Attitudes and Practices of Healthcare Providers Before and After Training on The Prevention of Mistreatment in Gynecology and Obstetrics Units in Guinea
by Moussa Camara1*, Kaba Saran Keita1, Sadan Camara1, Alpha Oumar Sall1, Madeleine Toure1, Fanta Barry1, Ibrahima Sory Conte2, Ida Ndione3, Tiany Sidibe1, Aïssatou Diallo1, Mamadou Diouldé Balde1
1Centre for Research in Reproductive Health in Guinea (CERREGUI), Conakry, Guinea
2Gamal Abdel Nasser University of Conakry, Guinea 3Amref Health Africa, West Africa Office, Dakar
*Corresponding author: Moussa Camara, Centre for Research in Reproductive Health in Guinea (CERREGUI), Conakry, Guinea.
Received Date: February 24, 2026
Accepted Date: March 05, 2026
Published Date: March 12, 2026
Citation: Camara M, Keita KS, Camara S, Sall AO, Toure M, et al. (2026) Attitudes and Practices of Healthcare Providers Before and After Training on The Prevention of Mistreatment in Gynecology and Obstetrics Units in Guinea. J Preg Child Health 7: 127. DOI: https://doi.org/10.29011/2998-2405.100027
Abstract
Context: Mistreatment of women in gynecology and obstetrics services can lead to adverse outcomes for women and new-borns and may discourage patients from seeking healthcare. The objective of this study is to evaluate the impact of training healthcare providers on their attitudes and practices in gynecology and obstetrics services in Guinea, with the goal of preventing and reducing mistreatment of women. Methods: This was a quasi-experimental comparative study using pre- and post-intervention data on healthcare provider training. A multivariate analysis using logistic regression was performed while controlling for confounding variables. A total of 220 healthcare providers were interviewed before and after the intervention, with a nearly identical proportion of female providers in both phases. Results: The multivariate analysis assessed the effect of training on healthcare providers’ attitudes and practices. In terms of healthcare provider practices, the training resulted in a statistically significant reduction in the overall risk of mistreatment of women, with a 6% reduction in gynecology services (RR = 0.94; 95% CI: [0.88–0.99]) and a 15% reduction in obstetrics services (RR = 0.85; 95% CI: [0.80–0.90]).
Conclusion: This study highlighted that training healthcare providers can influence their attitudes and practices but is not sufficient on its own to prevent and combat mistreatment in gynaecology and obstetrics services in Guinea. Hence the need to support this training with a comprehensive strengthening of the healthcare system in order to guarantee maternal care that respects women’s rights and dignity.
Keywords: Attitudes, practices, mistreatment, gynecology, obstetrics, Guinea.
Introduction
Mistreatment constitutes a form of gender-based violence that affects women of reproductive age when they access health services. According to the World Health Organization (WHO) and the United Nations, mistreatment includes physical and verbal abuse, lack of respect for autonomy and consent, discrimination, neglect, and failure to meet professional standards in the provision of gynecological, obstetric, family planning, and reproductive health services [1,2]. Since 2015, the WHO has used the term “mistreatment” rather than “obstetric violence” [3].
The magnitude of this problem is considerable. Globally, estimates of the prevalence of mistreatment, range from 50% to 55%, with significant regional variations [4]. In West and Central Africa, a systematic review estimated that 44% of women experienced mistreatment during childbirth in health facilities [5]. More recent country-specific data indicate even higher rates, with 65% of women in Ghana in 2023, 77% in South Sudan in 2018, and 47% of women in the East African region in 2023 reporting at least one form of mistreatment during childbirth [6–8].
In Guinea, available data indicate that women of reproductive age face significant barriers to accessing respectful maternal care [9,10]. These barriers include not only structural and economic constraints but also healthcare practices that fail to respect women’s rights. Mistreatment in gynecology and obstetrics therefore remains a major public health and human rights issue, undermining the quality of care and women’s trust in the healthcare system. A situational analysis conducted in 2023 documented a high prevalence and wide range of mistreatment, including physical, verbal, and psychological mistreatment [11–13]. The findings of this analysis led to the implementation of an intervention between 2023 and 2024 focusing on training healthcare providers and community health workers. The objective of this study is to evaluate the effect of training healthcare providers on their attitudes and practices in gynaecology and obstetrics services in Guinea in order to prevent and reduce the mistreatment of clients.
Methods
Study Design
This was a quasi-experimental pre- and post-intervention study. Pre-intervention data were collected through a situational analysis, the results of which have been published [11–13]. This analysis informed the design and implementation of the intervention. Postintervention data were collected in the same prefectures included in the situational analysis.
Description of the Intervention
It focused on training healthcare providers and community health workers/community relays, followed by field implementation at the client level in gynecology and obstetrics services carried out by healthcare providers.
The training covered the identification and description of mistreatment in gynecology and obstetrics, the role of healthcare providers in preventing and addressing mistreatment, and the establishment of a patient complaint mechanism. Particular emphasis was placed on women’s sexual and reproductive health rights.
Study Framework
General Framework
Guinea is a West African country covering an area of 245,857 km², with an estimated population of approximately 14,800,836 as of January 1, 2025 [14]. In 2018, about 44% of the population lived below the poverty line [15]. The proportion of women who gave birth in a health facility was 53%, compared with 47% who gave birth at home [16].
The Guinean healthcare system is organized into three levels: primary, secondary, and tertiary. The primary level includes 407 health facilities overseeing 1,640 health posts [17], supported by community health workers involved in awareness campaigns, primary malaria care, and vaccination activities. The secondary level consists of 25 prefectural hospitals, eight regional hospitals, and six communal medical facilities in Conakry. The tertiary level comprises three national hospitals, all operating within a decentralized health district system [17].
Specific Setting
The study was conducted in five prefectures representing Guinea’s four natural regions: Boké (Lower Guinea), Labé and Dabola (Middle Guinea), Faranah (Upper Guinea), and Guéckédou (Forest Guinea). These prefectures were selected due to their diverse geographical and socio-economic characteristics.
In each prefecture, the study was carried out in one regional or prefectural hospital, one urban health facility, and one rural health facility.
Study Population
The study population consisted of healthcare providers working in the gynecology and obstetrics departments of the selected health facilities, including physicians, midwives, nurses, and health technicians.
Sample Size and Sampling
The sample included 109 healthcare providers during the baseline situational analysis and 111 providers after the intervention, for a total of 220 healthcare providers. In each prefecture, the regional or prefectural hospital and the rural health facility were selected purposively, while the urban health facility was selected randomly using a random number generator.
Data Collection Techniques and Tools
Data were collected using structured questionnaires administered face-to-face by trained interviewers. The questionnaires were configured on tablets using KoboCollect software. They covered sociodemographic characteristics, attitudes toward respectful care (including consent, discretion, and complaint handling), selfreported practices and knowledge related to mistreatment, and previous training on respectful care.
Operational Definitions of Variables
Dependent Variables
- Any abusive practice or form of violence affecting women during interactions with health services (physical violence, verbal violence, or other forms of abuse), reported before and after the intervention.
- Reported cases of physical mistreatment (e.g., tying, slapping, hitting, applying abdominal pressure, or painful gynecological examinations).
- Reported cases of verbal mistreatment (e.g., yelling, scolding, insults, mocking, negative remarks, or threats).
- Other reported abusive practices (e.g., lack of consent, lack of discretion, stigmatization, breaches of confidentiality, poor communication, lack of pain management, neglect, lack of autonomy, or informal payments).
Independent Variables
Provider characteristics, including age, sex, education level, profession, type of health facility, years of professional experience, and previous training.
Statistical Analysis
Data were transferred from the tablets to Stata software for cleaning and analysis. Descriptive analyses were conducted using absolute and relative frequencies for categorical variables. Comparisons between pre- and post-intervention phases were performed using Pearson’s chi-square (χ²) test. Multivariate logistic regression analyses were conducted to assess the effects of the intervention on healthcare providers’ attitudes and practices while controlling for potential confounding variables. The intervention effect was evaluated using four main indicators: overall mistreatment, physical violence, verbal violence, and other forms of violence. Risk ratios (RR) and 95% confidence intervals were calculated, with statistical significance set at p < 0.05.
Ethical Considerations
The study was approved by the National Ethics Committee for Health Research of Guinea (Approval No. 162/CNERS/21, November 1, 2021). Written informed consent was obtained from all participants. Confidentiality and anonymity were strictly maintained.
Results
This analysis examined healthcare providers’ attitudes and practices before and after training aimed at preventing and reducing mistreatment of women in gynecology and obstetrics services.
Sociodemographic Characteristics
Table 1 presents the sociodemographic characteristics of the 220 healthcare providers. The proportion of providers under 30 years of age was higher in the post-intervention phase, while the 30–34 age group was more represented in the baseline phase. Female providers predominated in both phases, accounting for 84% before and approximately 86% after the intervention. Vocational training was the most common education level (80.7% before and 86.5% after), and more than two-thirds of providers were midwives (68.8% before and 74.8% after).
|
Sociodemographic characteristics |
Before Intervention (Situational Analysis) |
After Intervention (Post-Experimentation Research) |
P.value |
||||||
|
Hospital (n=80) |
HC*Urban Health Center (n=20) |
HC*Rural Health Center (n=9) |
Total (N=109) |
Hospital (n=81) |
HC*Ur- ban Health Center (n=20) |
HC* Rural Health Center (n=10) |
Total (n-111) |
||
|
Age (in year) |
0,715 |
||||||||
|
Less than 30 years |
13 |
5 |
2 |
20 (18,3) |
21 |
5 |
4 |
30 (27,1) |
|
|
30 - 34 years |
22 |
6 |
3 |
31 (28,4) |
16 |
6 |
4 |
26 (23,4) |
|
|
35 - 39 years |
16 |
2 |
1 |
19 (17,4) |
16 |
5 |
1 |
22 (19,8) |
|
|
40 - 44 years |
16 |
3 |
3 |
22 (20,2) |
14 |
4 |
1 |
19 (17,1) |
|
|
45 years and more |
13 |
4 |
0 |
17 (15,6) |
14 |
0 |
0 |
14 (12,6) |
|
|
Sex |
0,848 |
||||||||
|
Male |
14 |
2 |
1 |
17 (15,6) |
13 |
2 |
1 |
16 (14,4) |
|
|
Female |
66 |
18 |
8 |
92 (84,4) |
68 |
18 |
9 |
95 (85,6) |
|
|
Level of Education |
0,122 |
||||||||
|
Secondary |
5 |
0 |
0 |
5 (4,6) |
0 |
0 |
0 |
0 |
|
|
Voccational |
60 |
19 |
9 |
88 (80,7) |
66 |
20 |
10 |
96 (86,5) |
|
|
Higher Education |
12 |
1 |
0 |
13 (11,9) |
11 |
0 |
0 |
11 (9,9) |
|
|
Postgraduate |
3 |
0 |
0 |
3 (2,8) |
4 |
0 |
0 |
4 (3,6) |
|
|
Profession |
< 0,001 |
||||||||
|
Doctor |
15 |
0 |
0 |
15 (13,8) |
15 |
0 |
0 |
15 (13,5) |
|
|
Midewife |
59 |
13 |
3 |
75 (68,8) |
63 |
13 |
7 |
83 (74,8) |
|
|
Nurse |
4 |
3 |
4 |
11 (10,1) |
2 |
2 |
1 |
5 (4,5) |
|
|
Health Technical Agent (ATS) |
2 |
4 |
2 |
8 (7,3) |
1 |
5 |
2 |
8 (7,2) |
|
|
Years of experience in gynecology and obstetrics services |
0,831 |
||||||||
|
Less than 5 years |
13 |
4 |
3 |
20 (18,3) |
23 |
5 |
2 |
30 (27,0) |
|
|
5-9 years |
30 |
9 |
3 |
42 (38,5) |
18 |
8 |
4 |
30 (27,0) |
|
|
10-14 years |
19 |
3 |
2 |
24 (22,0) |
18 |
4 |
3 |
25 (22,6) |
|
|
15-19 years |
10 |
2 |
1 |
13 (11,9) |
13 |
3 |
1 |
17 (15,3) |
|
|
20 years and more |
8 |
2 |
0 |
10 (9,2) |
9 |
0 |
0 |
9 (8,1) |
|
|
Total number of years worked in the current Department |
0,617 |
||||||||
|
Less than 5 years |
25 |
8 |
7 |
40 (36,7) |
29 |
9 |
6 |
44 (39,6) |
|
|
5-9 years |
38 |
9 |
1 |
48 (44,0) |
33 |
9 |
2 |
44 (39,6) |
|
|
10-14 years |
12 |
2 |
1 |
15 (13,8) |
12 |
1 |
2 |
15 (13,5) |
|
|
15 years and more |
5 |
1 |
0 |
6 (5,5) |
7 |
1 |
0 |
8 (7,3) |
|
Table 1 : Sociodemographic characteristics of healthcare providers.
Attitudes and Practices of Healthcare Providers
Attitudes of Healthcare Providers
Consent before Gynecological or obstetric examinations
The proportion of women who provided consent before examinations increased from 74% before the intervention to 78.4% afterward, although this difference was not statistically significant (Table 2).
Discretion during consultations or care
Reported discretion during gynecological or obstetric consultations increased slightly from 92.7% to 95.5% after the intervention (Table 2).
|
Consent |
Before Intervention (Situational Analysis) |
After Intervention (Post-Experimentation Research) |
P.value |
||||||
|
Hos- pital (n=80) |
HC *Urban Health Center (n=20) |
HC *Ru- ral Health Center (n=9) |
Total (N=109) |
Hospital (n=81) |
HC *Urban Health Center (n=20) |
HC *Rural Health Center (n=10) |
Total (N=111) |
||
|
Do you ask for a woman’s consent before performing a gynecological or obstetric examination? |
0,911 |
||||||||
|
Never |
1 |
0 |
0 |
1 (0,9) |
0 |
0 |
0 |
0 |
|
|
Rarely |
3 |
0 |
0 |
3 (2,8) |
0 |
0 |
0 |
0 |
|
|
Often |
18 |
4 |
2 |
24 (22,0) |
16 |
6 |
2 |
24 (21,6) |
|
|
Always |
58 |
16 |
7 |
81 (74,3) |
65 |
14 |
8 |
87 (78,4) |
|
|
Discretion |
Before Intervention (Situational Analysis) |
After Intervention (Post-Experimentation Research) |
P.value |
||||||
|
Hos- pital (n=80) |
HC* Urban Health Centre urbain (n=20) |
HC* Rural Health Centre (n=9) |
Total (N=109) |
Hospital (n=81) |
HC* Urban Health Centre (n=20) |
HC* Rural Health Centre (n=10) |
Total (N=111) |
||
|
Do you ensure discretion during a consultation or care in gynecology or obstetrics? |
0,384 |
||||||||
|
Yes |
72 |
20 |
9 |
101 (92,7) |
78 |
19 |
9 |
106 (95,5) |
|
|
No |
8 |
0 |
0 |
8 (7,3) |
30 |
1 |
1 |
5 (4,5) |
|
Table 2: A woman’s consent before undergoing a gynaecological or obstetric examination.
Complaints, recourse to authorities, and follow-up
The proportion of reported complaints or recourse to authorities decreased from 48.6% before the intervention to 33.3% afterward, without statistical significance. However, apologies by providers decreased from 98.1% to 75.5%, while the intention to prevent recurrence remained stable at 24.5%. Most complaints were not acted upon in either phase (90.5% before and 97.3% after) (Table 3).
|
Before Intervention (Situational Analysis) |
After Intervention (Post-Experimentation Research) |
P.value |
|||||||
|
Hospital (n=80) |
HC* Urban Health centre (n=20) |
HC* Rural Health Centre (n=9) |
Total (N=109) |
Hospital (n=81) |
HC* Urban Health Centre (n=20) |
HC* Rural Health Centre (n=10) |
Total (N=111) |
||
|
Have you ever had a patient complain about your actions during a gynecological or obstetric examination (examples: vaginal examination, vaginal swab, end-vaginal ultrasound, episiotomy, instrumental extraction)? |
|||||||||
|
Yes |
42 |
8 |
3 |
53 (48,6) |
27 |
5 |
5 |
37 (33,3) |
|
|
No |
38 |
12 |
6 |
56 (51,4) |
54 |
15 |
5 |
74 (66,7) |
|
|
Accuracy of the examination in question |
0,310 |
||||||||
|
vaginal examination |
31 |
7 |
3 |
41 (77,4) |
19 |
4 |
3 |
26 (36,1) |
|
|
Episiotomy |
29 |
2 |
0 |
31 (58,5) |
20 |
2 |
2 |
24 (33,3) |
|
|
vaginal swab |
3 |
1 |
0 |
4 (7,5) |
7 |
0 |
0 |
7 (9,7) |
|
|
Instrumental extraction |
6 |
0 |
0 |
6 (11,3) |
11 |
0 |
2 |
13 (18,1) |
|
|
Reaction from health care providers |
0,987 |
||||||||
|
To apologize |
42 |
7 |
3 |
52 (98,1) |
27 |
5 |
5 |
37 (75,5) |
|
|
To prevent this from hap- pening again |
10 |
2 |
1 |
13 (24,5) |
8 |
2 |
2 |
12 (24,5) |
|
|
Hospital (n=42) |
HC* Urban Health Centre (n=8) |
HC* Rural Health Centre (n=3) |
Total (N=53) |
Hospital (n=27) |
HC* Urban Health Centre (n=5) |
HC* Rural Health Centre (n=5) |
Total (N=37) |
||
|
Complaint’s Effect |
0,624 |
||||||||
|
None |
37 |
8 |
3 |
48 (90,5) |
0 |
0 |
0 |
0 |
|
|
Warning |
4 |
0 |
0 |
4 (7,5) |
1 |
0 |
0 |
1 (100) |
|
Table 3: Patient complaint and subsequent actions according to service providers.
Healthcare Provider Practices
Frequency of mistreatment in gynecology and obstetrics
Self-reported mistreatment by healthcare providers decreased significantly between the two phases. In gynecology services, reported mistreatment declined from 40.4% to 17.1%, and in obstetrics services, from 53.2% to 16.2%.
However, in rural areas, mistreatment persisted, particularly in gynecology (40%). (Figure 1).
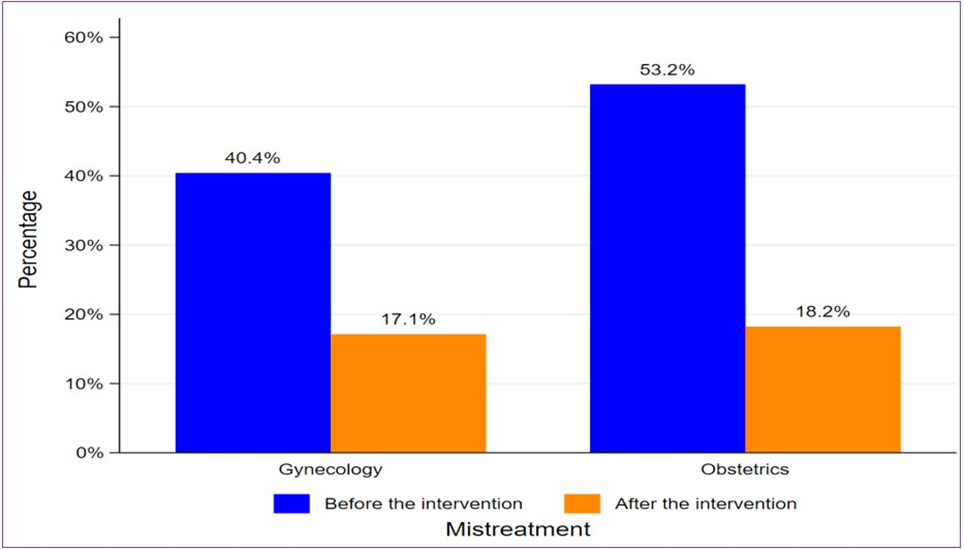
Figure 1: Overall Frequency of Mistreatment in Gynecology and Obstetrics Services in Guinea according to Providers.
Types of Mistreatments in Gynecology According to Healthcare Providers
Based on the types of mistreatments in gynecology reported by healthcare providers between the two periods, we observed a significant decrease (P-value=0.035) in verbal abuse after the procedure, from 75% to 42.1%. However, physical abuse increased from 13.6% to 36.8%, although this increase was not statistically significant (Figure 2).
Types of Mistreatments in Obstetrics According to Healthcare Providers
In obstetrics, verbal abuse also decreased significantly (P-value=0.002), from 69% before to 38.9% after the procedure. In contrast, physical abuse increased from 24.1% to 39%, but this difference was not statistically significant. (Figure 2).
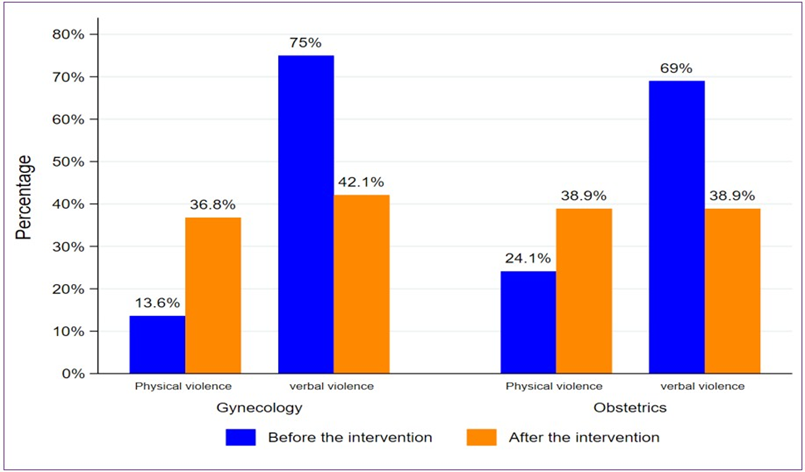
Figure 2: Types of mistreatments in gynecology and obstetrics services in Guinea according to healthcare providers.
Effects of Healthcare Provider Training on Reducing Mistreatment in Healthcare Facilities
Four main indicators were used to assess the impact of the intervention: overall mistreatment, physical violence, verbal violence, and other forms of violence. Multivariate analysis enabled an assessment of the intervention’s impact by service category.
In gynecology, the intervention resulted in a statistically significant 6% reduction in the overall risk of mistreatment (P = 0.033; RR = 0.94; 95% CI: [0.88–0.99]). No significant effect was observed for physical violence (RR = 1.03; 95% CI: [0.96–1.09]). However, the intervention had a positive and significant effect on verbal abuse, with a 17% reduction in risk (P < 0.001; RR = 0.83; 95% CI: [0.76– 0.90]). No statistically significant effect was observed for other forms of abuse (RR = 0.91; 95% CI: [0.83–1.00]) (Table 4).
|
Physical violence |
Before Intervention (Situational Analysis) |
After Intervention (Post-Experimentation Research) |
P.value |
||||||
|
Hos- pital (n=4) |
HC* Urban Health Centre (n=1) |
HC* Rural Health Centre (n=1) |
Total (N=6) |
Hos- pital (n=4) |
HC* Urban Health Centre (n=1) |
HC* Rural Health Centre (n=2) |
Total (N=7) |
||
|
Gynecology |
|||||||||
|
Tie down |
2 |
0 |
0 |
2 (33 ,3) |
0 |
0 |
0 |
0 |
0,095 |
|
Slap |
1 |
0 |
1 |
2 (33 ,3) |
0 |
1 |
0 |
1 (14,3) |
0,118 |
|
Beat |
3 |
1 |
1 |
5 (83,3) |
0 |
0 |
0 |
0 |
0,080 |
|
Apply pressure to the abdomen |
3 |
1 |
0 |
4 (66,7) |
3 |
0 |
1 |
4 (57,1) |
0,473 |
|
Painful gynecological exam |
1 |
0 |
0 |
1 (16,7) |
3 |
0 |
1 |
4 (57,1) |
0,472 |
|
Physical violence |
Hospital (9) |
HC* Urban Health Centre (3) |
HC* Rural Health Centre (2) |
Total (14) |
Hospital (5) |
HC* Urban Health Centre (0) |
HC* Rural Health Centre (2) |
Total (7) |
P.value |
|
Obstetrics |
|||||||||
|
Tie down |
1 |
0 |
0 |
1 (7,1) |
0 |
0 |
0 |
0 |
0,134 |
|
Slap |
0 |
2 |
1 |
3 (21,4) |
0 |
0 |
0 |
0 |
0,022 |
|
Beat |
1 |
1 |
1 |
3 (21,4) |
1 |
0 |
0 |
1 (14,3) |
0,648 |
|
Apply pressure to the abdomen |
7 |
2 |
1 |
10 (71,4) |
1 |
0 |
1 |
2 (28,6) |
0,334 |
|
Painful gynecological exam |
4 |
0 |
0 |
4 (28,6) |
2 |
0 |
0 |
2 (28,6) |
0,376 |
|
Verbal abuse |
Before Intervention (Situational Analysis) |
After Intervention (Post-Experimentation Research) |
P.value |
||||||
|
Hos- pital (n=28) |
HC* Urban Health Centre (n=4) |
HC* Rural Health Centre (n=1) |
Total (N=33) |
Hos- pital (n=5) |
HC* Urban Health Centre (n=1) |
HC* Rural Health Centre (n=2) |
Total (N=8) |
||
|
Gynecology |
|||||||||
|
Shout |
24 |
4 |
1 |
29 (87,9) |
3 |
0 |
1 |
4 (50,0) |
0,138 |
|
Scold |
17 |
0 |
0 |
17 (51,5) |
3 |
1 |
1 |
5 (62,5) |
0,199 |
|
Insult |
8 |
2 |
0 |
10 (30,3) |
2 |
0 |
0 |
2 (25,0) |
0,735 |
|
mock |
1 |
0 |
0 |
1(3,0) |
0 |
0 |
0 |
0 |
0,993 |
|
Negative remarks about the woman |
7 |
0 |
1 |
8 (24,2) |
5 |
0 |
0 |
5 (62,5) |
0,005 |
|
Threaten |
3 |
0 |
0 |
3 (9,1) |
1 |
0 |
0 |
1 (12,5) |
0,914 |
|
Other |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
1 (12,5) |
0,180 |
|
Obstetrics |
|||||||||
|
Shout |
32 |
5 |
1 |
38 (95,0) |
2 |
2 |
2 |
6 (85,7) |
0,340 |
|
Scold |
14 |
1 |
0 |
15 (37,5) |
1 |
1 |
1 |
3 (42,9) |
0,805 |
|
Insult |
8 |
4 |
0 |
12 (30,0) |
1 |
0 |
0 |
1 (14,3) |
0,243 |
|
mock |
2 |
1 |
0 |
3(7,5) |
0 |
0 |
0 |
0 |
0,900 |
|
Negative remarks about the woman |
3 |
1 |
0 |
4 (10,0) |
1 |
0 |
1 |
2 (28,6) |
0,473 |
|
Threaten |
2 |
0 |
0 |
2 (5,0) |
0 |
0 |
0 |
0 |
0,971 |
Table 4: Forms of physical violence in gynecology and obstetrics according to healthcare providers.
In obstetrics, a significant 15% decrease in the overall risk of mistreatment was observed after the intervention (P < 0.001; RR = 0.85; 95% CI: [0.80–0.90]), according to providers. No statistically significant effect was observed for physical violence at the 5% significance level (RR = 0.93; 95% CI: [0.87–1.00]). In contrast, the intervention had a strong and significant effect on verbal violence, with a 20% reduction in risk (P < 0.001; RR = 0.80; 95% CI: [0.73–0.87]). A significant 11% reduction in the risk of other forms of violence was also reported (RR = 0.89; 95% CI: [0.81–0.98]) (Table 5).
|
Gynecology |
||||
|
Mistreatment |
Physical violence |
Verbal abuse |
Other types of violence |
|
|
Intervention (before and after) |
RR = 0,94 [0,88-0,99] P = 0,033 |
RR = 1,03 [0,96-1,09] P = 0,380 |
RR = 0,83 [0,76-0,90] P < 0,001 |
RR = 0,91 [0,83-1,00] P = 0,054 |
|
Confounding variables |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
|
Obstetrics |
||||
|
Mistreatment |
Physical violence |
Verbal abuse |
Other types of violence |
|
|
Intervention (before and after) |
RR = 0,85 [0,80-0,90]; P < 0,001 |
RR = 0,93 [0,87-1,00]; P = 0,064 |
RR = 0,80 [0,73-0,87]; P < 0,001 |
RR = 0,89 [0,81-0,98]; P = 0,020 |
|
Confounding variables |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Age, sex, education, profession, healthcare facility, years of experience, years of work, attendance |
Table 5: Effects of the intervention on violence/mistreatment in gynecology according to healthcare providers.
Discussion
This quasi-experimental study, conducted in five prefectures of Guinea, aimed to evaluate the impact of a healthcare provider training intervention on attitudes and practices in gynecology and obstetrics services, with the objective of preventing and reducing mistreatment of women. The findings indicate that the frequency of mistreatment, as reported by providers, decreased significantly between the pre- and post-intervention periods in both services, declining from 40.4% to 17.1% in gynecology and from 53.2% to 16.2% in obstetrics.
The results also demonstrate improvements in respect for informed consent and confidentiality during care, although the persistence of certain mistreatment behaviors particularly in rural areas—remains concerning. Verbal mistreatment declined significantly in both services following the intervention: from 75% before the intervention to 42.1% after in gynecology, and from 69% to 38.9% in obstetrics. Physical mistreatment, however, did not show a statistically significant reduction. Overall, the intervention led to a significant reduction in the risk of mistreatment, estimated at 6% in gynecology and 15% in obstetrics.
These findings are consistent with existing evidence on the effectiveness of training interventions in promoting respectful care [2,4,18,19]. The observed reduction in mistreatment may be explained by increased awareness among providers of respectful maternal care principles and patients’ rights, fostered through targeted training.
Our results align with several African and international studies demonstrating the effectiveness of continuing education programs in improving the quality of obstetric and gynaecological care. For instance, a study conducted at Injibara General Hospital in northwest Ethiopia reported a 55.9% reduction in disrespect and mistreatment during antenatal care and delivery (from 71.8% at baseline to 15.9% at end line) [20]. Similarly, Tavcar et al., in Iran, reported a significant reduction in overall mistreatment scores following structured training of maternity care teams, with a decrease of more than 17 points compared to the control group [21].
These findings suggest that targeted training influences not only healthcare providers’ knowledge but also their attitudes and clinical practices, resulting in a measurable reduction in mistreatment. Structured educational interventions therefore appear to be effective and reproducible strategies that should be prioritized in national and regional health policies to improve women’s experiences, safety, and dignity in healthcare settings.
The improvement observed in respect for consent and confidentiality during gynecological and obstetric care is consistent with findings from studies conducted in Tanzania [22] and Kenya [23]. Furthermore, research by Sanjida Arora et al. in India indicates that training combined with confidentiality safeguards and systemic mechanisms such as reference materials and standardized care procedures can significantly enhance respect for patients’ rights [24]. These findings highlight the importance of ongoing training and regular supervision in fostering empathetic attitudes and effective communication. Although not always statistically significant, the observed trends underscore the need to sustain and intensify these efforts.
The significant reduction in verbal mistreatment observed in both gynecology and obstetrics in our study corroborates the findings of Bohren et al., who demonstrated the effectiveness of patient-centered interventions in promoting respect and dignity during maternity care [3]. In our study, this reduction may be attributed to improved communication skills, greater awareness of the consequences of disrespectful language, and increased empathy among providers. However, the persistence of physical violence despite the intervention underscores the complexity of mistreatment, as noted by Freedman and Kruk [25], who emphasize the need to address systemic and cultural factors. Training alone appears insufficient to eliminate severe forms of mistreatment that are often rooted in workload pressures, organizational constraints, and entrenched norms [5]. A more comprehensive approach incorporating organizational reforms, standardized protocols, and accountability mechanisms is therefore required.
Strengths and Limitations
This study is the first to focus on mistreatment of women in gynecology departments in Guinea, whereas previous studies only covered obstetrics departments, particularly childbirth. It was conducted in Guinea’s four natural regions across the targeted prefectures. The inclusion of a multivariate analysis controlling for confounding variables also strengthens the validity of the results. However, this study has some limitations, mainly related to the lack of planning for evaluating the sustainability of changes in the attitudes of health care providers toward preventing mistreatment of women who come for gynecological and obstetric consultations and care.
Implications for Practice and Research
The findings have important implications. First, the observed improvements in attitudes toward consent and confidentiality demonstrate that training can positively influence providers’ values regarding patients’ rights. Second, the persistence of physical violence and disparities between facilities, services, and geographic areas indicates that training alone is insufficient. A multi sectoral and integrated strategy is required. At the policy level, mistreatment should be explicitly recognized and addressed within national reproductive health frameworks. Strengthening complaint and redress mechanisms is essential to ensure accountability and justice for victims. Finally, particular attention should be given to rural settings to promote equity in access to respectful care.
Conclusion
This study demonstrates that training healthcare providers has a positive influence on their attitudes and practices regarding the prevention and control of abuse against women in gynecology and obstetrics services in Guinea. However, the results suggest the need to systematically integrate respectful care and abuse prevention into initial and continuing education programs. It is essential to sustain and scale up these interventions, which must be supported by broader measures to strengthen the health system, including staff motivation, adequate equipment and supplies, quality infrastructure, and robust monitoring and evaluation systems. These efforts are essential to ensure maternal health services that respect women’s rights, dignity, and integrity.
Acknowledgements
We would like to express our sincere thanks to the French Development Agency (AFD) for its financial support, which made this study possible. We would also like to express our gratitude to the Amref Health Africa – Centre for Research in Reproductive Health in Guinea (CERREGUI) consortium for the operational implementation of the project and for its ongoing commitment to promoting respectful care and reproductive health rights.
Ethical approval
The study was approved by Guinea’s National Ethics Committee for Health Research under number 162/CNERS/21 on November 1, 2021.
Conflict of interest
The authors declare that they have no conflicts of interest related to the conduct of this study, the analysis of the data, or the writing of the manuscript.
Author contributions
Study design: MDB, MC; data analysis: KSK, SC, MT, FB, AD, and TS; writing: MC, MDB; manuscript revision: MDB, KSK, IC, AOS, IN. Each author confirms that they have read and approved the final version of the manuscript prior to submission.
Data availability
The data used in this study are available from the corresponding authors upon reasonable request. They will be made available in accordance with the ethical requirements and confidentiality procedures defined by the National Ethics Committee for Research.
References
- World Health Organization, Department of Reproductive Health and Research. The prevention and elimination of disrespect and abuse during facility-based childbirth.
- Dubravka S (2019) human rights-based approach to mistreatment and violence against women in reproductive health services with a focus on childbirth and obstetric violence. UN-Note by the SecretaryGeneral.
- Bohren MA, Vogel JP, Hunter EC, Lutsiv O, Makh SK, et al. (2015) The Mistreatment of Women during Childbirth in Health Facilities Globally: A Mixed-Methods Systematic Review. PLoS Med 12(6): e1001847.
- Hakimi S, Allahqoli L, Alizadeh M, Ozdemir M, Soori H, et al. (2025) Global prevalence and risk factors of obstetric violence: A systematic review and meta-analysis. International Journal of Gynecology and Obstetrics. 169(3): 1012-24.
- Kassa ZY, Tsegaye B, Abeje A (2020) Disrespect and abuse of women during the process of childbirth at health facilities in sub-Saharan Africa: A systematic review and meta-analysis. BMC Int Health Hum Rights 20(1).
- Yalley AA, Abioye D, Appiah SCY, Hoeffler A (2023) Abuse and humiliation in the delivery room: Prevalence and associated factors of obstetric violence in Ghana. Front Public Health (11): 988961.
- Altahir A, Alaal AA, Mohammed A, Eltayeb D (2018) Proportion Disrespectful and Abusive Care during Childbirth among Women in Khartoum State-2016. Am J Public Health Res 6(6): 237-42.
- Gebeyehu NA, Adella GA, Tegegne KD (2023) Disrespect and abuse of women during childbirth at health facilities in Eastern Africa: systematic review and meta-analysis. Frontiers in Medicine Vol(10).
- Balde MD, Diallo BA, Bangoura A, Sall O, Soumah AM, et al. (2017) Perceptions and experiences of the mistreatment of women during childbirth in health facilities in Guinea: a qualitative study with women and service providers. Reprod Health 14(1): 1-13.
- Balde MD, Bangoura A, Diallo BA, Sall O, Balde H, et al. (2017) A qualitative study of women’s and health providers’ attitudes and acceptability of mistreatment during childbirth in health facilities in Guinea. Reprod Health 14(1): 1-13.
- Sall AO, Diallo R, Balde MD, Camara S, Kourouma K, et al. (2024) Mistreatment in the gynaecology and obstetrics units of health facilities: community women’s experiences in Guinea. Int J Reprod Contracept Obstet Gynecol 13(5).
- Balde MD, Diallo R, Kourouma K, Keita KS, Sidibe T et al. (2024) Frequency and factors associated with women’s mistreatment in obstetric units in Guinea. Int J Reprod Contracept Obstet Gynecol 14(1): 37-46.
- Diallo R, Balde MD, Kourouma K, Sidibe T, Sall AO, et al. (2024) Mistreatment of women during gynecological care in health facilities in Guinea. Int J Reprod Contracept Obstet Gynecol 14(1): 5-12.
- Country Meters: Guinea population. Available from: https:// countrymeters.info/en/Guinea 2025. [cited 2025 Dec 11].
- World Data Atlas. Guinea Poverty headcount ratio at national poverty line. Available from: https://data.worldbank.org/indicator/SI.POV. NAHC?locations=GN 2025. [cited 2025 Dec 11].
- National Institute of Statistics of Guinea, Demographic and Health Survey. DHS 2018. Republic of Guinea.
- Minister of Health, Health Statistical Yearbook 2017. Republic of Guinea.
- Asefa A, Morgan A, Bohren MA, Kermode M (2020) Lessons learned through respectful maternity care training and its implementation in Ethiopia: An interventional mixed methods study. Reprod Health 17(1):
- Dzomeku VM, Boamah Mensah AB, Nakua EK, Agbadi P, Lori JR, et al. (2021) Midwives’ experiences of implementing respectful maternity care knowledge in daily maternity care practices after participating in a four-day RMC training. BMC 20(1): 39.
- Mihret H, Atnafu A, Gebremedhin T, Dellie E (2020) Reducing disrespect and abuse of women during antenatal care and delivery services at injibara general hospital, Northwest Ethiopia: A pre–post interventional study. Int J Womens Health 12: 835-47.
- Tajvar M, Alipour S, Atashbahar O, Shakibazadeh E, Saeed AS, et al. (2025) Promoting respectful maternity care: a quasi-experimental study on the effectiveness of an educational intervention in Iranian hospitals. Reproductive Health 22(1): 40.
- Kruk ME, Kujawski S, Mbaruku G, Ramsey K, Moyo W (2018) Disrespectful and abusive treatment during facility delivery in Tanzania: A facility and community survey. Health Policy Plan 33(1): e26-33.
- Sando D, Ratcliffe H, McDonald K, Spiegelman D, Lyatuu G, et al. (2016) The prevalence of disrespect and abuse during facility-based childbirth in urban Tanzania. BMC Pregnancy Childbirth 16(1): 236.
- Arora S, Rege S, Bhate-Deosthali P, Thwin SS, Amin A, et al. (2021) 25. Freedman LP, Kruk ME (2014) Disrespect and abuse of women in García-Moreno C, et al. Knowledge, attitudes and practices of health childbirth: Challenging the global quality and accountability agendas. care providers trained in responding to violence against women: a pre- Lancet 384(9948): e42-4. and post-intervention study. BMC Public Health 21(1): 1973.
© by the Authors & Gavin Publishers. This is an Open Access Journal Article Published Under Attribution-Share Alike CC BY-SA: Creative Commons Attribution-Share Alike 4.0 International License. Read More About Open Access Policy.