supporting immunization in the country. As the country got closer to the implementation dates, the resources gaps became more glaring based on the verification of the micro plans, and the country implemented the campaign in four streams (Figure 2) across geopolitical zones, against the initially planned three phases.
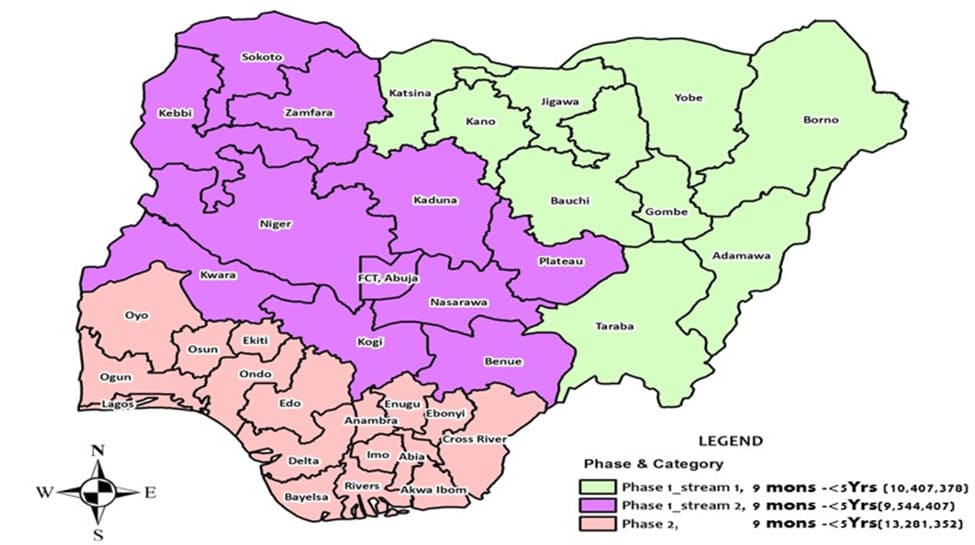
Figure 1: Proposed phasing of the 2017/2018 measles vaccination campaign in Nigeria.
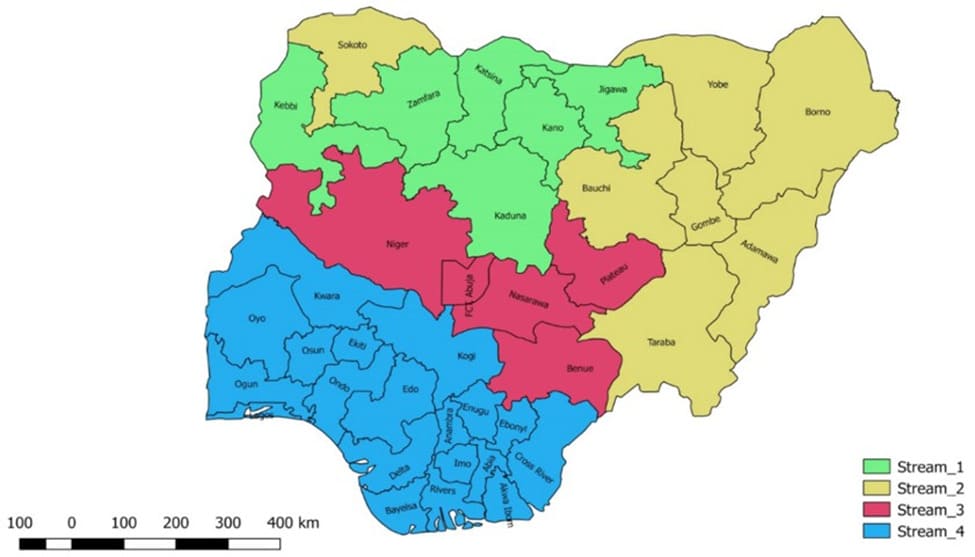
Figure 2: Final implemented streaming phases of the 2017/2018 measles vaccination campaign.
At the states level, NMTCC proposed a staggering approach to address shortfalls in resources. A menu of 3 types of staggering approaches was proposed to all the states and the states decided which of the staggering approaches was more appropriate for them at the end of the verification process with the National team at the state measles coordination committee debriefing meeting. The following staggering methods were proposed by the NMTCC for this campaign.
Zonal staggering: in this type of staggering approach, LGAs in the state are divided into two geopolitical zones looking at nearness in LGAs. Contiguous LGAs were clustered together or the geopolitical arrangement of the state was considered in the staggering plan. In some of the states, implementation of the campaign was done based on senatorial zones within the state. The selection of zones for the first phase is based on human resources and cold chain availability. Most of the time, the state team relocates to the implementing zone for ease of administration. This was done in Rivers and Kogi states as shown in figure 3.
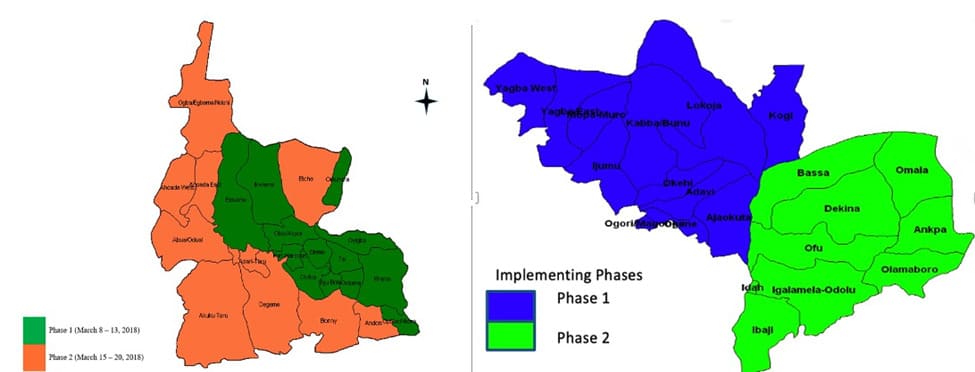
Figure 3: Inter LGA staggering by zone -Rivers state and Kogi state.
Intra-LGA Staggering: Wards within an LGA are selected to implement in the first phase, with factors such as cold chain, personnel, terrain, etc considered. With limited resources available, this form of staggering can be successfully implemented because the distance of travel is usually infinitesimal. This was done in Taraba state as shown in Figure 4.
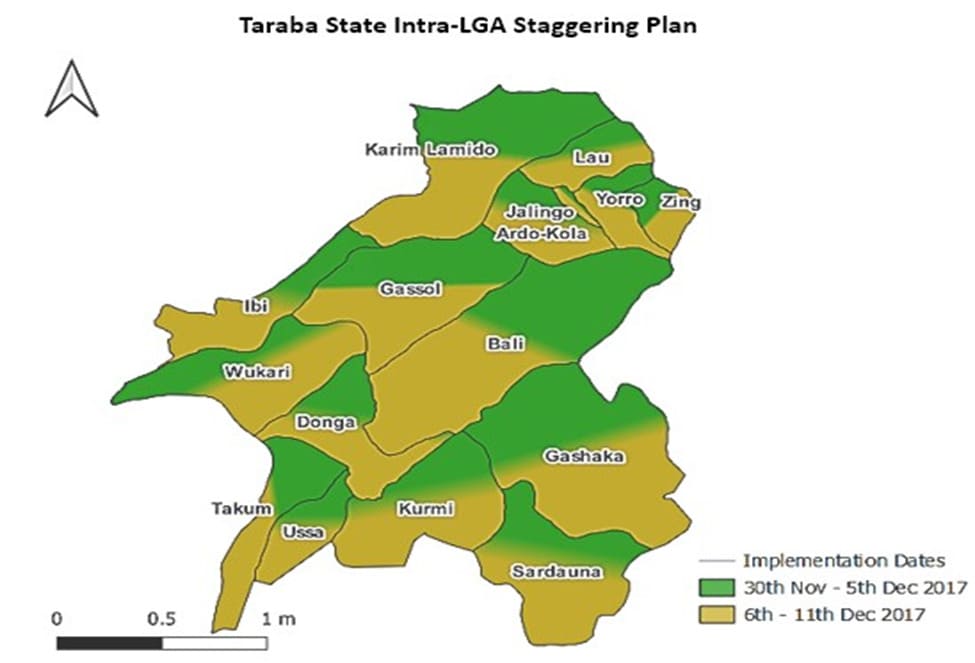
Figure 4: Intra LGA staggering for 2017/2018 Measles Vaccination Campaign as demonstrated by Taraba State.
Inter-LGA staggering: Selected LGAs in the state commence implementation during the first phase, there are several patterns of selecting the implementing LGA e.g. by zone, pairing, the population of LGAs or by terrain. This was demonstrated by Lagos and Oyo states as shown in figure 5.
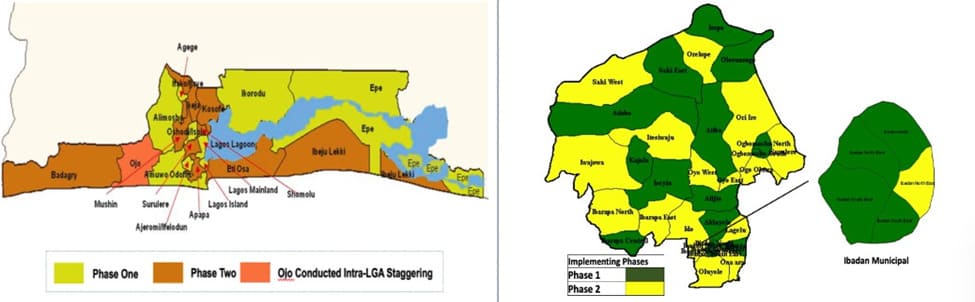
Figure 5: Inter LGA staggering by terrain/population Lagos and the Oyo States.
Using the lessons learnt from the concluded three streams of campaigns in the Northern part of the country as shown in figure 2, Lagos state implemented the campaign using the national guidelines by adopting the inter LGA staggering in (19/20) LGAs while one LGA (1/20) namely Ojo implemented using Intra LGA staggering because of the huge shortfall in human resources after adding the support from Badagry LGA. The staggering was important in Lagos state considering it as the most populous state in the country and its dynamics.
We found out that Lagos state could not have been able to reach the microplan estimate of 3,660,480 children targeted for the 2018 campaign within the stipulated time if there was no staggering of the campaign. The staggering of the campaign helped to minimize the human and cold chain equipment gaps.
Functional cold chain availability is the bedrock for any immunization activity. The needs become more in immunization campaigns as more storage is needed for the extra supplies encountered during SIAs. The observed cold chain equipment shortages in Lagos were not peculiar to Lagos alone as the 2017 Effective Vaccine Management Assessment report shows that storage capacity at local government and service delivery points were 70% and 59% respectively of the required capacity [17]. Similarly, in Ojo et al 2015 assessment of Challenges in the Logistics Management of Vaccine Cold Chain System in Ile-Ife, Osun State, Nigeria, only 45.7% of the required cold boxes in assessed facilities in the LGAs were functional [18] (Figure 6).
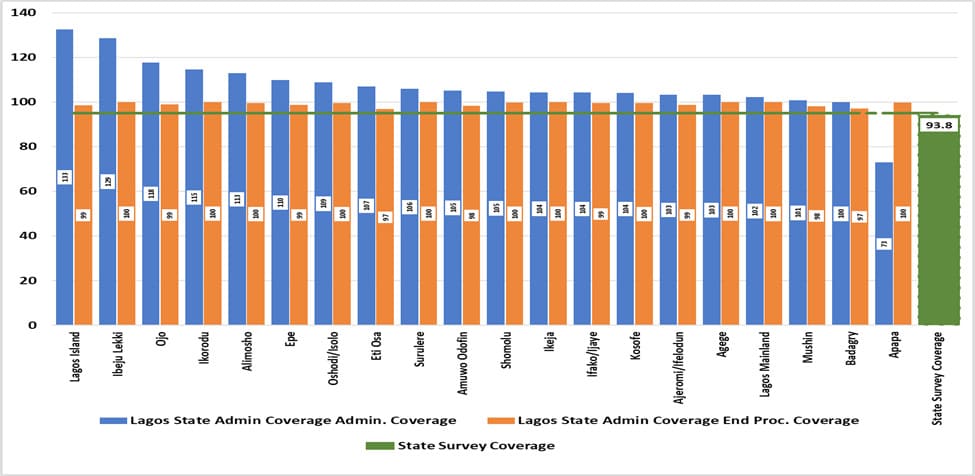
Figure 6: Lagos State 2018 MVC Admin. Coverage, End Process, and Survey Coverage Result, Lagos State 2018 MVC.
Health workforce is one of the six WHO health system building blocks necessary for good health outcomes. Service delivery is affected when there is shortage in the human resources for health. This is more noticeable in immunization campaigns where all hands are mobilized to attain the desired goal and in this case coverage of ≥95% in the post campaign coverage survey. From our findings, the shortage in the human resources needed for the measles vaccination campaign in Lagos could have made it impossible to carry out an effective vaccination campaign. This is in line with Manyazewal T, 2017 assertion that “a well-performing health workforce is one that works in responsive ways, fair and efficient to achieve the best health outcomes possible, given available resources and circumstances” in his survey of using health care professionals to determine performances of public health facilities in Ethiopia [19].
The staggering of the campaign helped to minimize the shortage of health workers which as reported by Akwataghibe, et al in their 2019 study is one of the major barriers to immunization services while exploring factors influencing immunization utilization in Nigeria. The study stated clearly “Health workforce shortage was a frequently mentioned problem which hindered immunization service delivery” [20].
Our study has shown that there was shortage of both qualified health workers and cold chain equipment to reach the target population for the duration of the campaign and this was mitigated by the staggering approach adopted in the 2018 MVC in Lagos state.
The outcome of the 2018 measles vaccination campaign in Lagos was positive as there was a marked improvement in the postcampaign coverage survey result of 59.3% in 2013, 88% in 2016 and 94% in 2018 [21-23]. Other innovations could have contributed to the improvement in the coverage but we believe the ability to reach most of the targeted children as evidenced by the end process monitoring data that shows less than 5% of the children were missed in all the LGAs could only have been possible because of the mitigation of a major gap in human resources and CCEs by the staggering approach adopted by the state.
Limitations
The staggering plan in Lagos showed some limitations, especially with the link to the Phase 2 LGAs as some phase 1 LGAs were reluctant to deploy the total qualified staff needed to support the phase 2 LGAs as they were continuing with mop-up vaccination. The mop-up vaccination became necessary following the results of the end-process monitoring in their respective wards and the rapid convenience monitoring carried out by the National and the State supervisors. This was done because the State Government was following up on all the actions on daily basis and any failure was said to be sanctioned [24,25]. This made the phase 2 LGAs to carry the vaccination exercise for a longer period and the campaign was completed only after three weeks as they were pushed to the extreme to achieve good results. Similarly, there was no standardized way of selecting the qualified health workers that were deployed to carry out routine services during instead of taking part in the campaign as the routine immunization work going on that same time did not attract any extra stipend so there may be bias in selection across the various LGAs.
Finally, the improvement in the performance of the 2018 campaign in Lagos state when compared to the previous campaigns of 2013 and 2015/2016 may not be entirely due to the staggering alone as such the result should be interpreted with caution. In the same vein, the methodologies used in the post-campaign coverage survey for 2013, 2015/2016 were different and comparing the coverage is a limitation of the study.
Conclusion
The study found that Lagos state leveraged the staggering approach of the campaign to bridge the human and materials resource gaps to implement a quality measles vaccination campaign. The result also provides supporting evidence to highlight the staggering approach as being effective in addressing human resources and CCE gaps, especially in resource-limited areas. We recommend that considering the human resource for health gaps in most lower and middle-income countries, staggering should be considered when planning their supplemental immunization activities.
Credit Authorship Contribution Statement
Chimaobi Ihebuzor: Conceptualization, Methodology, Formal analysis, Writing – Original draft, Writing – Review and editing, Visualization – Tables and figures. Joseph Oteri: Conceptualization, Methodology, Formal analysis, Writing – Original draft, Writing – Review and editing, Visualization – Tables and figures. Boubacar Dieng: Conceptualization, Methodology, Writing – Review and editing. Samuel Bawa: Conceptualization, Methodology, Writing – Review and editing, Visualization – Tables and figures. Adejoke Oladele Kolawole: Conceptualization, Methodology, Writing – Review and editing. Bolanle Orefejo: Conceptualization, Methodology, Writing – Review and editing, Visualization – Tables and figures. Anne Eudes Jean Baptiste: Conceptualization, Methodology, Writing – Review and editing, Visualization – Tables and figures. Nneka Onwu: Review and editing, Validation.
Acknowledgments
We wish to acknowledge the immense support of the State primary health care board and all the Partners that supported the 2018 measles vaccination campaign in Lagos state. Our appreciations also go to the vaccination team members and the community for their immense contributions towards the successful implementation of the Measles vaccination campaign. We also acknowledge Jude Asolo (UNICEF) and Sam Ibizugbe (CHAI) for their wonderful inputs to the development of the states’ staggering maps.
Authors’ Contribution
CI, AJO, and SB conceived the study idea and contributed to the study design and literature search. CI, AJO, BD, SB, AOK, BO, AEJB, and NO contributed to data collection, preparation of figures and tables, and performed the analysis. All contributed to interpretation and writing.
Research Data for this Article
Some of the data sets used in this paper are publicly available via the sources referenced in the manuscript. Other data was generated as part of the activities supporting the measles elimination strategy and SIA. The datasets analysed during the current study are available in the folder (Lagos state measles 2017/2018 microplan data) https://drive.google.com/drive/ folders/1t6lFW9XmcRCjwm9OHJGrX--c-fsSFLzl?usp=sharing
The data set contains the Lagos state and the twenty Local Government Areas microplans and the daily call-in data that was used to derive the administrative coverage used in the analysis.
Funding
This research was part of the documentation of the best practices from the 2018 Measles vaccination campaign and did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- World Health Organization (2012) African Regional MeaslesElimination Strategic Plan (2012-2020). 1-45 p.
- UNDP: Transforming Our World: the 2030 Agenda for Sustainable
- Postolovska I, Helleringer S, Kruk ME, Verguet S (2018) Impact of measles supplementary immunization activities on utilization of maternal and child health services in low-income and middle-income countries BMJ Glob Health 3: e000466.
- FMOH (2011) Comprehensive EPI Multi-year plan 2011 – 2015.
- Nigeria: WHO and UNICEF estimates of immunization coverage: 2020
- National Bureau of Statistics Nigeria - Multiple Indicator Cluster Survey/National Immunization Coverage Survey 2016-17, Fifth round (MICS) and NICS (third Round).
- Pinkbook: Measles | CDC.
- WHO AFRO Region (2011) Resolution. Measles Elimination by 2020: A Strategy for the African Region.
- Masresha BG, Braka F, Onwu NU, Oteri J, Erbeto T, et al. (2018) Progress Towards Measles Elimination in Nigeria: 2012-2016. J Immunol Sci 135-139.
- KIT Royal Tropical Institute and The Society for Family Health (2018) Measles campaigns and their effects on the overall immunization
- Momoh J, Oteri AJ, Mogekwu F, Onwu N, Dieng B, et al. (2021) Ensuring accountability in implementation of supplementary immunisation activities: A case study of the 2017/2018 measles vaccination campaign in Nigeria. Vaccine 39: C12-C20.
- National Population Commission (2007) Population Estimates 20072018.
- World Health Organization (2009) Microplanning for immunization service delivery using the Reaching Every District (RED) strategy. World Health Organization African Regional Office.
- World Health Organization (2016) Planning and implementing highquality supplementary immunization activities for injectable vaccines using an example of measles and rubella vaccines: a field guide.
- Hamisu M, Dieng B, Taiwo L, Jean Baptiste AE, Bawa S, et al. (2021) Microplanning verification and 2017/2018 measles vaccination campaign in Nigeria: Lessons learnt. Vaccine 39: C46-C53.
- FMOH, NPHCDA 2017/2018 Measles Vaccination Campaign Field
- Nigeria 2017 EVM assessment report (2017) Findings and recommendations.
- Ojo TO, Ijadunola MY, Adeyemi EO, Adetunji OO, Adurosakin FO, et (2019) Challenges in the logistics management of vaccine cold chain system in Ile-Ife, Osun State, Nigeria. Journal of Community Medicine and Primary Health Care 31: 1-12.
- Manyazewal T (2017) Using the World Health Organization health system building blocks through survey of healthcare professionals to determine the performance of public healthcare facilities. Arch Public Health 75: 50.
- Akwataghibe NN, Ogunsola EA, Broerse JEW, Popoola OA, Agbo AI, et al. (2019) Exploring Factors Influencing Immunization Utilization in Nigeria-A Mixed Methods Study. Front Public Health 7: 392.
- National Primary Health Care Development Agency (2014) Integrated measles Campaign Coverage survey-Final report.
- National Primary Health Care Development Agency & Partners 2016 Measles Vaccination coverage survey - Final technical report Abuja Nigeria.
- National Bureau of Statistics, National Primary Health Care Development Agency 2018 Post Measles Campaign Coverage Survey Main Survey Report Abuja Nigeria.
- Anugwalu CE, Oteri AJ, Bawa S, Dieng B, Jean Baptiste AE, et al. (2022) The effect of using Open Data Kit for Rapid Convenience Monitoring to guide 2017/2018 measles vaccination campaign Nigeria: a case study of Lagos state. Ann Vaccines Immunization 6: 1019.
- Mogekwu FI, Oteri JA, Nsubuga P, Ezebilo O, Maxwell N, et al. (2021) Using data to improve outcomes of supplemental immunisation activities: 2017/2018 Nigeria measles vaccination campaign. Vaccine 39: C38-C45.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.